
Abstract
Background:
Unicompartmental knee arthroplasty (UKA) and high tibial osteotomy (HTO) are treatment options for patients with medial spontaneous osteonecrosis of the knee (SONK).
Purpose:
To compare the clinical outcomes after UKA and HTO in patients with SONK.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective study included 42 patients who had undergone Oxford UKA and 40 patients who had undergone opening-wedge HTO between 2014 and 2020. All patients were diagnosed with isolated medial SONK without subchondral collapse of the femoral condyle and tibial plateau. The patients were preoperatively and postoperatively evaluated using the Lysholm knee scoring system, the Western Ontario and McMaster Universities Osteoarthritis Index, and a numeric rating scale assessing patient satisfaction.
Results:
Patients in the UKA group were significantly older than those in the HTO group (median age, 71.5 years [IQR, 68.0-76.5 years] vs 65.0 years [IQR, 60.0-70.0 years], respectively; P < .001). The median follow-up time was 3.78 years (IQR, 2.45-4.53 years) for the UKA group and 3.87 years (IQR, 2.90-5.60 years) for the HTO group. Significant improvements in functional scores were observed in both the UKA and HTO groups (P < .001 for all), with no significant between-group differences in scores at the final follow-up (≥2 years after surgery). The satisfaction rate was similar (80.95% for UKA and 75.0% for HTO).
Conclusion:
According to the study results, significant improvements in clinical outcomes were seen after opening-wedge HTO with microfracture for a younger group of patients with SONK without subchondral collapse, while Oxford UKA had a comparable effect on an older group of patients. Both UKA and HTO were found to be viable surgical approaches for SONK at short- to midterm follow-up.
Keywords
Spontaneous osteonecrosis of the knee (SONK) was first described by Ahlbäck et al 1 in 1968. It mainly occurs in older patients (age, >60 years), and women are 3 times more likely to be affected than are men. 26 However, its cause remains unknown. Yamamoto and Bullough 43 postulated that a subchondral insufficiency fracture is the primary cause of SONK. The most common presentation of SONK is acute-onset localized knee pain mainly involving the medial femoral condyle and rarely involving the medial tibial plateau, without a known history of trauma. 27
Advancements have been made in the treatment approaches for patients with SONK. Nonoperative approaches, such as restricted weightbearing and analgesic drug use, can be adopted for patients without condyle collapse. 31 Surgical options include arthroscopic microfracture, 2 osteochondral grafts, 39 high tibial osteotomy (HTO), unicompartmental knee arthroplasty (UKA), and total knee arthroplasty (TKA); however, the optimal treatment modality remains debatable. UKA and HTO are effective surgical treatment options for SONK and have been demonstrated to markedly improve patients’ functional outcomes and survival rates.5,10,17,18,38
The purpose of the current study was to compare UKA and HTO in patients with SONK in terms of their postoperative clinical outcomes.
Methods
Study Design
After receiving approval from our institutional review board, we collected relevant data from our hospital database of consecutive patients with SONK who had undergone Oxford UKA or opening-wedge HTO (OWHTO) between January 1, 2014, and December 31, 2020. Included were patients with the following criteria: (1) SONK confirmed based on the preoperative magnetic resonance imaging (MRI) features described by Lecouvet et al, 23 (2) isolated medial compartment SONK without subchondral collapse of the femoral condyle and tibial plateau, (3) failure of nonoperative treatment for a minimum of 3 months after the MRI diagnosis of SONK, (4) varus alignment <15°, (5) flexion contracture <15°, 32 and (6) not taking TKA into consideration after shared decision-making. Patients with the following characteristics were excluded: (1) history of ligament reconstruction, (2) inflammatory arthritis, (3) secondary osteonecrosis (history of alcohol abuse or corticosteroid treatment), and (4) having undergone both HTO and UKA in separate knees. Cases that further required secondary operation were recorded.
