
Abstract
Objective
The purpose of this study was to evaluate the mid-term clinical outcomes of osteochondral autograft transplantation (OAT) with concomitant high tibial osteotomy (HTO) in spontaneous osteonecrosis of the knee (SONK) with a large lesion.
Design
A total of 48 knees of 48 consecutive patients with SONK (lesion size ≥4 cm2, no age criteria) who underwent opening wedge HTO and concomitant OAT were retrospectively investigated, and those who were followed up postoperatively for at least 5 years were included in this case series study. Clinical outcomes were evaluated using knee and function scores of Knee Society Score, radiographic outcomes were evaluated using the anatomical femorotibial angle (FTA), and these outcomes were compared between patients aged ≥70 years and <70 years.
Results
Of the 48 cases, a total of 43 cases were available for review at a minimum of 5 years, and 5 cases were excluded from the analysis. Overall, the mean knee score improved from preoperative 48.8 ± 13.3 to postoperative 87.9 ± 8.6 at 1 year (P < 0.05) and 85.0 ± 10.4 at final follow-up (P < 0.05 vs. preop., N.S. vs. 1 year). The mean function score also improved from preoperative 60.1 ± 10.9 to postoperative 87.3 ± 12.2 at 1 year (P < 0.05) and 84.2 ± 12.4 at final follow-up (P < 0.05 vs. preop., N.S. vs. 1 year). The mean standing FTA was corrected significantly from 181.1° ± 2.7° preoperatively to 169.7° ± 2.4° at 1 year (P < 0.05) and 169.4° ± 3.1° at final follow-up (P < 0.05 vs. preop., N.S. vs. 1 year). There were no significant differences in clinical and radiographic outcomes between patients aged ≥70 years and <70 years. There were 4 cases of lateral hinge fracture around the osteotomy site and 1 case of delayed union. None of the patients underwent revision surgery during the follow-up period (survival rate of 100%).
Conclusions
Mid-term clinical outcomes of patients with SONK who underwent HTO and OAT with a relatively large lesion were good.
Keywords
Introduction
Spontaneous osteonecrosis of the knee (SONK) is a well-defined clinical and pathological entity, mainly involving a single compartment. The lesion of SONK is usually localized in a superficial subchondral area of the medial femoral condyle. 1 It rapidly leads to end-stage osteoarthritis depending on the lesion size, 2 and surgical treatment is often required.
Various surgical procedures including arthroscopic debridement, bone marrow stimulation with drilling or microfracture, core decompression, high tibial osteotomy (HTO), osteochondral autograft transplantation (OAT), osteochondral allograft transplantation, unicompartmental knee arthroplasty, and total knee arthroplasty have been introduced for the treatment of SONK.3-5 Of these surgical options, the optimal one is selected on the basis of the pathological condition. The lesion of SONK is usually limited to the small area of the superficial subchondral tissue in the medial femoral condyle, 6 and articular cartilage of the lateral tibiofemoral and patellofemoral compartments, the anterior cruciate ligament, and the lateral meniscus are intact in most cases. In addition, cases in the advanced stage are likely to show varus knee deformity. 7 In these pathological conditions, joint-preserving surgical procedures with repair of damaged cartilage and valgus correction by HTO are available options.
Joint-preserving management of SONK with a large cartilage lesion is difficult, and replacement surgery is often performed.8,9 However, a recent study investigating cases with SONK for 2 years demonstrated that normal or nearly normal cartilage repair was observed in most large lesions with defect size over 4 cm2 after OAT with concomitant HTO. 10 Whether clinical outcomes are good in these cases with long-term follow-up remains to be elucidated. Furthermore, as SONK occurs more frequently in the elderly population than in the younger population, the effects of age on the results need to be investigated.
The purpose of this study was to evaluate the mid-term clinical outcomes of OAT with concomitant HTO in SONK cases with a large lesion. It was hypothesized that HTO and OAT for SONK with a large lesion would improve clinical outcomes.
