
Abstract
Background:
The number of rotator cuff repairs (RCRs) is increasing each year. Total shoulder arthroplasty (TSA) is a successful treatment option for patients with glenohumeral osteoarthritis with a functioning rotator cuff.
Purpose/Hypothesis:
The purposes of this study were to report the outcomes of TSA in patients with ipsilateral RCR and determine whether patients with a history of ipsilateral RCR who subsequently underwent TSA had differences in outcomes compared with matched controls who underwent TSA with no history of RCR. We hypothesized that patients with prior RCR will have significant improvements in clinical outcome scores, with no difference in outcomes after TSA compared with those with no prior RCR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients eligible for inclusion were those with a history of prior RCR who underwent TSA at a single institution with a minimum 2-year follow-up between 2000 and 2015. Outcomes for this group, including American Shoulder and Elbow Surgeons (ASES) scores, were reported and then compared with a matched control group of patients who underwent TSA with no history of prior RCR. Controls were matched based on age, sex, and preoperative ASES score.
Results:
Overall, 14 patients (64% males; mean ± SD age, 65.1 ± 11.1 years) underwent prior ipsilateral RCR before TSA. ASES scores significantly improved from 42.9 to 78.5 at 2 years and to 86.6 at 5 years. When compared with 42 matched control patients (matched 1:3) who underwent TSA with no history of RCR, there was no significant difference in ASES scores at 2 years (78.5 vs 85.3; P = .19) and 5 years (86.6 vs 90.9; P = .72) between the prior RCR and no RCR groups.
Conclusion:
TSA in patients with a history of prior ipsilateral RCR led to significant improvements in clinical outcomes. No difference in clinical outcomes at 2 or 5 years after TSA was found between patients with and without a history of prior ipsilateral RCR.
Keywords
As the population continues to age, more patients are suffering from shoulder problems. 4,19 The number of rotator cuff repairs (RCRs) performed each year continues to rise, as more active patients suffer from symptomatic rotator cuff tears. 19 Outcomes after RCR in patients of varying ages have been encouraging, with improvement in clinical outcomes routinely seen despite lack of tendon healing in some patients. 1,3,6 While RCR remains the most common treatment for symptomatic rotator cuff tears that have failed nonoperative treatment, there are some studies 12,22,25 that have suggested reverse total shoulder arthroplasty (RTSA) should be the treatment of choice in older patients with massive rotator cuff tears, even in those who have no evidence of glenohumeral arthritis. While RTSA is an effective procedure for treating pseudoparalysis and rotator cuff tear arthropathy, it is not without its shortcomings—namely, loss of shoulder internal rotation, forward elevation, and others. 8,15
Total shoulder arthroplasty (TSA) has become an effective treatment option for patients suffering from glenohumeral osteoarthritis with an intact, functioning rotator cuff. 5,7,14,17 Compared with RTSA, TSA affords patients a more effective and consistent recovery from pain, shoulder function, and shoulder rotation (specifically internal rotation). 8,15 Prior studies 11,21,23 have found conflicting results as to whether prior ipsilateral RCR affects outcomes after RTSA. No study to date has evaluated the effect of prior ipsilateral RCR on outcomes after TSA. Therefore, the rationale for this study was that even when patients have clinically good outcomes after RCR, retears could be present that may affect the results after TSA. Furthermore, after RCR, the rotator cuff heals with scar tissue that makes repaired tendons more prone to failure in the future. It is currently unclear how this tissue functions after TSA. This study sought to answer these questions.
The purposes of this study were to report the outcomes of TSA after ipsilateral RCR and to determine if patients with a history of ipsilateral RCR who subsequently underwent TSA had differences in outcomes compared with matched controls who underwent TSA with no history of RCR. We hypothesized that patients with prior RCR will have significant improvements in clinical outcome scores, with no difference in outcomes after TSA compared with those with no prior RCR.