Diagnosis Criteria of SONK
Typical radiographic findings, such as the flattening and subchondral radiolucency of the weightbearing area, are often negative in the early stages of SONK. 15 Because of its high sensitivity to bone marrow changes, MRI may be useful in the diagnosis of patients with suspected SONK. Lecouvet et al 23 described the typical features observed on the MRI scans of patients with early irreversible osteonecrosis: subchondral hypointensity visible on T2-weighted images, deep lines of reduced signal within the affected condyle, and localized depressions in the epiphyseal contour. In all patients included, we confirmed the diagnosis of SONK by reviewing their MRI scans for the features mentioned by Lecouvet et al. 23
Surgical Techniques and Rehabilitation
After receiving a full explanation of the 2 types of surgery for SONK, including their advantages and disadvantages, along with possible complications and risks, the patients selected the type of surgery themselves. OWHTO was performed using the AO TomoFix plate (Synthes GmbH), and mobile-bearing Oxford UKA (Zimmer Biomet) was performed using a minimally invasive technique. All procedures were performed by a experienced surgeon (P.-W.W.) in our orthopaedic department.
Opening-Wedge HTO
For OWHTO, a full-length standing anteroposterior radiograph was obtained for preoperative planning. The Miniaci method 30 was used to calculate the correction angle. The postoperative weightbearing line was set to be within 55% to 62.5% from the medial edge of the tibial plateau. Knee arthroscopy and microfracture were routinely performed by the surgeon before the actual procedure, with the cartilage in all knee compartments and cruciate ligament stability assessed during the process. Microfracture was performed strictly according to the technique described by Steadman et al, 35 with multiple holes of 3 to 4 mm deep and 1 to 2 mm in diameter spaced approximately 1 to 2 mm apart. Then, we started the OWHTO with an oblique incision to expose the medial proximal tibia, followed by release of the medial collateral ligament. The upper edge of the pes anserinus insertion was set as the starting point of the osteotomy. Two K-wires were positioned to be the cutting guide of the saw, and >10 mm of the lateral cortex was left intact to prevent hinge fracture. After the first cut of the posterior two-thirds of the tibia, the second cut was made proximal to the tibial tuberosity at an angle of 110° to 120° from the previous cut. After completion of the osteotomy, a spreader (TomoFix bone spreader) was placed into the osteotomy gap; then by opening the spreader with a screwdriver, the gap was opened to the desired width. Next, the TomoFix plate was fixed at the optimal position with 7 to 8 locking screws, followed by placement of the bone substitutes (Bicera; Wiltrom Ltd) into the osteotomy gap. 34
For rehabilitation, muscle-strengthening exercises and active and passive range of motion exercises were started on the first postoperative day. Within 2 weeks after surgery, the patients were instructed to begin partial weightbearing with the help of crutches. Full weightbearing was permitted after 6 weeks, if feasible.
Unicompartmental Knee Arthroplasty
We performed a mobile-bearing UKA using the cemented Oxford knee with a minimally invasive approach. The patient was placed supine with the operated knee flexed to 90°. A medial parapatellar incision was made from the patella to 3 cm under the joint line, and the osteophyte of the affected medial compartment was removed. The optimal femoral sizing spoon was inserted by using a tibial saw guide and a G-clamp together. Next, vertical and horizontal cuts were made to excise the eroded part of the medial tibial plateau. A femoral drilling guide was placed to confirm the position of the posterior resection guide, and the posterior aspect of the femoral condyle was removed. The first milling was performed using a 0 spigot, and the flexion and extension gaps were further equalized through subsequent drilling. An anti-impingement guide was applied to prevent impingement while bearing in full extension and full flexion. Finally, the final trial reduction was tested before cementing the tibial and femoral components. The bearing was inserted last, and a radiograph was obtained postoperatively to ensure correct placement of the components. 32
For rehabilitation, quadriceps muscle and passive range of motion exercises were started from the first postoperative day, aiming to achieve 90° of flexion in 7 days. The patients were instructed to begin partial weightbearing with crutches on the second postoperative day.
Preoperative and Postoperative Evaluation
The patients’ functional scores, including the Lysholm knee score 28 and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score, 3 were assessed before surgery and during the patients’ visits to the clinic or via telephone inquiry for at least 2 years postoperatively. If the patient underwent a bilateral procedure, the functional scores reflected the combined results of both knees. The functional score questionnaire had been translated into Mandarin in a previous study, and no comprehensive problems were reported.37,42 The functional scores of the cases with revision to TKA were not included in the statistical analysis, as they may not accurately represent the effectiveness of the previous surgery.
