
Abstract
Background:
Spontaneous osteonecrosis of the knee (SONK) is a poorly understood but debilitating disease entity. Total knee arthroplasty (TKA) is the standard of care for those patients who fail conservative management, but considering SONK’s predilection for affecting a single knee compartment, unicompartmental knee arthroplasty (UKA) appears to be a more tailored option. Unfortunately, conflicting data exist on the utility of UKA in SONK. Thus, the purpose of this study was to evaluate functional outcomes and revision rates of UKA in the setting of SONK.
Methods:
A systematic literature search was performed to evaluate all studies examining patients who underwent UKA for SONK. Screening of the articles was performed using multiple Boolean search strings, methodological index for non-randomized studies criteria, and other selected exclusion criteria.
Results:
Seven studies were included, with a total of 276 knees (273 patients). The mean age was 68 years (64–74 years), with a mean body mass index of 26 kg/m2 (25–29 kg/m2). The final range of motion was 125° (124–126°). Standardized mean difference (SMD) of clinical improvement pre- and post-outcome was 3.39 (p < 0.001). The improvement in the visual analog score was 57.03 points, with an SMD of 4.57 (p < 0.001). Revision rates were determined to be 5.51% (95% confidence interval of 1.96–10.69%).
Conclusion:
Our meta-analysis demonstrated that in properly selected patients, UKA could be an excellent alternative to TKA for patients with SONK. These data show that UKA has few complications, significant improvements on functional outcomes, and good survivorship at a mean follow-up of 6 years.
Introduction
Also known as idiopathic or primary osteonecrosis, spontaneous osteonecrosis of the knee (SONK) is a disease entity whose primary etiology remains unknown. 1 –3 Although some cite microtrauma or bone edema as potential causes, the diagnosis is generally arrived through a combination of patient presentation and subsequent imaging studies. 4,5 It commonly presents with a sudden onset of monoarticluar pain, with no inciting trauma. This discomfort is usually described as worse at night, with a normal physical examination except for localized pain over the affected osseous area. 1,2,4,6 Patients tend to be older than 50 years of age, affecting women more than men, and have no other risk factors for osteonecrosis. Within the possible treatment alternatives, total knee arthroplasty (TKA) has been described as the standard treatment for patients with end-stage disease who have failed conservative management. 1,2,6 –9
SONK, however, is usually localized to the medial compartment of the knee; therefore, unicompartmental knee arthroplasty (UKA) appears to be a more tailored treatment option. 6 By preserving the unaffected compartments of the knee, more native joint kinematics and proprioception can be preserved when compared to TKA. 10 In addition, there may also be a decrease rate of deep vein thrombosis and total blood loss in UKA when compared to TKA. 10 These advantages make UKA an appealing alternative.
However, the superiority of UKA implants in terms of preservation of joint kinematics in the setting of SONK has come under scrutiny. Some manuscripts state that UKA is comparable to TKA, while others conclude that UKA is an inferior construct. 1,7,9,11 Unfortunately, due to the relative rarity of SONK, these studies often lack in patient numbers and control groups, thus making it difficult to draw meaningful conclusions. To address these limitations, we plan to systematically evaluate all available current literature on UKA in the setting of SONK. More specifically, the purposes of this study are to (1) understand the survivorship of UKAs, (2) determine the clinical and functional outcomes, and (3) determine the complication rates seen in patients who undergo UKA in the setting of SONK.
Methods
We performed a systematic literature search of the MEDLINE library to evaluate all studies examining patients who underwent UKA for SONK. This was performed with multiple strings, which included “Spontaneous Osteonecrosis Knee” (179 studies) and “Spontaneous Osteonecrosis Knee and Unicompartmental Knee Arthroplasty” (10 studies). Two authors, independently blinded from each other’s results, further examined the title and abstract of these studies, finding that 50 were relevant to our criteria (Figure 1.).

Research flow chart.
Furthermore, each study was evaluated using the methodological index for non-randomized studies (MINORS) criteria. 12 This criterion was further modified into an all-or-nothing scale in which studies that adequately reported a subset of the MINORS criteria received one point. This approach has been used in previous studies and has been validated. 13 All studies that had less than six points were excluded from this study. All studies were then screened based on their inclusion criterion: studies that specifically assessed SONK treated with UKA with outcome measures (outcome measures included the Kaplan–Meier survival analysis, reason for implant failure or revision, range of motion (ROM) postsurgery, and global knee outcome scores). Exclusion criteria were (1) those articles not written in English, (2) articles that did not differentiate between primary and secondary osteonecrosis of the knee in their results, and (3) modified MINORS criteria of greater than or equal to 64 review article. We also reviewed the references for each of the included papers in an attempt to identify potential studies that were omitted. The overall search process produced seven studies for final inclusion in our analysis, two of which were prospective in design, with the remaining five being retrospective.