Materials and Methods
Patients
A total of 48 knees of 48 consecutive patients with SONK who underwent opening wedge HTO (OWHTO) and concomitant OAT between 2009 and 2016 were retrospectively investigated, and those who were followed up postoperatively for at least 5 years were included in this case series study. The inclusion criterion was painful SONK with lesion ≥4 cm2 localized to the medial femoral condyle (lesion size <4 cm2 was not treated with OAT). The exclusion criteria were patients with severe varus deformity with anatomical varus alignment greater than 5° in a weight-bearing radiograph, flexion contracture greater than 15°, or a history of inflammatory arthritis, joint infection, or corticosteroid intake.
The study protocol and publication were approved by the institutional review board at Yokohama City University (#B180200061). Written informed consent was obtained from all individual participants included in this study.
Surgical Procedure and Postoperative Management
After arthroscopic examination, the lesion of the medial femoral condyle was exposed through subvastus arthrotomy, and debridement of damaged cartilage was performed. Osteochondral plugs (4.5 or 6.5 mm in diameter and 20 mm in depth) were harvested from minimal weight-bearing periphery of the femoral condyles at the level of the patellofemoral joint and transplanted to corresponding burr holes in the cartilage defect using commercially available instruments (Smith and Nephew Inc., Andover, MA). Average 3.4 osteochondral plugs (range, 2-6 plugs) were used depending on the lesion size. OWHTO was performed using an anteromedial approach under fluoroscopic guidance. 11 The amount of angular correction was planned preoperatively aiming to achieve tibiofemoral anatomical valgus of 10° in a 1-leg standing radiograph postoperatively. The osteotomy was started 35 mm below the medial articular surface of the tibia. An oblique osteotomy was performed from the medial cortex to the upper third of the proximal tibiofibular joint using biplanar technique, leaving the tibial tuberosity intact. The osteotomized gap was gradually opened and filled with 2 wedged blocks of beta-tricalcium phosphate with 60% porosity (Osferion; Olympus Terumo Biomaterials. Corp., Tokyo, Japan) and fixed with TomoFix (DePuy Synthes, Zuchwil, Switzerland).
Patients started a postoperative rehabilitation program including isometric quadriceps exercise and range-of-motion exercise the day after surgery. A non-weight-bearing regimen was prescribed for 1 week, followed by partial weight-bearing exercise. Full weight-bearing exercise was permitted 2 weeks postoperatively. Isometric exercise of the quadriceps, gluteus, and hamstrings; active/passive knee full range-of-motion exercise; patella mobilization; and hamstrings and gastrocnemius-soleus stretches were continued. Patients were encouraged to walk with or without the use of a walking aid. Finally, patients achieved step-over-step stair climbing.
Assessment of Clinical and Radiographic Outcomes
Patients were followed up postoperatively every year for clinical and radiographic assessments. Clinical evaluation was carried out using the Knee Society Score (KSS). 12 For radiographic assessment, an anteroposterior weight-bearing radiograph of the knee was taken, and knee alignment was expressed as the anatomical femorotibial angle (FTA), measuring the lateral angle between the anatomical axes of the femur and tibia. The outcomes were assessed between preoperative and postoperative time points. To evaluate the effect of age, clinical outcomes were compared between 2 different age groups (≥70 years vs. <70 years).
Assessment of Articular Cartilage
Second-look arthroscopy was performed in all patients at the time of plate removal, and cartilage repair was evaluated according to the International Cartilage Repair Society (ICRS) repair grade.13,14
Statistical Analysis
Statistical analysis was carried out using BellCurve for Excel version 3.21 (Social Survey Research Information Co., Ltd., Tokyo, Japan). As histograms of the data indicated that the variables had non-normal distributions, nonparametric statistical methods were used to analyze the data. The Friedman test was used to test for significant differences over time points with respect to clinical and radiographic evaluations. When a significant difference was detected, post hoc pairwise tests with Bonferroni correction were applied for multiple comparisons. Pearson’s chi-squared test was used to test for significant differences in the distributions of categorical variables. An adjusted P value <0.05 was considered significant. A post hoc power analysis was performed for comparison of 2 age groups. Consequently, the statistical power was calculated to be 82% for a sample size of 22 and 21 in each group to detect a significant difference with α level of 0.05 and effect size of 0.8.
Results
Details of Follow-Up
Of the 48 cases, 4 were lost to follow-up within 5 years, and 1 patient developed a serious medical disease; these 5 cases were excluded from the analysis. Thus, 43 cases were available for review at a minimum of 5 years, with a mean duration of follow-up of 6.7 years (5-10 years), and were included in the study. Preoperative demographic data are shown in Table 1 .