Additionally, patient satisfaction was evaluated using a 4-item numeric rating scale: 0 (unsatisfied), 1 (neutral), 2 (satisfied), and 3 (very satisfied). Based on their responses, patients were categorized as either unsatisfied (score of 0 or 1) or satisfied (score of 2 or 3). The cases of complication and revision surgery were also recorded.
Statistical Analysis
The Shapiro-Wilk test was performed to assess the normality of the distribution of continuous variables. Because of the nonnormal distribution, continuous variables are presented as median (interquartile range). Categorical variables are presented as frequency (percentage). The Mann-Whitney U test (for continuous variables) and chi-square test (for categorical variables) were used to compare the UKA and HTO groups and their subgroups (ie, satisfied vs unsatisfied patients). The Wilcoxon signed-rank test was used to compare clinical outcomes before and after surgery. Univariable and multivariable linear regression analyses were performed to determine the differences between the UKA and HTO groups. Potential confounders, including age and sex, were adjusted for in the multivariable models. All statistical analyses were performed using R (Version 4.1.0; R Core Team), and a P value of <.05 was considered to be statistically significant.
Results
After excluding 2 patients (1 with HTO and UKA in separate knees and 1 with previous anterior cruciate ligament reconstruction), 95 patients who underwent Oxford UKA or OWHTO were included in this retrospective cohort study: 51 patients underwent Oxford UKA and 44 patients underwent OWHTO, and 1 