
Abstract
Background:
Unicompartmental knee arthroplasty (UKA) is an effective treatment option for medial compartment osteoarthritis (OA) of the knee. Whether spontaneous osteonecrosis of the knee (SPONK) can be successfully treated with UKA remains controversial. This study evaluated the clinical and radiological results of patients with SPONK who were treated by UKA using Oxford phase III prostheses.
Methods:
We compared a prospective series of 23 UKA cases operated for SPONK with 235 UKA cases operated for OA. All patients underwent Magnetic Resonance Imaging (MRI) to confirm the diagnosis and exclude any major lesion in the lateral compartment. The stage, condylar ratio, and volume of the necrotic lesion were evaluated. The pre and postoperative Oxford knee scores (OKSs) were compared.
Results:
The mean follow-up was 60 months. No statistical differences in complication rates between the groups were found. The mean OKS improved from 39.48 ± 5.69 to 18.83 ± 3.82 (p < 0.05). There were no significant differences in the pre and postoperative OKS between the different groups.
Conclusion:
SPONK can be successfully treated with UKA, with a favorable short- to mid-term follow-up.
Introduction
Spontaneous osteonecrosis of the knee (SPONK) is mainly found in the elderly and has limited involvement of the periarticular bone especially in medial femoral condyle (MFC). 1 It was first described by Ahlback et al. 2 in 1968, but the precise etiology remains unknown. The typical clinical presentation is disabling pain, especially with load, which decreases during rest, and some patients describe sudden acute onset of pain, which is frequently worse at night.
Many surgeons believe joint arthroplasty is the only reasonable treatment for late-stage SPONK. 3,4 In the past decade, unicompartmental knee arthroplasty (UKA) has been extremely successful in the treatment of medial compartment osteoarthritis (OA), with a survival rate of 97% at 10 years. 5,6 The better survival in the current study as compared to previous reports may be due to improvements in modern prosthetic designs, less invasive surgical techniques, or more appropriate patient selection. The role of UKA for SPONK remains unclear. We retrospectively analyzed the clinical and radiological results of UKA in SPONK limited to MFC.
Patients and methods
From January 2007 to July 2013, 258 patients (81 males and 177 females) received medial UKAs in our department. Of these, 23 patients had SPONK, while 235 had medial compartment OA. The mean age was 71.6 years (range: 60–85 years). The mean weight was 67.5 kg (range: 50–79 kg). The mean body mass index (BMI) was 25.2 (range: 22–29; Table 1). All operations were performed by the same senior doctor in a district central hospital with Oxford phase III (Biomet Ltd, UK). All patients underwent Magnetic Resonance Imaging (MRI) to confirm the diagnosis and exclude any major lesion in the lateral compartment and anteroposterior (AP), lateral, and valgus/varus stress radiographs.
Comparison of demographical data between the two groups.

SPONK: spontaneous osteonecrosis of the knee; OA: osteoarthritis; BMI: body mass index; MFC: medial femoral condyle; MTP: medial tibial plateau.
a χ 2 test.
bGrouped t-test.
The selection criteria were as follows: (1) secondary osteonecrosis, inflectional, and immune arthritis were excluded; (2) all patients received conservative treatment at least 3 months before the operation; (3) full-thickness cartilage was preserved in the lateral compartment; (4) flexion/varus deformity was <15° and intra-articular varus could be fully corrected; and (5) presence of intact Anterior Cruciate Ligament (ACL), Posterior Cruciate Ligament (PCL), Lateral Collateral Ligament (LCL), and Medial Collateral Ligament (MCL).
All patients underwent standard minimally invasive surgery described in the Oxford partial knee manual. 5,6 Large defects after curettage of dead bone were filled with cement during surgery (Figure 1). All components were cemented. After surgery, static quadricep exercises and continuous passive motion were started on the first postoperative day to achieve 90° knee flexion over 2–3 days. Walking with weight bearing using two crutches was started on the same day.