Patients’ Demographic Data.
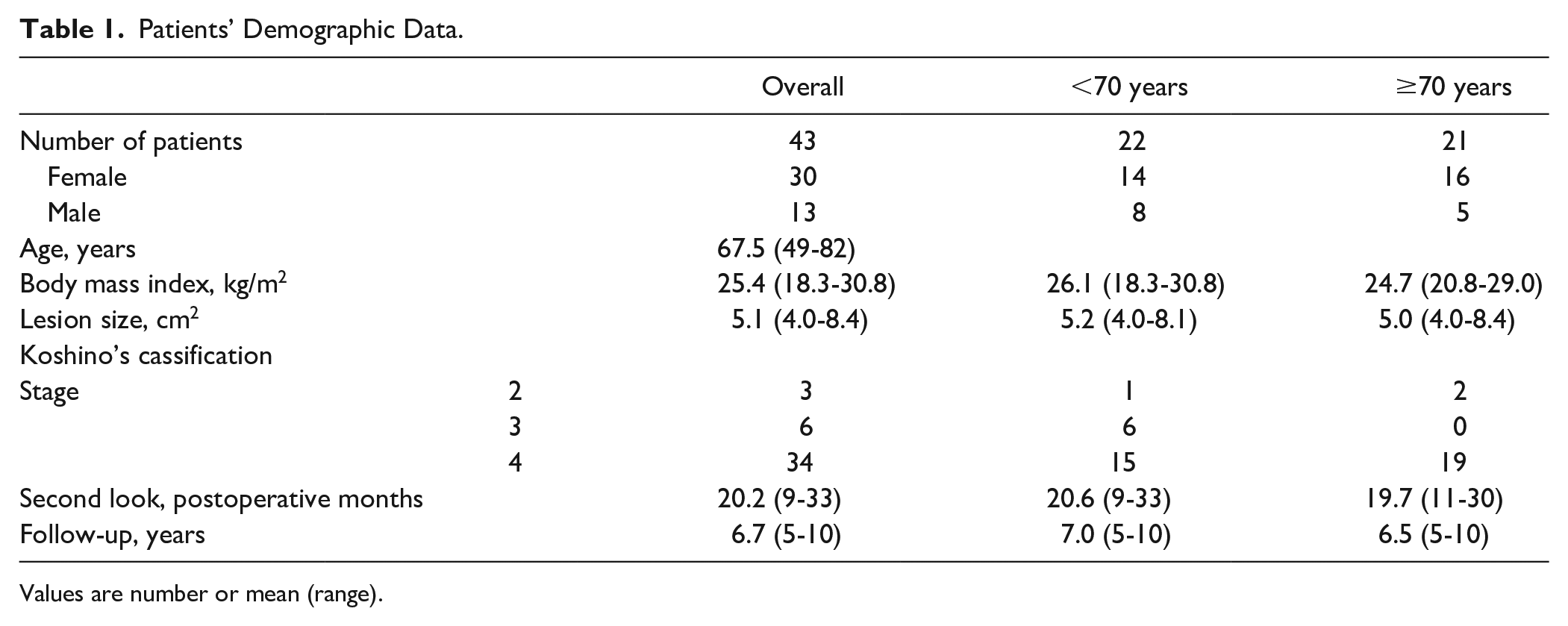
Values are number or mean (range).
Complications
There were 4 cases of lateral hinge fracture around the osteotomy site and 1 case of delayed union. There were no cases that required additional surgical treatment in relation to these complications. No cases had neurovascular injury, wound-healing problems, infection, or venous thromboembolism.
Clinical Outcomes
The KSS results are summarized in Tables 2 and 3 . Overall, the mean knee score improved continuously from a preoperative value of 48.8 ± 13.3 to postoperative values of 87.9 ± 8.6 at 1 year (P < 0.05), 85.0 ± 9.7 at 5 years (P < 0.05), and 85.0 ± 10.4 at final follow-up (P < 0.05). The mean function score also improved continuously from a preoperative value of 60.1 ± 10.9 to postoperative values of 87.3 ± 12.2 at 1 year (P < 0.05), 85.8 ± 11.5 at 5 years (P < 0.05), and 84.2 ± 12.4 at final follow-up (P < 0.05). KSS grading showed that 19 cases (86.4%) with age <70 years and 21 cases (100%) with age ≥70 years were classified as excellent or good at postoperative 5 years. There were no significant differences between the 2 age groups. None of the patients underwent revision surgery during the follow-up period (survival rate of 100%).