patient in each group underwent a bilateral procedure. In the UKA group, 8 patients were lost to follow-up and 1 underwent revision TKA. In the HTO group, 3 patients were lost to follow-up and 1 underwent revision TKA. One knee in the HTO group underwent wound debridement for a superficial tissue infection 2 weeks after the initial operation (Figure 1).
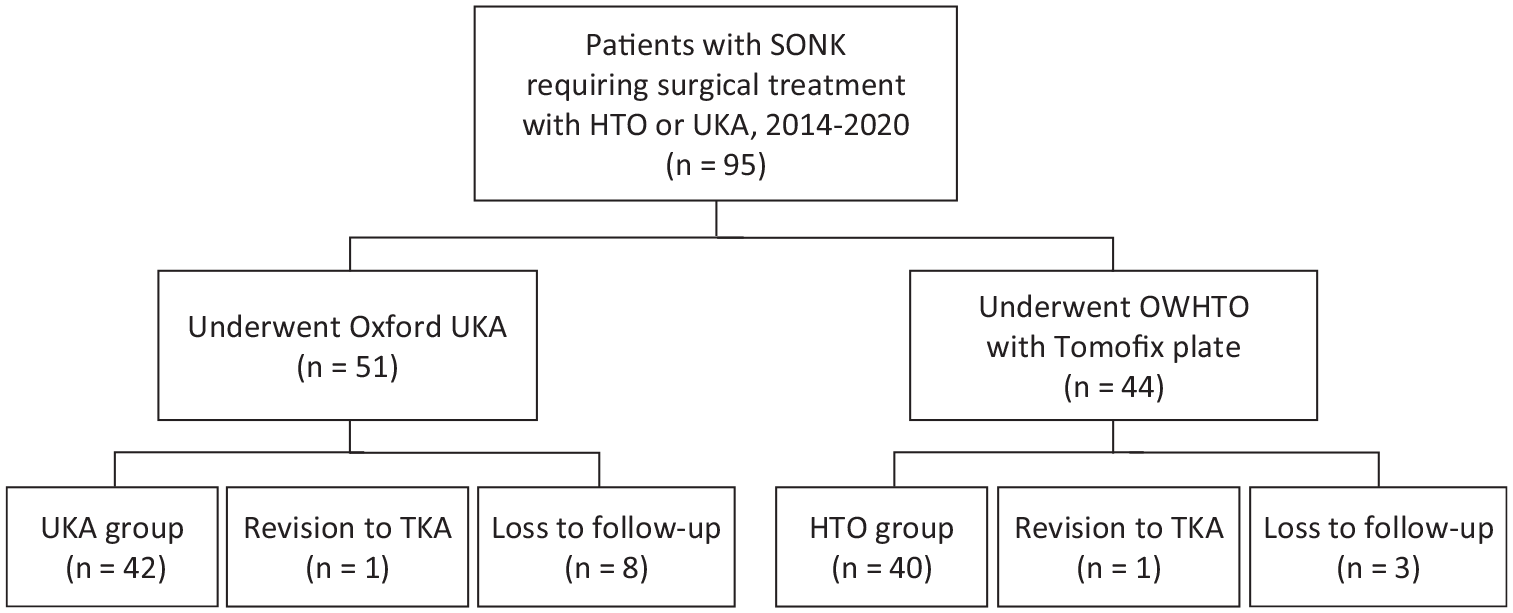
STROBE (Strengthening the Reporting of Observational Studies) patient flow diagram. HTO, high tibial osteotomy; OWHTO, opening-wedge high tibial osteotomy; SONK, spontaneous osteonecrosis of the knee; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
The final analysis included 82 patients: 42 patients (43 knees) in the UKA group and 40 patients (41 knees) in the HTO group. The characteristics of the included patients are summarized in Table 1. All patients were evaluated for ≥2 years (median follow-up duration: UKA, 3.78 years [IQR, 2.45-4.53 years; range, 2-6.5 years]; HTO, 3.87 years [IQR, 2.90-5.60 years; range, 2-7.8 years]).
Patient Characteristics a
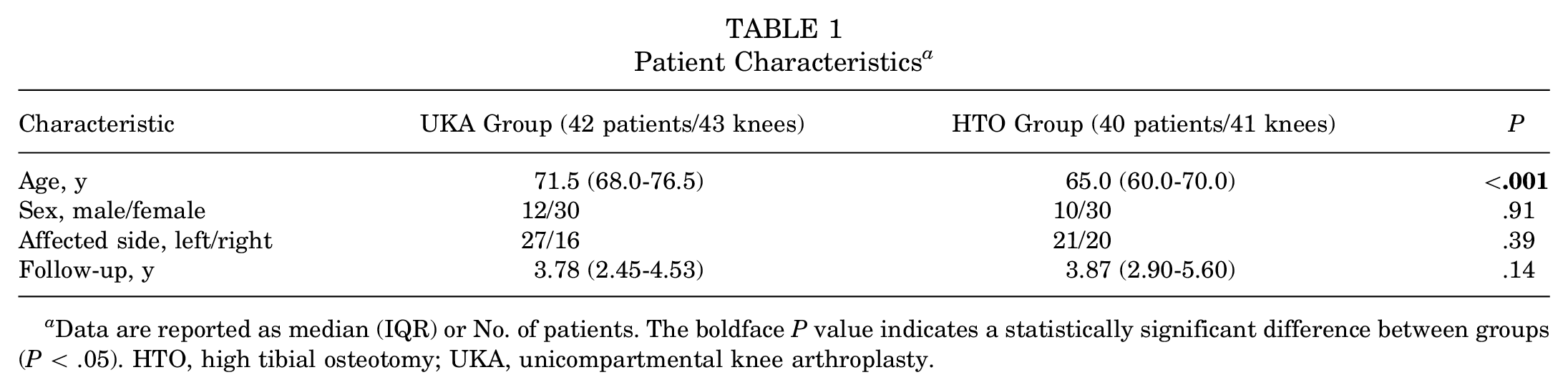
Data are reported as median (IQR) or No. of patients. The boldface P value indicates a statistically significant difference between groups (P < .05). HTO, high tibial osteotomy; UKA, unicompartmental knee arthroplasty.
Clinical Outcomes
In both the UKA and HTO groups, the WOMAC and Lysholm scores at ≥2 years postoperatively were significantly better than the preoperative scores (P < .001 for all). No significant differences between the groups were noted in functional scores or patient satisfaction (Table 2).