Methods
A prospective shoulder arthroplasty registry is maintained at our institution to collect data on all patients undergoing a TSA. After institutional review board approval, a review of this database was conducted to identify all patients who had undergone an ipsilateral RCR before undergoing their TSA between 2000 and 2015. All TSAs were performed by 1 of 6 surgeons (including authors J.S.D., D.M.D., and L.V.G.) at a single institution. Inclusion criteria were patients with any prior RCR (either open or arthroscopic) who subsequently underwent a primary TSA with a minimum of 2 years of follow-up. The exclusion criterion was prior ipsilateral shoulder arthroplasty (either revision TSA or conversion of a hemiarthroplasty to a TSA) or <2 years of follow-up. All TSA procedures were performed through a standard deltopectoral approach. All patients in both the case and the control groups had intact, functioning rotator cuffs based on preoperative physical examination, magnetic resonance imaging (MRI), or computed tomography (CT), as well as intraoperatively under direct visualization at the time of TSA.
The shoulder arthroplasty registry at our institution records both objective and subjective outcomes, all of which were collected for this study. These subjective outcomes include overall patient satisfaction and whether the patient would recommend this surgery to another patient. The objective outcomes include the American Shoulder and Elbow Surgeons (ASES) score, physical component summary (PCS) portion of the 12-Item Short Form Health Survey (SF-12), mental component summary (MCS) portion of the SF-12, and the Shoulder Activity Scale (SAS). Patients are evaluated at regular intervals for the first year and then at the 2- and 5-year postoperative time points.
There were 14 patients in the registry with a history of prior ipsilateral RCR who subsequently underwent TSA. All patients underwent TSA with a cemented, pegged, polyethylene glenoid. A total of 7 patients had a preoperative CT scan and 7 had a preoperative MRI. The rotator cuff demonstrated tendinosis in the supraspinatus in 1 patient, an isolated partial thickness tear of the supraspinatus in 1 patient, a partial thickness tear of the supraspinatus and infraspinatus in 1 patient, and a partial thickness tear of the supraspinatus and infraspinatus with intrasubstance tearing of the subscapularis in 1 patient. Of the 14 patients, 5 had grade I or II Goutallier changes in the supraspinatus based on preoperative imaging.
These 14 patients were then matched 1:3 to a group of control patients who underwent TSA but had no history of prior ipsilateral RCR. Controls were matched based on age (±5 years), sex, and preoperative ASES score (±10 points) (Table 1).
Patient Characteristics a
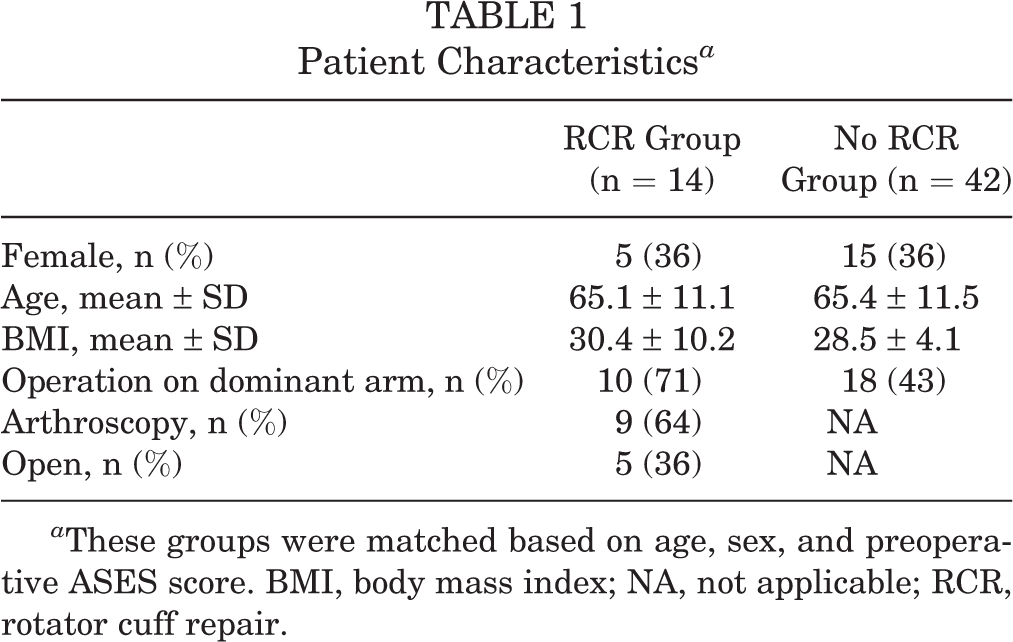
a These groups were matched based on age, sex, and preoperative ASES score. BMI, body mass index; NA, not applicable; RCR, rotator cuff repair.