Mean Knee Society Scores.
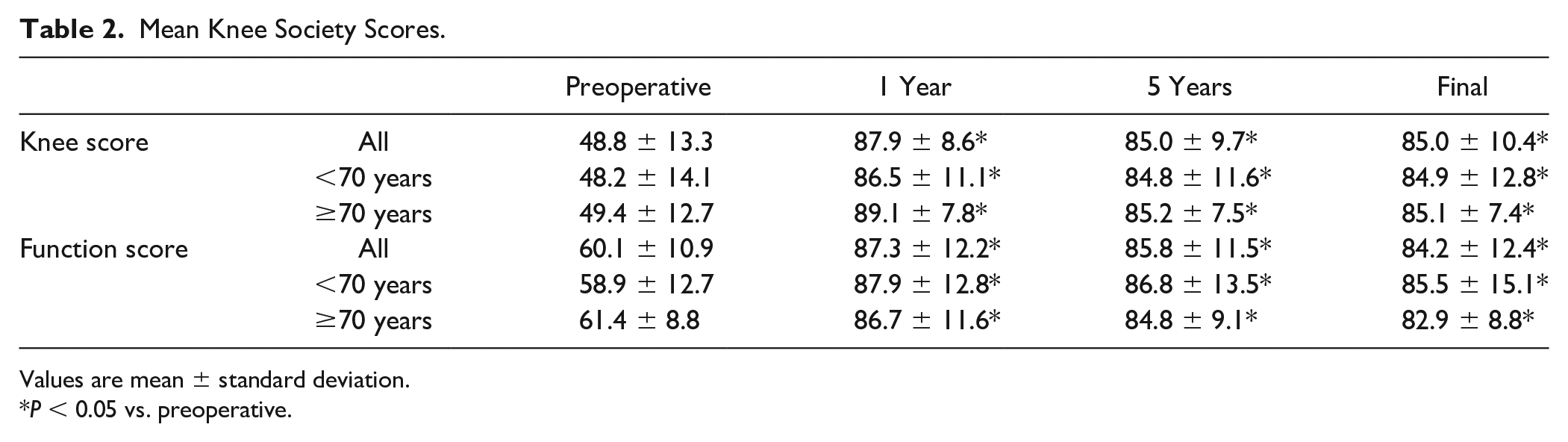
Values are mean ± standard deviation.
P < 0.05 vs. preoperative.
Knee Society Scores Grading.
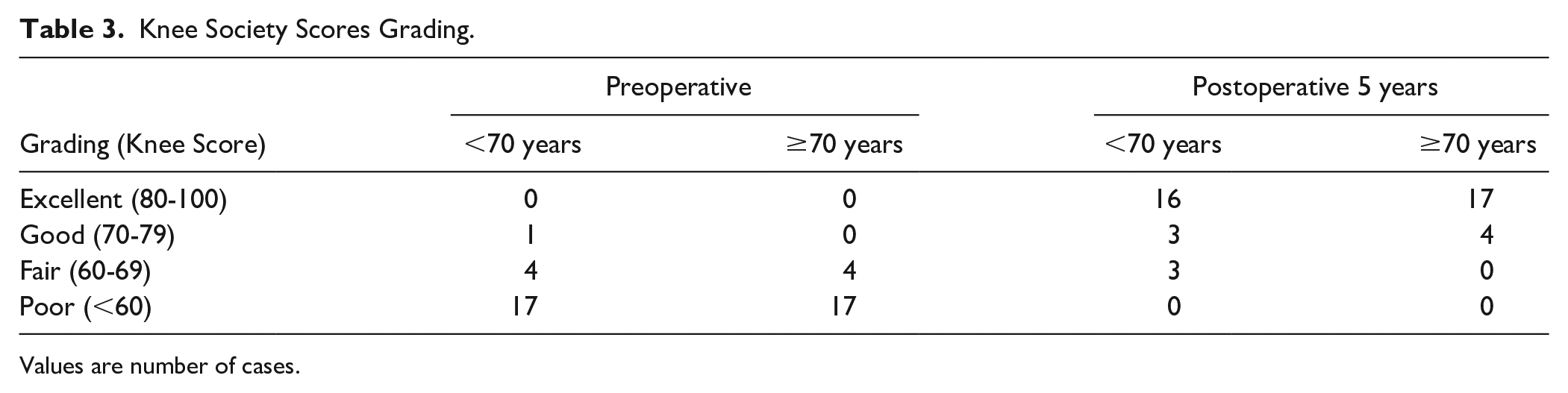
Values are number of cases.
