
Abstract
Background:
A lateral hinge fracture is a common complication in medial open wedge high tibial osteotomy (MOWHTO) and is associated with delayed union or nonunion. A comparison of outcomes between patients with or without a lateral hinge fracture after MOWHTO with a structural allograft has not been investigated.
Purpose:
To validate the outcomes of MOWHTO with a structural allograft, especially in the presence of a lateral hinge fracture.
Study Design:
Case series; Level of evidence, 4.
Methods:
We conducted a single-surgeon cohort study at a tertiary referral hospital between April 2017 and August 2022 and included patients who had undergone MOWHTO with a structural allograft for isolated medial compartment osteoarthritis with genu varum. We compared the incidence of delayed union or nonunion events and functional scores between patients with a lateral hinge fracture and those without using the Fisher exact test and independent t test.
Results:
A total of 88 MOWHTO procedures (77 patients) were analyzed. The overall incidence of lateral hinge fractures was 29.5% (n = 26), including type I (n = 20 [22.7%]) and type II (n = 6 [6.8%]). Notably, 42.3% (n = 11) of these fractures had not been detected intraoperatively but during the follow-up visits. The overall Knee Society Score (KSS), Knee Society Score–Function (KSS-F), and Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores were 90.0 ± 10.0, 93.4 ± 10.8, and 93.8 ± 7.1 points, respectively. None of the patients had delayed union or nonunion, and none underwent a reoperation because of bony union problems. The functional scores (KSS, KSS-F, and WOMAC) were not different between patients who had a lateral hinge fracture and those who did not (P > .05).
Conclusion:
The routine use of a structural allograft was associated with satisfactory outcomes after MOWHTO, regardless of whether there was a lateral hinge fracture.
A lateral hinge fracture is one of the most common complications of medial open wedge high tibial osteotomy (MOWHTO) and can lead to construct instability and displacement, delayed union or nonunion, and recurrent varus deformities.5,12 Although a delayed weightbearing protocol has been adopted in patients with a lateral hinge fracture, the incidence of delayed union, nonunion, or reoperations is high.16,22 Therefore, when a lateral hinge fracture is detected intraoperatively, several surgical methods such as adding an opposite screw for fixation with a structural autograft, allograft, or synthetic graft have been utilized to improve structural stability and to avoid adverse outcomes or the need for further surgical interventions.1,2,30
Compared with MOWHTO without a graft, the use of a structural allograft has advantages of improved mechanical properties and may decrease the risk of lateral hinge fractures or failure.2,30 In the presence of a lateral hinge fracture, the use of a structural allograft also provides superior construct stability and more consistent results after cyclic fatigue testing. 2 Consistent with the findings from these biomechanical studies,1,2,30 several studies of MOWHTO with a structural allograft reported satisfactory results with regard to low rates of nonunion or implant failure, ranging between 0% and 4%.9,17,18,23,25,27 However, in many of these series of MOWHTO with a structural allograft, a more conservative delayed weightbearing protocol was adopted.9,18,25,27 In current practice, the efficacy of using a structural allograft in MOWHTO would be more ideally validated in the setting of an early weightbearing protocol. In addition, none of these studies has compared outcomes between patients who had a lateral hinge fracture and those who did not.
In this study, we aimed to validate the effect of using a structural allograft in MOWHTO, especially in patients with a lateral hinge fracture. We hypothesized that (1) the routine use of a structural allograft in MOWHTO would lead to low rates of delayed union or nonunion and satisfactory functional scores and (2) outcomes would not be different between patients who had a lateral hinge fracture and those who did not.
Methods
Data Collection
We conducted this retrospective study at Taipei Veterans General Hospital, a tertiary referral hospital in Taipei. This study was approved by the ethics committee and institutional review board of our hospital. The requirement for informed consent was waived because of the retrospective nature of this study. Between April 2017 and August 2022, we reviewed the medical records and included patients who had undergone MOWHTO with a structural allograft for isolated medial compartment osteoarthritis with genu varum. All the procedures were performed by a single fellowship-trained orthopaedic surgeon (S.-W.T.). During this study period, a structural allograft was used in every patient who underwent MOWHTO. We screened for patients who were eligible for analysis according to the national health insurance procedure codes for corrective osteotomy (PCS-64006B) and bone graft (PCS-64002B) recorded for the same procedure. The exclusion criteria were patients who (1) lacked postoperative lower limb scanograms and (2) did not fulfill a minimum follow-up of 12 months (Figure 1).