Statistical Analysis
Continuous variable data were reported as weighted means ± weighted standard deviations. Categorical variable data were reported as frequencies with percentages. For all statistical analyses, either measured and calculated from study data extraction or directly reported from the individual studies, P < .05 was considered statistically significant. We used t tests to compare the 2- and 5-year outcomes between the RCR and non-RCR groups.
Results
Of the 14 study patients (RCR group), 64% were males, and the average age was 65.1 ± 11.1 years. At 2-year follow-up after the TSA, significant improvements were seen in ASES and SF-12 PCS, while no significant difference was seen in SF-12 MCS and SAS (Table 2). All patients had 2 years of follow-up data and 28.5% had 5 years of follow-up data. Two patients developed complications: One patient had persistent anterior instability necessitating a revision of the humeral component, and 1 patient developed a postoperative infection necessitating a 2-stage exchange (an anatomic replacement was reimplanted after a spacer).
2-Year Outcomes for Patients in the RCR Group a

a Bolded values reached statistical significance. ASES, American Shoulder and Elbow Surgeons; MCS, mental component summary portion of the SF-12; PCS, physical component summary portion of the SF-12; RCR, rotator cuff repair; SAS, Shoulder Activity Scale; SF-12, 12-Item Short Form Health Survey.
When RCR group was matched in a 1:3 fashion to a group of controls with no history of ipsilateral RCR (no RCR group; n = 42), there were no significant differences in any of the baseline scores (Table 3). There were no significant differences between the RCR and no RCR groups in any of the measured variables at either the 2- or 5-year follow-up or in complication rates.
2- and 5-Year Outcomes for Patients in the RCR and No RCR Groups a

a These groups were matched on preoperative ASES score. ASES, American Shoulder and Elbow Surgeons; MCS, mental component summary portion of the SF-12; PCS, physical component summary portion of the SF-12; SAS, Shoulder Activity Scale; SF-12, 12-Item Short Form Health Survey.
b Proportion reporting very satisfied or somewhat satisfied.
c Proportion reporting yes, definitely or yes or probably.
Discussion
As the population continues to age, the number of RCRs performed annually is increasing. 19 Similarly, the number of TSA procedures continues to rise. 4 Our study hypotheses were confirmed, as patients with prior RCR who subsequently underwent TSA had significant improvements in clinical outcome scores, with no difference in outcomes after TSA compared with patients with no prior RCR.
This is the first study to date to report comparative outcomes after TSA in patients with and without a history of prior RCR. Previous studies 20,24 have evaluated outcomes after TSA with concomitant RCR and reported good to excellent outcomes in the majority of patients. Interestingly, Ahearn et al 2 reported outcomes after TSA in patients with attenuated or partially torn rotator cuffs and found no difference in outcomes between patients with intact, attenuated, or partially torn rotator cuffs. However, there were no patients with full-thickness rotator cuff tears included in that study. With the increasing number of both RCR and TSA, it is important to understand the effect of one procedure on the other, and based on the results of this study, prior RCR does not have a negative effect on functional outcomes after TSA. 19,26 However, previous work 13 has found RCR after TSA to be an ineffective procedure in the majority of cases. It is important to note that the data from this study indicate similar 2-year postoperative outcomes between patients with a history of RCR before TSA and those without a history of RCR at 2 years. However, given the limited data in 5-year outcomes, it is difficult to definitively conclude there is no difference in outcomes at 5 years because of the possibility of type II error.