Comparison of Clinical Outcomes Between the UKA and HTO Groups a

Data are reported as median (IQR) or n (%). Patient-reported outcome scores were reported once in patients who received bilateral procedures (n = 1 for each group). Boldface P values indicate statistically significant differences between preoperative and postoperative values (P < .05). HTO, high tibial osteotomy; UKA, unicompartmental knee arthroplasty; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Because of the difference in mean age between the UKA and HTO groups, we conducted multivariable linear regression to adjust for potential confounders. After adjustments for age and sex, no significant between-group differences were observed in postoperative functional scores (Table 3).
Multivariable Linear Regression of UKA and HTO Outcomes a

HTO, high tibial osteotomy; UKA, unicompartmental knee arthroplasty; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Adjusted for age and sex.
The comparison of outcomes between unsatisfied and satisfied patients is shown in Table 4. In the UKA group, a significantly worse postoperative WOMAC score was found in the unsatisfied patients compared with the satisfied patients (P < .005). In the HTO group, both the WOMAC and Lysholm scores were significantly worse in the unsatisfied patients (P = .04 for both).
Comparison of Outcomes Between Unsatisfied and Satisfied Patients in the UKA and HTO Groups a

Data are reported as median (IQR). Boldface P values indicate statistically significant differences between unsatisfied and satisfied patients (P < .05). HTO, high tibial osteotomy; UKA, unicompartmental knee arthroplasty; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Discussion
The results at short- to midterm follow-up in the current study implied that both UKA and HTO are viable treatment options for patients with SONK. The 2 procedures led to comparable and significant improvements in the patients’ functional scores. Furthermore, the satisfaction rate was 80.95% for UKA and 75.0% for HTO, respectively.
Previous studies have demonstrated that both UKA and HTO are effective treatment options for SONK. Heyse et al 14 retrospectively analyzed 52 cases of UKA for SONK (mean follow-up duration, >10 years). They found that the mean postoperative WOMAC score at the latest follow-up was 7.7 ± 11.4, similar to the value observed in our UKA group. Several other studies have also reported significant improvements in the flexion angle and functional scores after Oxford UKA for SONK.6,10,22,45 On the other hand, Choi et al 5 performed biplanar OWHTO in 33 patients with SONK and reported a significant improvement in the WOMAC score (from 38.83 ± 8.7 preoperatively to 15.66 ± 5.47 at 41 months postoperatively). Takeuchi et al 38 performed OWHTO combining artificial bone substitutes in 30 patients with SONK, reporting significant improvements in the patients’ Knee Society Scores at a mean follow-up of 40 months; 70% of their patients could sit in the Japanese style, which requires deep knee flexion. Follow-up arthroscopy in 24 patients performed after 2 years revealed that the necrotic area was completely covered with fibrous cartilage-like tissue. These findings are consistent with our results, indicating that both UKA and HTO can significantly improve clinical outcomes with comparable efficacy in patients with SONK.
Previous studies have indicated that joint-conserving surgery such as HTO could be considered in the precollapse stage of SONK.5,33 In our study, we performed OWHTO with microfracture for patients with SONK. Akgun et al 2 reported that arthroscopic microfracture could provide improvement in the Lysholm score for patients with SONK. However, a systematic review pointed out that microfracture alone resulted in poorer clinical outcomes when compared with microfracture with concomitant OWHTO, with a higher reoperation rate in the microfracture only group. 7 Furthermore, a finite element study showed that the stress in the medial compartment can be alleviated by correcting the weightbearing axis, 40 which cannot be achieved by microfracture alone. In our opinion, OWHTO with microfracture was capable of achieving improvement in clinical outcomes for patients with SONK. In addition, OWHTO may be able to provide cartilage regeneration in the SONK-affected area. Kumagai et al 20 noticed improved cartilage status in terms of International Cartilage Regeneration & Joint Preservation Society grade during second-look arthroscopy at a mean of 15.2 ± 5.1 months postoperatively. Takeuchi et al 38 and Goshima et al 11 both revealed that the necrotic area was covered with fibrous cartilage-like tissue at second-look arthroscopy after OWHTO.