Flowchart of patient inclusion. MOWHTO, medial open wedge high tibial osteotomy.
Preoperative Planning and Operative Procedure
A standard lower limb scanogram was utilized for preoperative planning. We measured the mechanical tibiofemoral angle (mTFA), medial proximal tibial angle (MPTA), mechanical lateral distal femoral angle (mLDFA), and joint line convergence angle (JLCA). The Miniaci method was utilized to calculate the opening thickness of the osteotomy site. 15 The designated postoperative weightbearing line was set at 55% to 62.5% of the width of the tibial plateau.
The MOWHTO procedures were performed under spinal or general anesthesia. The adductor canal block was routinely used by the anesthesiologists for postoperative pain management. The patient was placed in a supine position on a radiolucent table. An incision of about 6 cm was made on the medial proximal tibia. The medial collateral ligament and pes anserinus were partially released to facilitate exposure of the osteotomy site and subsequent plate fixation. Under the guidance of intraoperative fluoroscopy, 2 parallel 3.0-mm K-wires were inserted from a point about 4 to 5 cm below the medial joint line toward the hinge point about 2 cm below the lateral joint line. One-plane osteotomy was performed using an oscillating saw and an osteotome. An angle ruler was inserted to gradually create an opening over the osteotomy site. A triangular, wedge-shaped structural allograft was made from a femoral head allograft and was plugged into the osteotomy site. The cortical margin of the femoral head wedge was aligned with the medial border of the tibial osteotomy site to ensure the correct opening thickness and optimal structural support. The thickness of the graft was determined preoperatively. A nonlocking buttress plate (Syntec Scientific) or a Tomofix locking plate (DePuy Synthes) was then used for fixation. Our national health insurance system covers the cost of nonlocking buttress plates for MOWHTO procedures. However, patients are responsible for out-of-pocket costs if they choose to use a locking plate for MOWHTO. The choice between a nonlocking buttress plate and a locking plate was made by the patient preoperatively. Finally, we placed a Hemovac drain (Zimmer Biomet) and closed the wound. Immediate postoperative radiographs were examined in the postanesthesia care unit.
Postoperative Care Protocol
All patients were instructed to walk with a walker or crutches on postoperative day 1. The Foley catheter was removed on postoperative day 1, and the Hemovac drain was removed on postoperative day 2. Because of the use of allografts, prophylactic antibiotics (cefazolin or clindamycin) were given for 2 days until the drain was removed. Patients were usually discharged on postoperative day 3. Outpatient visits were arranged at 2 weeks, 6 weeks, 3 months, 6 months, 12 months, and then annually. We examined radiographs at every outpatient visit starting from 6 weeks postoperatively. For patients who were fixed with a nonlocking buttress plate, 70% partial weightbearing was allowed in the first 6 weeks, followed by weightbearing without restrictions thereafter. For patients who were fixed with a locking plate, weightbearing without restrictions was allowed immediately after the procedure. This weightbearing protocol remained the same even if a lateral hinge fracture was observed intraoperatively, on immediate postoperative radiographs, or during the follow-up visits.
Outcome Measures
In this study, we compared the outcomes between patients who had a lateral hinge fracture and those who did not. The primary outcome was the incidence of delayed union or nonunion events. We adopted the definition of bone union after MOWHTO with an allograft according to the modified van Hemert rating system.13,24 The assessment of bone union patterns in the opening gap was conducted by outlining a triangle along the edges and corners of the osteotomy site in the anterior-posterior view. This involved dividing the osteotomy site into 5 zones, each representing 20% of the osteotomy site length along the base from the lateral side. Bone union was defined as phase 4 or 5 findings at zone 3, involving blurred or nonvisible lucent lines between either surface of the allograft and host bone without sclerotic margins at the periphery of the wedge opening.13,24 Delayed union was defined as failure to achieve union by 6 months postoperatively. Nonunion was defined as failure to achieve union at a minimum of 9 months, without signs of healing for a consecutive 3 months. 3 Additionally, we recorded the time to union in weeks. The secondary outcomes were functional scores, including those for the Knee Society Score (KSS), the Knee Society Score–Function (KSS-F), and the Western Ontario and McMaster Universities Arthritis Index (WOMAC).