There are limited data 26 on the effects of prior shoulder surgery on outcomes after TSA. Werthel et al 26 evaluated 4577 patients who underwent shoulder arthroplasty (18% of whom had previous nonarthroplasty shoulder surgery) and found a significantly higher infection rate (2.4% vs 1.2%) in patients with a history of prior shoulder surgery. Currently, there are no studies that have evaluated the percentage of patients who undergo TSA after having an RCR. We found only 14 patients in our database who met the inclusion criteria between 2000 and 2015. This could indicate that a prior RCR is an uncommon procedure in patients undergoing TSA, or it could be a sampling bias. Prior studies 9,18 have evaluated the critical shoulder angle (CSA), as well as glenoid inclination, and their association with rotator cuff tears versus development of osteoarthritis. Moor et al 18 reported on several groups: 102 shoulders with MRI-documented full-thickness rotator cuff tears without osteoarthritis, 102 shoulders with primary osteoarthritis and no rotator cuff tear noted during TSA, and 94 asymptomatic shoulders with normal rotator cuffs and no osteoarthritis. The authors found that the control group had an average CSA of 33.1°, the group with isolated full-thickness rotator cuff tears had an average CSA of 38°, and the group with isolated osteoarthritis had an average CSA of 28.1°. Hence, it could be that patients with prior rotator cuff tears are less likely to develop osteoarthritis secondary to their anatomy. Regardless of the reason, it is meaningful, as a patient who has a functional rotator cuff after RCR and develops glenohumeral osteoarthritis can possibly undergo a TSA instead of an RTSA.
Prior cost analysis studies 10,16 have found the most cost-effective treatment option for patients with a massive rotator cuff tear is an arthroscopic RCR. Therefore, from a cost perspective, it is better to attempt an RCR in patients with pseudoparalysis and no significant osteoarthritis rather than going straight to an RTSA. Furthermore, it is reassuring that outcomes after TSA are not significantly affected by prior ipsilateral RCR. This information will allow surgeons to properly counsel their patients on the risks and benefits of soft tissue versus arthroplasty procedures, and it provides alternative treatment options for these patients.
Limitations
The patients in this study are from a single institution and were under the care of 6 experienced surgeons. We did not know the exact size and chronicity of the rotator cuff tears that the patients sustained and that were subsequently fixed, so it is unknown if tear size or chronicity played a role in the outcomes. While this is the first study to evaluate outcomes after TSA in patients with prior RCR, the numbers were small, thus a 1:3 matching was used to increase the sample size. Larger studies are needed to corroborate the results of the current study to confirm there is no difference in outcomes between patients who undergo RCR before TSA compared with those who do not. The number of patients with 5-year data was limited, and so we could not definitively conclude there were no differences in outcomes at 5 years. Furthermore, this was a retrospective review of prospectively collected data. The quality of the RCR at the index total shoulder was not recorded. Finally, the sample size was not large enough to compare outcomes after TSA in patients with a history of a prior open versus arthroscopic RCR.
Conclusion
TSA in patients with a history of prior ipsilateral RCR led to significant improvements in clinical outcomes. No difference in clinical outcomes at 2 years after TSA was found between patients with and without a history of prior ipsilateral RCR.
Footnotes
Final revision submitted March 7, 2020; accepted March 20, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.J.E. has received research support from DePuy Synthes and educational support from Arthrex, DePuy Synthes, and Smith & Nephew. J.S.D. has received research support from Arthrex; speaking fees from Arthrex; consulting fees from Arthrex, Linvatec, Merck Sharp & Dohme, Trice Medical, and Wright Medical; and royalties from Linvatec and Wolters Kluwer Health–Lippincott Williams & Wilkins. D.M.D. has received other financial support from Biomet, consulting fees from Wright Medical and Zimmer Biomet, and royalties from Saunders/Mosby-Elsevier and Zimmer Biomet. L.V.G. has received consulting fees from Exactech and Zimmer Biomet and speaking fees from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital for Special Surgery (study No. 2013-014-CR5).