Radiographic Outcomes
The mean standing FTA decreased significantly from 181.1° ± 2.7° preoperatively to 169.7° ± 2.4° at 1 year after surgery ( Table 4 ). The valgus correction in standing FTA was maintained during the follow-up period (169.5° ± 3.0° at 5 years and 169.4° ± 3.1° at final follow-up, N.S. vs. 1 year). There were no significant differences between the 2 age groups. Radiographs of a representative case are shown in Figure 1 .
Mean Standing Femorotibial Angle (Degrees).
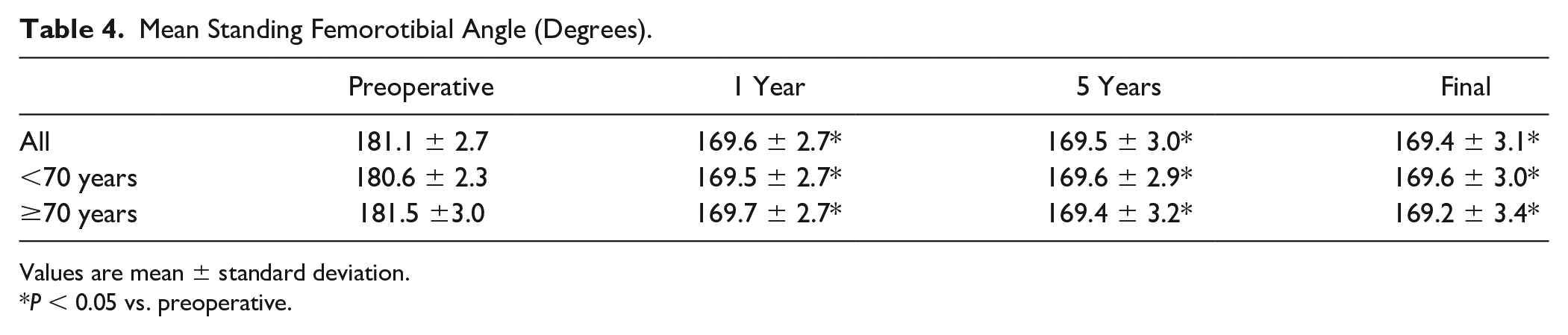
Values are mean ± standard deviation.
P < 0.05 vs. preoperative.