Statistical Analysis
We performed analyses using SPSS software (Version 25.0; IBM). Descriptive statistics were calculated for all available data. The chi-square or Fisher exact test was used to compare categorical variables where appropriate. The independent t test was used to compare continuous variables. The significance level was .05. We performed multivariate regression analyses to validate the association between the presence of a lateral hinge fracture and the outcomes. Factors that were considered in the multivariate linear regression models included age, sex, body mass index (BMI), smoking, type of plate, opening thickness, presence of a lateral hinge fracture, and type of hinge fracture. The backward variable selection method was employed to choose the optimal model, with significance for a risk factor at the level of .05. The results were expressed as β coefficients with 95% confidence intervals.
Results
Patient Characteristics
We included 77 patients (88 procedures) who underwent MOWHTO with a structural allograft using a nonlocking buttress plate (n = 58) or locking plate (n = 30). Overall, the mean age and BMI were 53.5 ± 7.3 years and 26.5 ± 4.0 kg/m2, respectively. A slightly higher proportion of this cohort was female (53.4%). A smoking habit was recorded in 18.2% of the cohort. The mean follow-up duration was 43.9 ± 16.9 months (range, 12-76 months). The patient characteristics were not different between those who had a lateral hinge fracture and those who did not (P > .05) (Table 1). Data on hemoglobin level, estimated blood loss, transfusion, and length of stay are provided in Appendix Table A1.
Patient Characteristics a
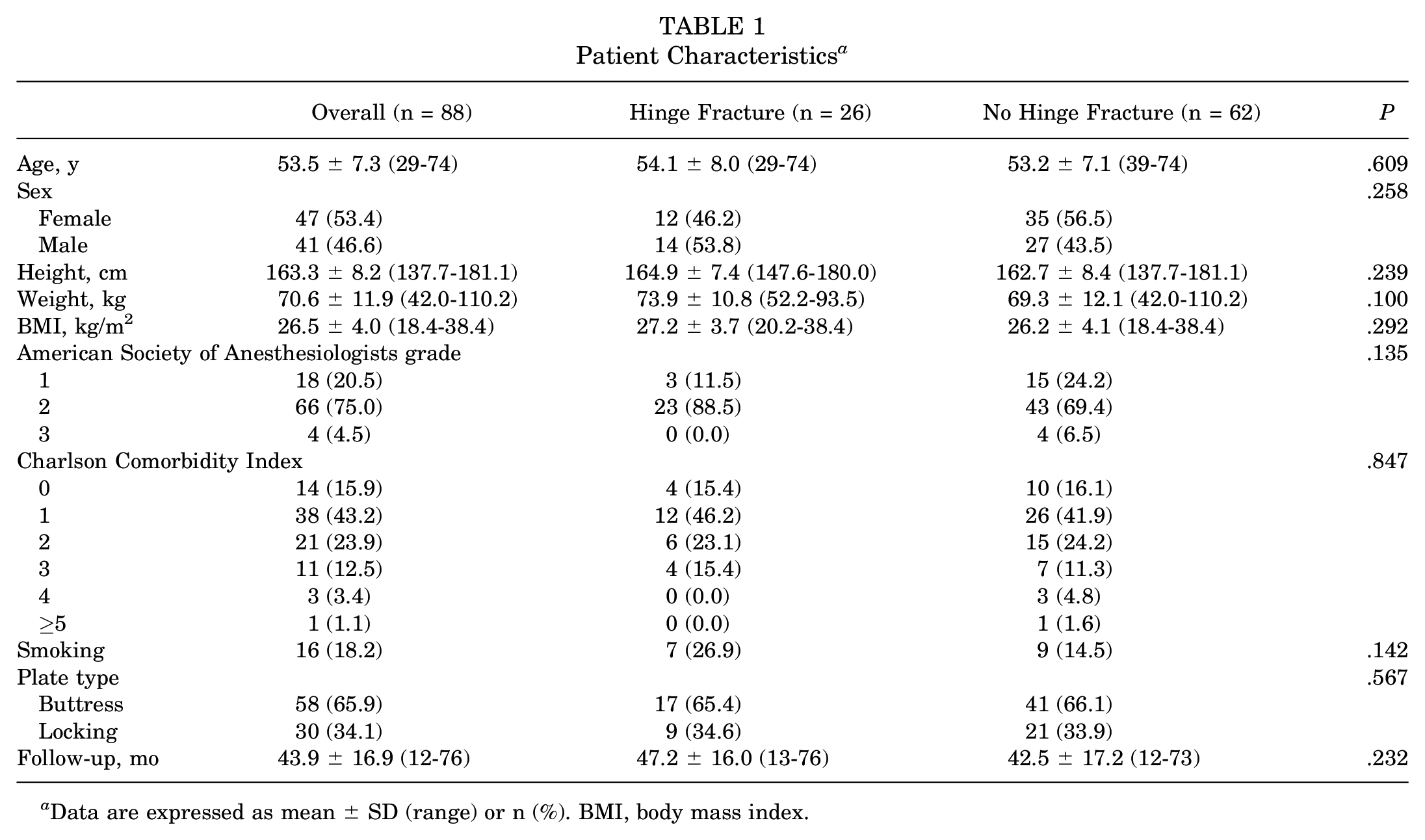
Data are expressed as mean ± SD (range) or n (%). BMI, body mass index.