Large defects after curettage of dead bone were filled with cement.
The clinical and radiographical data of pre and postoperation were recorded. The clinical follow-up was assessed at 1 month, 3 months, 6 months, 1 year, and once per year thereafter. Follow-up consisted of physical examination, recording of pain and complications, and a standard series of radiographs. Pain, function, and health-related quality of life were evaluated pre and postoperatively by patient- and assessor-based outcome scores. Oxford knee score (OKS) consisting of pain and function, ranging from 12 to 60, with 12 being the best outcome was used. 7
The classification of SPONK was evaluated according to Aglietti et al. 8 Plain radiographs were normal in stage I lesions. Stage II was seen as mild flattening of the subchondral weight-bearing surface. Stage III showed subchondral lucency with mild sclerosis, distal to the lesion. Stage IV showed a radiolucent lesion with a sclerotic halo and collapse of the subchondral bone visible as a calcified plate. Stage V lesions showed secondary degenerative changes and erosions with femoral and tibial subchondral sclerosis.
We measured the location, size, stage, condylar ratio, and volume of the necrotic lesion by plain radiographs and MRI. Condylar ratio is the ratio of the width of lesion to the MFC in AP radiograph (Figure 2; condylar ratio = a (the width of lesion)/b (the width of the MFC) × 100%). The volume of the lesion is the product of the width and height in the coronal images and depth in the sagittal images from MRI (Figure 3; volume = a (the width in coronal) × b (the height in coronal) × c (the depth in sagittal)). The volume was then classified as small (0–10 cm3), medium (10–20 cm3), or large ( >20 cm3).

The condylar ratio = a (the width of lesion)/b (the width of the MFC) × 100%. MFC: medial femoral condyle.

The volume = a (the width in coronal) × b (the height in coronal) × c (the depth in sagittal).
The accuracy of implant positioning was determined by standing AP and lateral radiographs during routine outpatient clinic visits. Analysis of X-rays was performed by an independent investigator who was not involved in the surgical procedure. On AP views, the varus (−)/valgus (+) alignments of the femoral component were measured relative to the long axis of the tibia. On lateral views, flexion (−)/extension (+) of the femoral component was measured relative to the posterior femoral cortex. 9 Subsidence, dislocation, loosening, and osteonecrotic changes in the lateral compartment were observed (Figure 4).

X-rays showing a restored component.
Data were analyzed using SAS8.1. (SAS Institute, NC, USA)Age, gender, BMI, and complications between different groups were compared using χ 2 test. The pre and postoperative OKS was compared using paired t-test. OKS and femoral component alignment (FCA) between different groups were compared using grouped t-test. The significance level was set at p < 0.05.
Results
No significant differences were found in gender, age, and BMI between SPONK and OA groups (Table 1).
The SPONK lesion was limited to the medial condyle of the distal femur in all cases. The lesions were stage IV (16 cases) and stage V (seven cases) by Aglietti’s classification. The condylar ratio were 25–60%, 18 cases were < 50% of condylar ratio, and 5 cases were > 50% of condylar ratio. The volume of lesion was small in 17 cases and medium in 6 cases.
The mean follow-up was 60 months (range: 24–108 months). No complications of death, fat embolism, deep vein thrombosis, and prosthetic infection were seen. No subsidence and loosening were observed in X-rays. Bearing dislocations occurred in three cases, which were changed to a thicker bearing. Lateral compartment OA occurred in one case, which was revised to total knee arthroplasty (TKA). Superficial infection occurred in four cases. At the final follow-up, the mean OKS score improved from 39.48 ± 5.69 to 18.83 ± 3.82 (p < 0.05). The femoral component valgus/varus alignment was −0.89°± 3.72° and flexion/extension alignment was −1.02°± 3.25°. All FCAs were between ± 10° valgus/varus and flexion/extension. Comparison of the clinical results between the SPONK and OA groups is shown in Table 2. Comparison of the clinical and radiographical results between small volume and medium volume of SPONK is shown in Table 3.