Of the seven studies examined, multiple manuscripts only reported the Knee Society Score (KSS) or Hospital for Special Surgery Score (HSS) individually, rather than both scores (n = 4 KSS, n = 3 HSS). These two scoring systems were treated as equivalent and averaged together in our final analysis. For full comparison between the KSS and HSS scores, the functional and clinical components of the KSS were combined. Similar comparisons between different knee outcome scores have been performed in previous studies. 1,14
Extracted data included years of follow-up, patient demographics (age, gender, and body mass index (BMI)), laterality of lesion, reason for revision (aseptic loosening, superficial and deep infection, and poly wear), revision rate, knee ROM, maximum knee flexion, clinical outcomes (KSS, visual analog score (VAS), and HSS), and Kaplan–Meier survival curves at 5-, 10-, and 15-year follow-up.
All data were compiled in a Microsoft Excel spreadsheet (2012 version; Microsoft Corporation, Redmond, Washington, USA). The patient outcome variables and demographics were recorded from each study. Then, with the aid of a statistical software (MedCalc Software, version 16.4.3, bvba; Ostend, Belgium), random effect models were utilized to determine statistical mean differences (outcome metric data) and rates (revisions) for patients undergoing UKA.
Results
The 7 studies that were included in our final cohort evaluated a total of 276 knees (273 patients), of which 273 knees had medial and 3 had lateral compartment osteonecrosis. These patients had a mean age of 68 years (range 74–64 years). There was a 2:1 ratio of female to male (182:91), with a mean BMI of 26 kg/m2 (range of means 25–29 kg/m2). These patients were followed up for a mean of 6 years (range 2–11 years) (Table 1).
Patient demographics.
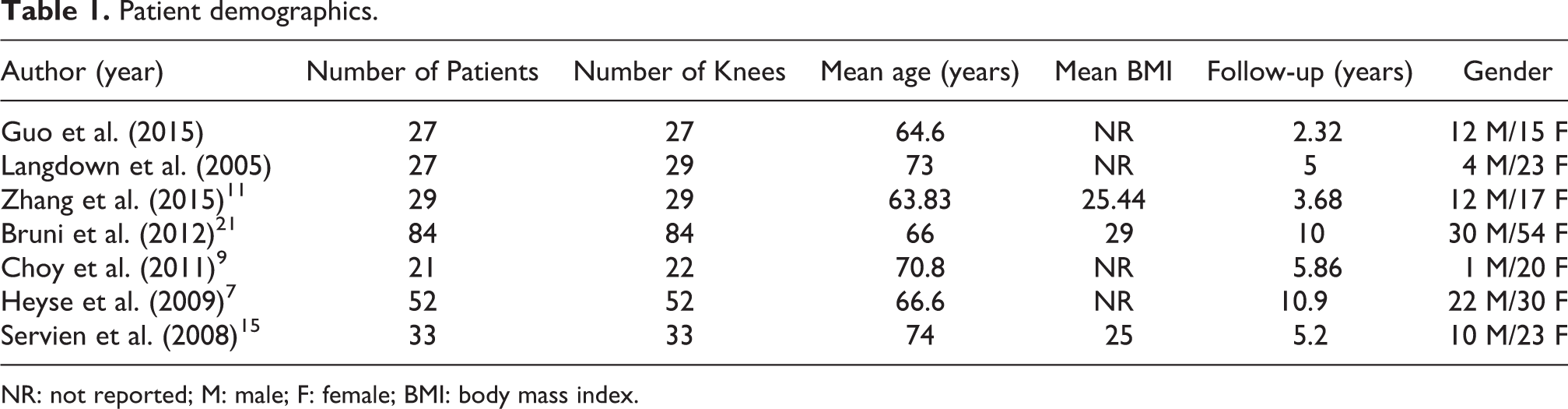
NR: not reported; M: male; F: female; BMI: body mass index.