Radiographic and Functional Outcomes
The mean preoperative mTFA, MPTA, mLDFA, and JLCA were −7.4°± 3.1°, 84.6°± 2.6°, 87.6°± 1.4°, and 3.1°± 2.0°, respectively. The mean postoperative mTFA, MPTA, mLDFA, and JLCA were 1.5°± 2.3°, 91.7°± 2.1°, 87.5°± 1.5°, and 2.0°± 1.5°, respectively. The preoperative and postoperative radiographic parameters, including opening thickness, mTFA, MPTA, mLDFA, and JCLA, were not different between patients who had a lateral hinge fracture and those who did not (P > .05). A lateral hinge fracture occurred in 26 procedures (29.5%), and 42.3% (n = 11) of these fractures were not detected intraoperatively but during the subsequent follow-up visits (Figures 2 and 3). In terms of the Takeuchi classification for hinge fractures, 22 there were 20 (76.9%) type I and 6 (23.1%) type II fractures (Table 2).

A 49-year-old female patient with left knee osteoarthritis who underwent medial open wedge high tibial osteotomy with a buttress plate and structural allograft. (A) Preoperative radiograph. (B) Immediate postoperative radiograph. A lateral hinge fracture was not observed. (C) Radiograph at 6 weeks postoperatively. A type I lateral hinge fracture was noted. (D) Bone union at 4 months postoperatively.

A 56-year-old male patient with right knee osteoarthritis who underwent medial open wedge high tibial osteotomy with a buttress plate and structural allograft. (A) Preoperative radiograph. (B) Immediate postoperative radiograph. A lateral hinge fracture was not observed. (C) Radiograph at 2 months postoperatively. A type II lateral hinge fracture was noted. (D) Bone union at 5 months postoperatively.
Radiographic and Functional Outcomes a

Data are expressed as mean ± SD (range) or n (%). JLCA, joint line convergence angle; KSS, Knee Society Score; KSS-F, Knee Society Score–Function; mLDFA, mechanical lateral distal femoral angle; MPTA, medial proximal tibial angle; mTFA, mechanical tibiofemoral angle; WOMAC, Western Ontario and McMaster Universities Arthritis Index. Dashes indicate not applicable.
Overall, the mean KSS, KSS-F, and WOMAC scores were 90.0 ± 10.0, 93.4 ± 10.8, and 93.8 ± 7.1 points, respectively. The functional scores (KSS, KSS-F, and WOMAC) were not different between patients who had a lateral hinge fracture and those who did not (P > .05). All patients achieved union at the osteotomy site within a mean duration of 16.4 ± 5.1 weeks. None of the patients experienced delayed union or nonunion or required subsequent procedures for bone union problems. The mean time to union was not different between patients with a lateral hinge fracture and those without (17.1 ± 5.4 vs 16.1 ± 5.0 weeks, respectively; P > .05) (Table 2). In addition, there was no significant difference in the time to union between plate types (locking plate vs nonlocking buttress plate: 17.3 ± 5.1 vs 15.9 ± 5.0 weeks, respectively; P > .05). According to the classification of complications after MOWHTO proposed by Martin et al, 14 all the lateral hinge fractures in this study were categorized as class I (n = 26 [29.5%]), requiring no additional treatment or alterations in postoperative care. No class II or III complications were observed that necessitated extended nonoperative treatment or additional surgery.