In our study, the reported satisfaction rate was 80.95% for UKA and 75.0% for HTO, similar to the 20% dissatisfaction rate reported in a previous systematic review regarding primary TKA for patients with osteoarthritis. 13 Koh et al 19 reported that dissatisfaction in OWHTO was related to the severity of osteoarthritis, while age, activity scale, and other surgical factors did not seem to be predictive factors; as for UKA, they reported that younger age (<60 years) and severe varus deformity were related to dissatisfaction. Because the current study put emphasis on medial SONK, some of these factors, such as the degree of osteoarthritis in the affected knee, were not thoroughly analyzed. Moreover, further subgroup analysis in our study found no age difference between satisfied and unsatisfied patients; however, previous studies have indicated that older age was associated with a higher risk of revision HTO.12,25,44 Fitoussi et al 8 analyzed 108,007 patients after UKA and HTO and reported that age >60 years increased the risk of revision up to 8 times in HTO; on the contrary, age <60 years increased the risk of revision UKA. Boyer et al 4 analyzed 3754 UKA patients and also revealed that a younger age lowered implant survival, especially leading to revision for aseptic loosening. Given this evidence and their surgical experience, the surgeons in our institution might have had a tendency to encourage UKA when facing older patients, which may explain the significant age difference between the UKA and HTO groups in our study. Therefore, the 2 procedures should be carefully selected in patients with SONK considering patient characteristics and surgical indications to achieve better satisfaction and clinical outcomes.
Recent studies have indicated that UKA seemed to be equivalent to or even more suitable than TKA for patients with SONK. Flury et al 9 demonstrated that UKA had a superior WOMAC score compared with TKA in patients with SONK, and similar complication rates. Suh et al 36 also reported a better functional score at 6 months in UKA and comparable outcomes at longer follow-up, and UKA may provide a better range of motion postoperatively. Moreover, in previous studies concerning osteoarthritis, UKA was reported to be associated with lower joint awareness and a significantly lower rate of surgically managed periprosthetic joint infection in comparison with TKA.16,24 Likewise, Matsumoto et al 29 reported a comparable satisfaction between OWHTO and TKA, with OWHTO showing significantly better satisfaction in pain relief and restored function in stair climbing.
However, the subsequent progression in the lateral compartment might be a concern for long-term survival and clinical outcomes after UKA and HTO. Walker et al 41 revealed good long-term functional outcomes and survivorship at least 10 years after minimally invasive Oxford UKA in medial osteoarthritis, but degeneration in the lateral compartment was noted during follow-up. Kumagai et al 21 reported a lateral compartment cartilage degeneration at second-look arthroscopy after OWHTO, which was associated with deterioration in 10-year clinical outcomes. To date, studies regarding Oxford UKA and OWHTO for SONK have merely focused on midterm outcomes, with the longest mean follow-up being 8.4 years. 10 Above all, although HTO and UKA both showed satisfactory clinical outcomes and good survival at short- to midterm follow-up, whether their long-term effectiveness could be maintained still requires further investigation.
Limitations
First, because of the rarity of SONK, our sample size was relatively small, and further studies with a larger number of cases are needed to determine the optimal procedure. Second, we did not randomly separate the patients into different surgery groups. On the contrary, patients were free to choose the surgical technique after we described the procedures. However, the surgeons may have tended to encourage older patients to undergo UKA given the higher risk of revision after HTO, which might have resulted in selection bias. To mitigate the bias, we adjusted for potential confounders by using a multivariable linear regression model; no significant differences were noted in functional scores between UKA and HTO. Lastly, we assessed the clinical outcomes after a relatively short follow-up, demonstrating only the short- to midterm outcomes of UKA and HTO. Future studies with longer follow-ups are required to determine whether UKA and HTO can provide good long-term functional scores and satisfaction for patients with SONK.
Conclusion
According to our results, OWHTO with microfracture significantly improved the clinical outcomes for a younger group (median age, 65 years) of patients with SONK without subchondral collapse, while Oxford UKA had a comparable effect on an older group of patients (median age, 71.5 years). The current study demonstrated that both Oxford UKA and OWHTO are viable surgical options for SONK treatment at short- to midterm follow-up.
Footnotes
Acknowledgements
The authors thank Yu-Yin Wei for her help in proofreading the English language of the study.
Final revision submitted April 12, 2024; accepted April 23, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research assistance was provided by Shuang Ho Hospital (No. 113SHHR-05). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Taipei Medical University–Joint Institutional Review Board (reference No. N202307005).