Comparison of clinical results between the two groups.

SPONK: spontaneous osteonecrosis of the knee; OA: osteoarthritis; OKS: Oxford knee score.
aGrouped t-test.
bFisher’s exact test.
Clinical results and component alignment of SPONK patients.
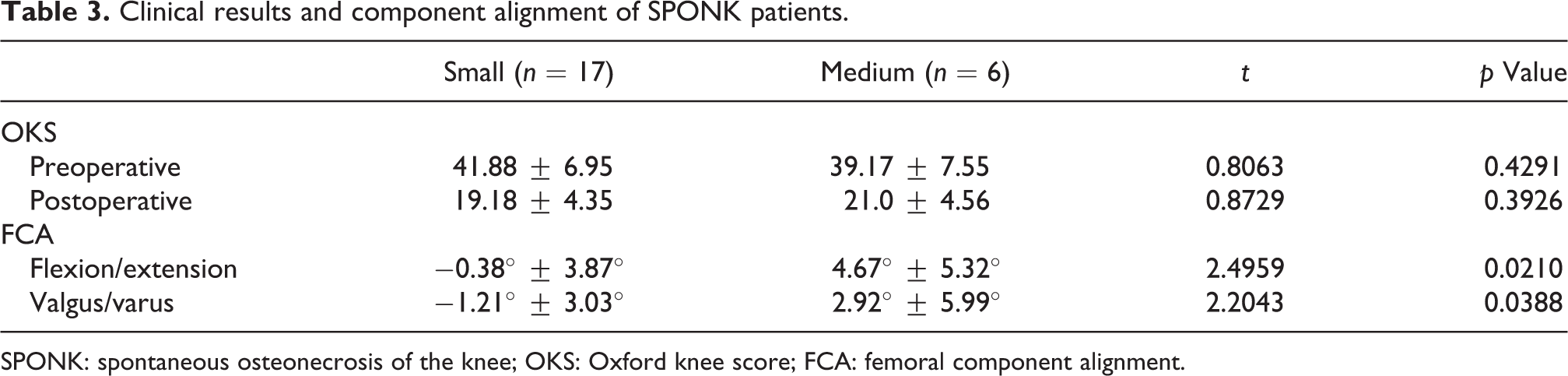
SPONK: spontaneous osteonecrosis of the knee; OKS: Oxford knee score; FCA: femoral component alignment.
Discussion
The precise etiology of SPONK remains unknown. The disease is typically found in the elderly. Females are three times more often affected than men. 10 In our study, all cases were >60 years old, and the lesion was limited to the medial condyle of the distal femur. Females were 2.3 times more affected than men.
There are many treatment options for SPONK, including conservative treatment, arthroscopic debridement, drilling of the lesion, bone grafting, and arthroplasty. The optimal treatment option for SPONK depends on the symptoms as well as the grade and stadium of disease. 4,11 Soucacos et al. 12 suggested surgery for SPONK stage III or higher. Conservative treatment is suitable for small lesions without evidence of structural ruin. For lesion width > 50% of the condyle, the prognosis of conservative treatment is unfavorable. 8,13 All cases in our study were stages IV or V. Three months of conservative treatment failed in 18 cases with condylar ratios < 50%. Therefore, we support previous recommendations that joint arthroplasty is the only reasonable treatment for late-stage SPONK with secondary joint collapse. 3,4 Conservative treatment is unfavorable even for small lesions in late-stage SPONK.