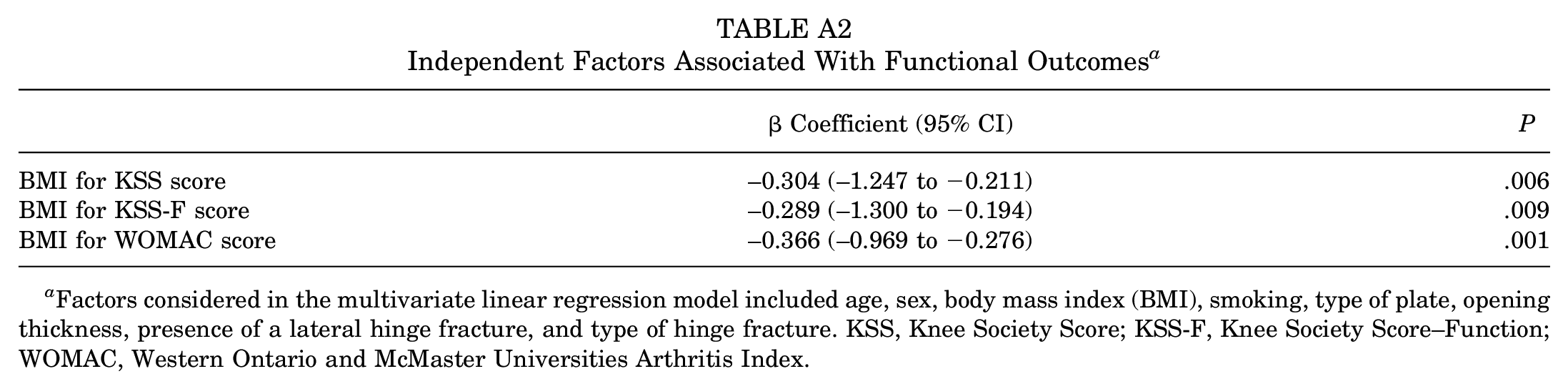
Multivariate regression analysis could not be performed on the primary outcome because there were no delayed union or nonunion events in this series. The results from multivariate linear regression analyses revealed that a higher BMI was associated with lower KSS scores (β coefficient = −0.304 [95% CI, −1.247 to −0.211]), KSS-F scores (β coefficient = −0.289 [95% CI, −1.300 to −0.194]), and WOMAC scores (β coefficient = −0.366 [95% CI, −0.969 to −0.276]). The presence of a lateral hinge fracture, the type of hinge fracture, and the type of plate were not risk factors for the outcomes (Appendix Table A2).
Discussion
The most important findings of this study were that (1) all patients who underwent MOWHTO with a structural allograft had uneventful bone union and satisfactory functional results (mean KSS, KSS-F, and WOMAC scores: 90.0 ± 10.0, 93.4 ± 10.8, and 93.8 ± 7.1 points, respectively) and (2) there were similar radiographic and functional outcomes between patients who had a lateral hinge fracture and those who did not (Table 2).
A lateral hinge fracture is a common complication after MOWHTO and can lead to construct instability, displacement, delayed union or nonunion, and the recurrence of varus deformities. Its incidence varies from 3% to 30%.5,12 To avoid adverse outcomes after a lateral hinge fracture, several reinforcement strategies such as additional opposite screw fixation and bone graft augmentation have been validated to improve structural stability in several biomechanical studies and finite element analyses.1,2,30 The use of a structural allograft has shown biomechanical advantages such as higher stiffness, reduced stress of the lateral tibial cortex and the implant, decreased maximum displacement of the tibia, relative displacement of the medial gap, and decreased risk of implant failure and lateral hinge fractures.1,30 In the presence of a lateral hinge fracture, patients with a structural allograft demonstrated the ability to withstand higher peak forces and had lower valgus malrotation, higher stiffness, and more consistent results from cyclic fatigue testing compared with those without bone grafts. 2 However, to fill the osteotomy gap with a structural allograft only when a lateral hinge fracture is recognized intraoperatively might not be an effective strategy. That is because a high proportion (38.5%-47.6%) of lateral hinge fractures have not been identified intraoperatively but rather during follow-up visits at 6 weeks, 3 months, or even up to 6 months.4,8,14,20 In this study, all patients who underwent MOWHTO with a structural allograft achieved uneventful union at the osteotomy site, regardless of the type of plate or the presence of a lateral hinge fracture.