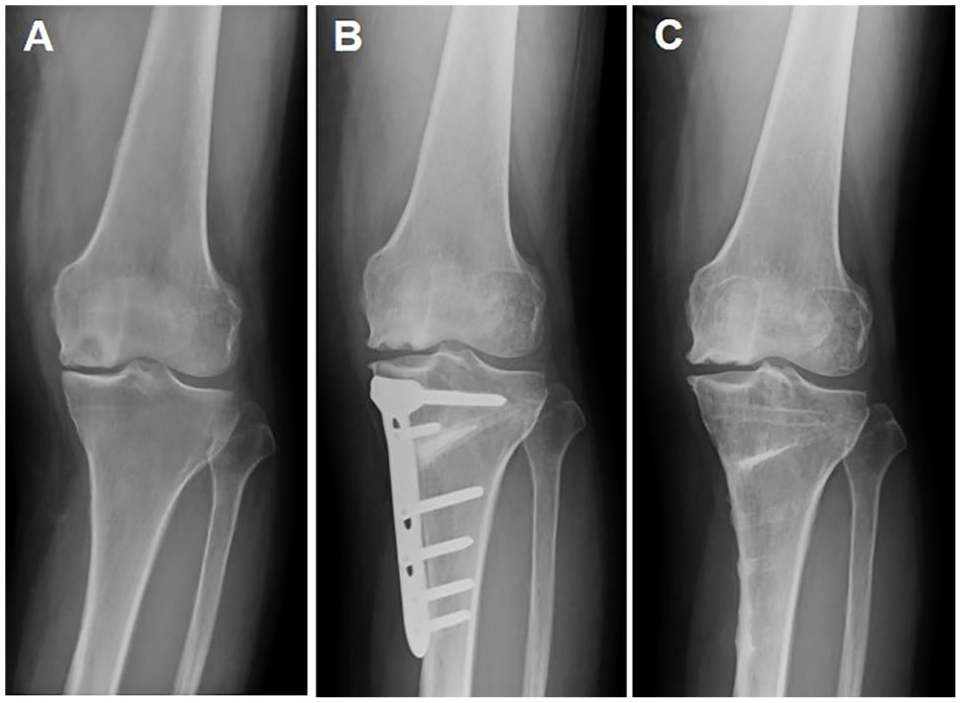
Radiographs of a 72-year-old woman with spontaneous osteonecrosis of the knee who was treated with osteochondral autograft transplantation and opening wedge high tibial osteotomy: (
Cartilage Repair
Postoperative cartilage status at second-look arthroscopy according to the ICRS overall repair grade classification is summarized in Table 5 . Cartilage repair was achieved, being normal or nearly normal in 20 cases (90.9%) with age <70 years and 21 cases (86.1%) with age ≥70 years. There were no significant differences between the 3 age groups. Photographs of a representative case are shown in Figure 2 .
Cartilage Repair Assessment by Second-Look Arthroscopy.
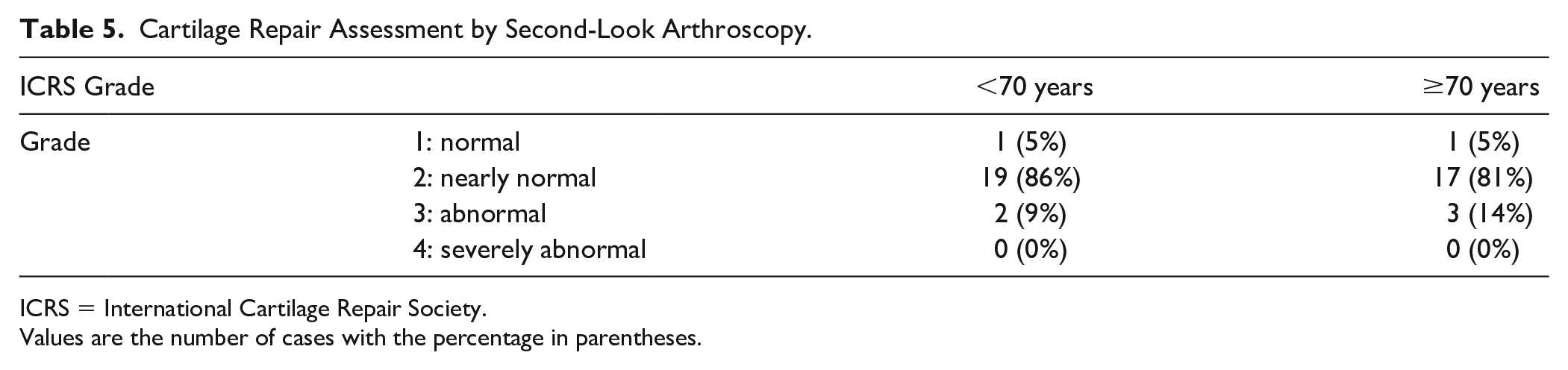
ICRS = International Cartilage Repair Society.
Values are the number of cases with the percentage in parentheses.