The final ROM for patients who underwent UKA for SONK was 125° (range 126–14°), and the final maximum flexion was 127° (range 102–146°). In terms of clinical improvement from pre- and postsurgery, because different scales were used in multiple studies (KSS and HSS), we adjusted all values to a 100-point scale with 0 being the worst outcome and 100 being the best possible outcome. The preoperative value of our combined scores was 53 points (range 35–64 points, standard deviation (SD): 15) and postoperative value was 86 points (range 63–93 points, SD 10). Our model found a standardized mean difference (SMD) of 3.39 (95% confidence interval (CI) of 2.4–4.4; p < 0.001) with respect to clinical improvement (Figure 2). The same model was used to evaluate changes in the VAS score from pre- to postoperatively, with a mean preoperative VAS of 76 points (range 69–86 points, SD 11), a postoperative mean of 19 points (range 17–20 points, SD 15), and a total improvement of 57 points. The SMD of the VAS improvement was shown to be 4.57 (95% CI of 2.96–6.20, p < 0.001) (Figure 3, Table 2).

Forest plot improvement in clinical outcome.

Forest plot improvement in pain (VAS). VAS: visual analog score.
Clinical scores pre- and postoperatively (VAS, adjusted KSS, and HSSKS).

SMD: standard mean difference; SD: standard deviation; CI: confidence interval; VAS: visual analog score; KSS: Knee Society Score; HSSKS: Hospital for Special Surgery Knee Score.
In terms of the revision rates, our model revealed a revision rate of 5.51% (95% CI of 1.96–10.69%) (Figure 4). Specifically, of the revisions that occurred, 2 were due to septic failure and 17 were due to aseptic failure (Table 3). No revisions for polyethylene wear or superficial infections was reported. Two studies described a Kaplan–Meier survivorship at 10 and 15 years of 93% and 90%, respectively. 7,15
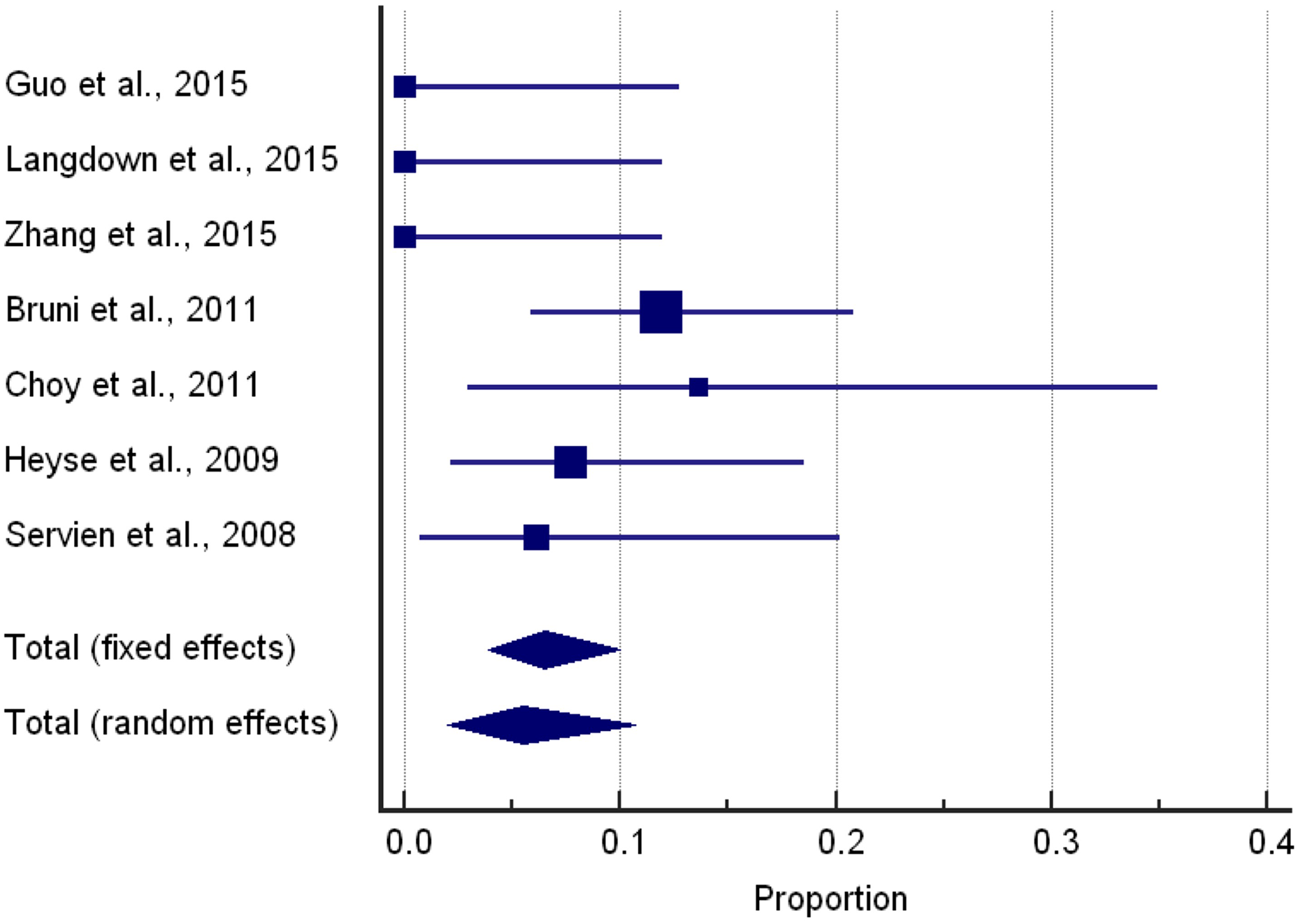
Forest plot of revision rates.