Early mobilization and weightbearing in patients who have undergone MOWHTO help to prevent venous thromboembolism and improve early functional outcomes. 11 Several earlier series of MOWHTO with structural allografts have revealed low rates of nonunion or implant failure (0%-4%).9,18,25,27 However, these studies had delayed rehabilitation protocols, including nonweightbearing for at least 6 to 8 weeks,25,27 partial weightbearing after 6 weeks, 18 or the use of an immobilizer brace for 6 weeks. 9 In our study, immediate weightbearing without restrictions and 70% partial weightbearing were allowed in patients who underwent MOWHTO with a locking plate and nonlocking buttress plate, respectively. There were no delayed union or nonunion events. Our results were similar to those of 2 recent series of MOWHTO with structural allografts that adopted an early weightbearing protocol. The rates of nonunion or implant failure were low (0%-2%).17,23 Notably, none of these studies focused on outcomes and changes in weightbearing protocols in patients who had a lateral hinge fracture.9,18,23,25,27 Delayed weightbearing protocols were usually adopted in patients who had a lateral hinge fracture, especially unstable ones (Takeuchi type II or III).19,21 Nevertheless, the incidence of delayed union or nonunion was high.16,22 Nakamura et al 16 assessed 74 patients who underwent MOWHTO without a graft. Type I, II, and III hinge fractures were noted in 7, 2, and 6 patients, respectively. Patients who had a type I or II hinge fracture followed a standard protocol of partial and full weightbearing at 1 and 3 weeks postoperatively, respectively. Patients with a type III hinge fracture followed a delayed protocol of partial and full weightbearing at 3 and 6 weeks postoperatively, respectively. The rates of delayed union or nonunion after type I, II, and III hinge fractures were 14.3%, 100%, and 33%, respectively. 16 Takeuchi et al 22 examined 93 patients who underwent MOWHTO with a synthetic bone graft. There were 19 type I, 5 type II, and 2 type III lateral hinge fractures. Patients who had a type I or II hinge fracture followed a protocol of nonweightbearing and partial weightbearing at 1 and 2 weeks postoperatively, respectively. Patients with a type III hinge fracture adopted a protocol of nonweightbearing for 2 weeks, followed by partial weightbearing thereafter. A total of 2 patients (40%) with a type II hinge fracture had delayed union and shifted to a nonweightbearing protocol. 22
During our procedure, we select femoral head grafts from patients with hip osteoarthritis. A femoral head wedge is harvested from the area with significant subchondral sclerosis. We ensure that the cortex of the femoral head wedge is well aligned with the medial cortical border of the tibial osteotomy site to optimize the quality of support.
Compared with the use of a structural autograft, the allograft has several advantages, including no need for additional harvesting procedures and no donor site morbidity. However, a potential concern is the risk of infections.7,29 The rates of surgical site infections or deep infections after the use of an allograft in MOWHTO are low (1.7%-1.9%).10,23,28 The standard procurement, processing, preservation, and storage of allografts, as well as the use of prophylactic antibiotics after MOWHTO, are appropriate measures to avoid allograft-related infections.6,29 The duration of prophylactic antibiotic use in our patients was slightly longer (cefazolin or clindamycin; 2 days), and none of them had surgical site complications or deep infections. Notably, the additional cost associated with using a structural allograft should be considered as a drawback of this augmentation modality. 26
Limitations
There were several limitations of this study. First, this was a retrospective study with a relatively small sample size. Second, during this study period, we filled the gap with a structural allograft in every MOWHTO procedure. Therefore, we were not able to make comparisons between the use of an allograft, autograft, or no bone graft. A randomized controlled trial is warranted to compare the outcomes of these bone graft options, especially in the presence of a lateral hinge fracture.
Conclusion
The routine use of a structural allograft was associated with satisfactory radiographic and functional outcomes after MOWHTO, regardless of whether there was a lateral hinge fracture.
Footnotes
Appendix
Independent Factors Associated With Functional Outcomes a
| β Coefficient (95% CI) | P | |
|---|---|---|
| BMI for KSS score | −0.304 (–1.247 to −0.211) | .006 |
| BMI for KSS-F score | −0.289 (–1.300 to −0.194) | .009 |
| BMI for WOMAC score | −0.366 (–0.969 to −0.276) | .001 |
Factors considered in the multivariate linear regression model included age, sex, body mass index (BMI), smoking, type of plate, opening thickness, presence of a lateral hinge fracture, and type of hinge fracture. KSS, Knee Society Score; KSS-F, Knee Society Score–Function; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Final revision submitted March 17, 2024; accepted April 4, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Taipei Veterans General Hospital (2023-11-009AC).