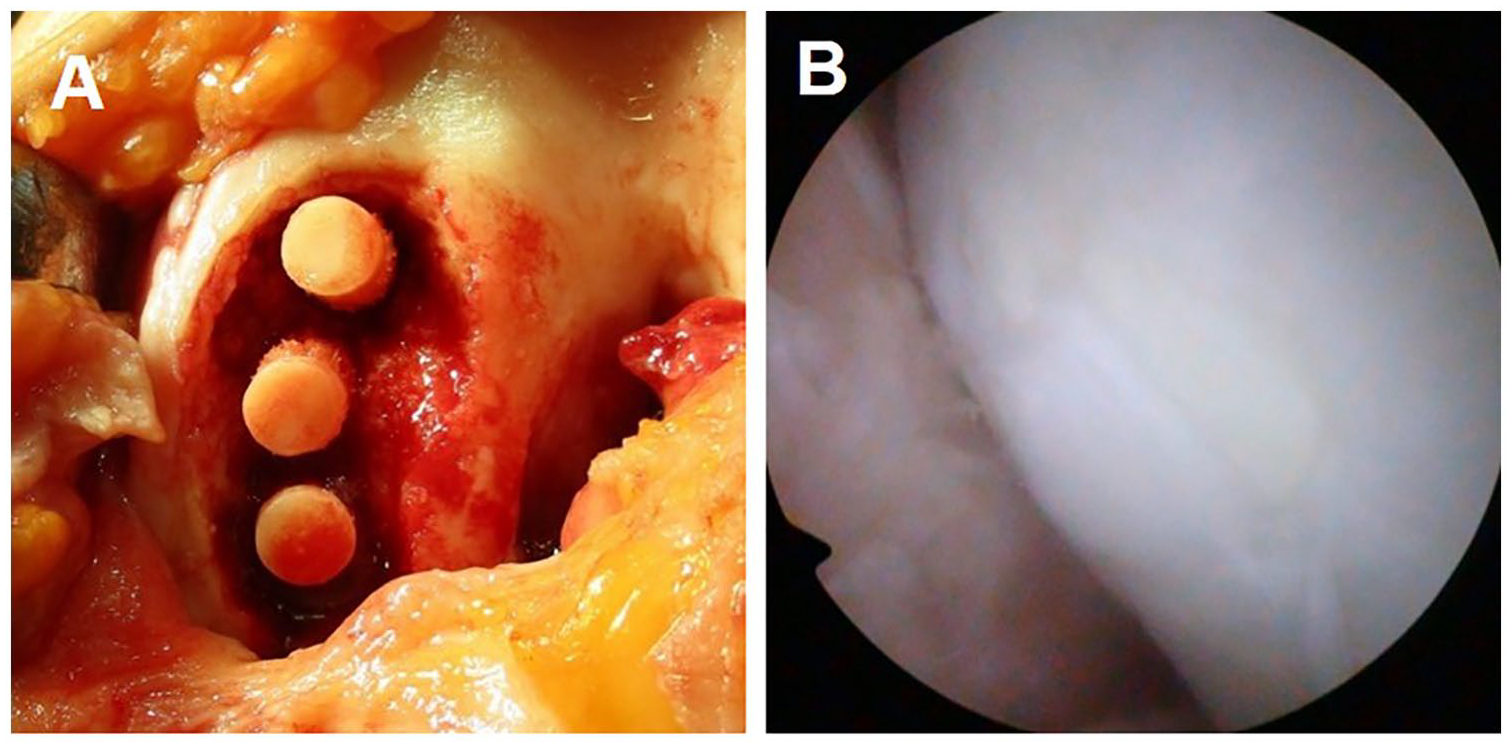
Photographs of a 72-year-old woman with spontaneous osteonecrosis of the knee who was treated with osteochondral autograft transplantation and opening wedge high tibial osteotomy: (
Discussion
This study was intended to describe the impact on the mid-term clinical outcomes of patients with SONK who underwent OWHTO and OAT for a relatively large lesion. The results of the present series support the initial hypothesis that OAT and HTO improve clinical outcomes. The major advance in the present study is the provision of evidence that excellent results are obtained even in older patients with a mean age of 68 years at the time of surgery.