Because SPONK is a disease that mainly affects the MFC, UKA can be an alternative treatment. Arthroplasties of the knee can be either total or unicompartmental. Some studies have suggested that the outcome of UKA might be inferior as compared to that of TKA. Marmor 14 reported a failure rate of 12.5% at 5.5 years. Radke et al. 15 indicated that patients who underwent TKA showed clinically better results. The failure rate was 16.4% at 5 years in patients who underwent UKA. Myers et al. 16 discussed the outcome of TKA and UKA after SPONK in their review and found that poor outcome after UKA in earlier studies was secondary to inappropriate patient selection. However, survival seems to have changed in recent studies. Parratte et al. 17 retrospectively reviewed 31 knees with osteonecrosis and showed a 96.7% 12-year survival rate of UKA. Langdown et al. 18 described 27 patients with SPONK operated with UKA at 5-year follow-up and showed no case of implant failure. Heyse et al. 4 reported 52 cases of UKA for SPONK with average follow-up of 10.9 ± 4.8 years (range: 4–25 years). The American Knee Society Score (AKS) increased from preoperative 85 ± 30 to 173 ± 27 at the latest follow-up. Patients’ satisfaction rate was 97.3%. The Kaplan–Meier survival was 93.1% at 10 years and 90.6% at 15 years. In our study, the OKS improved from preoperative 41.17 ± 7.04 to 19.65 ± 4.38 (p < 0.01) at the latest follow-up. Only one case needed revision (bearing dislocation). In our opinion, UKA is a better option than TKA for SPONK due to lower invasiveness, bone stock, and preservation of kinematics.
Some studies reported comparable results for UKA in patients with SPONK versus OA. 3,11 Servien et al. 11 compared a prospective series of 33 UKAs operated for SPONK with 35 UKAs operated for OA. The mean follow-up was 5 years. The mean postoperative International Knee Society score improved significantly, and no significant differences were found between the groups. The survival rate was 92.8% for the SPONK group and 95.4% for the OA group. They opined that UKA shows excellent clinical results in SPONK. Similarly, in our study, there were no significant differences in postoperative OKS between the two groups (19.65 ± 4.38 vs. 18.77 ± 3.80, p > 0.05). The complication rate (8.7% vs. 5.3%) and the survival rate (95.7% vs. 98.7%) were similar.
Regular osteotomy cannot eliminate large lesions. Large defects after curettage of dead bone were filled with cement during the surgery. The size of the necrotic lesion will influence the method and outcome of surgery. Choy et al. 19 classified the volume as small (0–10 cm3), medium (10–20 cm3), and large (20–30 cm3) to evaluate the therapeutic results. In their report, 22 SPONK knees accepted UKA. The survival rate at 6 years was 78%. Bearing dislocation occurred in two cases and femoral component loosening in one case (volume 22.8 cm3). They suggested that UKA could be an alternative treatment option in SPONK, and guidelines for TKA or UKA need to be established to improve the survival rate. In our study, OKS between the small and medium groups were similar (19.18 ± 4.35 vs. 21.0 ± 4.56; p = 0.39). All FCAs were between ± 10° valgus/varus and flexion/extension, and the alignment of the medium group was worse than the small group. No subsidence and loosening were observed, which may be due to the absence of large volume defects.
Our study had several limitations. First, it was retrospective, the follow-up time was short- to mid-term, and the sample size was small. Second, our study did not include large volume lesions, so it is unknown whether UKA is suitable for these cases. Third, there was no control group undergoing TKA for patients with SPONK, so we could not establish guidelines for TKA or UKA.
Conclusions
In conclusion, UKA could be a successful treatment option for SPONK in short- to mid-term, but long-term results need to be investigated. SPONK is a unicompartmental disease. UKA is a better option than TKA due to its bone and natural kinematics preservation and micro damage.
Footnotes
Acknowledgments
The authors’ institution would like to thank Shanghai Municipal Science and Technology Commission and Shanghai Municipal Public Health and Family Planning Commission. These agencies did not participate in the data collection, analyses, interpretation, and writing of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors’ institution received funding from Shanghai Municipal Science and Technology Commission (134119b1400) and Shanghai Municipal Public Health and Family Planning Commission (2013040).