Complications leading to revisions.

CI: confidence interval; SD: standard deviation.
aUsing a total (random effects) model.
Discussion
Primary SONK is a poorly understood disease entity that can leave patients with severe disability that is refractory to conservative treatment modalities. 8,16 For end-stage SONK, knee arthroplasty appears to be the current treatment of choice; however, there is controversy over the unicompartmental implant in the setting of primary SONK. 1,6 Using a systematic review of the literature, we demonstrated that UKA can be an acceptable procedure for the treatment of primary SONK when it is correctly indicated in a carefully selected subset of patients. UKA had acceptable survival analysis as well as revision rates at extended follow-up and had good clinical outcomes both in the short- and long-term with an overall revision rate of 5.51%.
This study had several limitations typical of a systematic review and/or meta-analysis. These limitations included the fact that we may have missed some of the articles pertaining to this subject. This chance was minimized, as two separate investigators conducted individual literature searches and cross-referenced each paper to ensure completeness. The risk of inclusion of poorly designed studies was mitigated using specific criteria (modified MINORS). There is also the risk of inappropriate combination of heterogeneous data; however, we were careful to list each data point from each paper separately in the project’s electronic spreadsheet to ensure accurate measurements and proper units for continuity and correctness. We are also limited by the cohort size of the included manuscripts; however, this study evaluates the largest subset of SONK patients who underwent UKA. There is also a risk that our data could be partially skewed due to the scaled adjustment for clinical scores. However, this was the only alternative; hence, this was necessary in order to gain more meaningful results from our data pool.
Our findings were similar to those described by Richardson and Morris who showed high rates of survival for UKA implants at extended follow-up as well as excellent clinical outcomes determined by both patient questionnaires and clinical examinations. 17 We were also able to show that most revisions were caused by aseptic loosening, which similar to other literature findings. 6,7,9 In contrast, our study has contradictory results to those reported by Myers et al. 1 who concluded that UKA was inferior to TKA with only “fair” results. However, in their discussion, they stated that the UKAs may have been conducted on patients in whom a this procedure was not correctly indicated, thus skewing their results. There was also a difference between our results and those of Radke et al. 6 , in which they found higher revision rates in UKA when compared to TKA. However, in the study by Radke et al., the UKA group contained one patient with previous radiation therapy and three patients actively undergoing corticosteroid therapy, which may have also skewed their results.
Although our study does not focus on alternative procedures to UKA and TKA for the treatment of SONK, several other procedures been reported in the literature with varying success. These include arthroscopic debridement, microfracture, core decompression, and osteochondral allograft transfer system procedures; however, small patient numbers, short follow-up, and lack of widespread use of treatment modalities may give a false sense of potential success. The prolonged morbidity associated with some of these procedures makes them less favorable to patients when compared to arthroplasty. 3,18
Conclusion
UKA is an important tool in the arsenal of orthopedic surgeons treating patients who develop primary SONK. We have shown through this review that UKA can be an excellent alternative to TKA in the setting of properly selected patients. This statement is supported by good survivorship and functional outcomes at a mean follow-up of 6 years. Further research is needed to understand the etiology and progression of the disease process, but currently UKA remains a viable and more kinematically friendly option with a potentially higher success rate than other surgical alternatives. Further analysis is warranted with regard to secondary osteonecrosis of the knee and whether this similar disease entity affects the survival and outcome of UKA. There is also the need to continue to monitor primary SONK patients who underwent UKA as the data pool is still small with regard to this patient population and increased length of follow-up with more patients would allow for more meaningful results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.