OAT was introduced as a treatment option involving the transplantation of multiple cylindrical osteochondral grafts from the relatively less weight-bearing periphery of the articular surface to the cartilage defect, 15 and it was an option for the treatment of SONK.10,16-18 Better long-term clinical outcomes of isolated OAT than microfracture have been reported in the treatment of focal chondral and osteochondral defects of the weight-bearing area.19,20 However, patients with a cartilage lesion in the medial femoral condyle often show varus knee deformity, and such malalignment is a potential failure risk with an isolated procedure of cartilage repair.21,22 Minzlaff et al. 23 reported that mean survival rates of combined OAT and valgus HTO for deep osteochondral defects of the medial femoral condyle and concomitant varus malalignment >2° were 95% at 5 years, 93% at 7 years, and 90% at 8.5 years. Large cohort data after HTO and cartilage repair versus cartilage repair alone in patients with cartilage defect of the medial compartment of the knee demonstrated that concomitant HTO led to significantly higher satisfaction in patients, and the advantages of accompanying HTO were seen in the group of patients with a varus deformity of 5° or more. 24 Therefore, a concomitant procedure of HTO is recommended with OAT, especially in patients with varus deformity.
The defect size is one of the factors affecting outcomes of cartilage repair procedures.25,26 Determining the indication for surgery based on defect size is controversial in treatment with OAT. Several studies were limited to lesion size of 4 cm2 or less for OAT.27-29 In contrast, good results were shown for relatively large lesions, including those over 4 cm2.30-33 Although the lesion of SONK is usually localized in the limited area of the medial femoral condyle, the size is relatively large in cases requiring surgical treatment. A previous study showed no success in the repair of a necrotic lesion with defect size over 4 cm2 after bone marrow stimulation as a concomitant procedure with HTO, but success of cartilage repair after OAT regardless of the lesion size. 10 In OAT, intact cartilage and bone with viable cells are transplanted in the osteochondral lesion, and the articular surface and subchondral structure are reconstructed with joint congruity. In addition, osteochondral autografts reduce the area of the defect surface, and the gap among osteochondral plugs can be filled with fibrocartilage. The lesion of SONK with or without the collapse of the knee joint can be successfully treated with OAT and HTO.4,10,18 This study supports the treatment strategy for relatively large lesions of SONK by demonstrating good mid-term clinical outcomes after OAT and HTO.
Age has also been discussed as another factor affecting outcomes in the treatment of articular cartilage lesions. A previous study suggested that age was a prognostic factor for cartilage repair, 25 and the inclusion criterion of age was important for better clinical outcomes, with an upper limit of 50 years. 15 In contrast, the cartilage lesion in patients with SONK aged above 50 years could be successfully treated with OAT.10,16-18 Kotani et al. evaluated clinical outcomes of OAT for 16 SONK cases with a mean age of 64.9 years (range, 58-74 years) at a mean follow-up of 67 months. Their results showed good improvement of functional score, especially in patients with an FTA of less than 180°. 16 Tarumi et al. 18 reported significantly improved clinical outcomes and cartilage repair after concomitant HTO and OAT in 23 SONK cases with a mean age of 65.8 years (range, 44-77 years) at a mean follow-up of 72.2 months. These results were comparable to the results of the present study. The present study conducted further investigation regarding the influence of age, and the results showed good mid-term clinical outcomes after OAT and HTO in patients with SONK aged 70 years and above, suggesting that the indication for surgery may not always be limited by age. Controversial findings may be due to disease characteristics and patient activity. The activity level of younger patients is relatively high, and they often require return to high-level athletics. 34 Most patients with SONK are relatively old, and their activity level seems to be generally low. 35 The required level of outcome may differ among these study populations. OAT with concomitant HTO is likely to satisfy the demand of aged patients with SONK to return to their activity level.
This study has several limitations. First, this was a retrospective, nonrandomized, sequential review. Second, the present series included no control group. Third, postoperative arthroscopy was performed only once, and mid-term to long-term cartilage status was unknown. Fourth, there is a lack of comparison with younger patients group as most of the patients in the present study was above 50 years of age.
Conclusions
The present study demonstrated that the clinical outcomes of patients with SONK who underwent HTO and OAT for relatively large lesions were good at mid-term follow-up. OAT with concomitant HTO is a recommended treatment option for patients with SONK, who desire joint preservation.
Footnotes
Authors’ Note
This work was performed at Yokohama City University Hospital.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the institutional review board at Yokohama City University (#B180200061).
Informed Consent
Written, informed consent was obtained from all subjects before the study.