
Abstract
Background:
Few clinical studies have reported the predictors of lateral hinge fracture (LHF) after medial opening-wedge high tibial osteotomy (MOWHTO).
Purpose/Hypothesis:
The purpose was to compare the incidence of LHF on plain radiographs versus computed tomography (CT) scans and to investigate the factors related to the development of LHF after MOWHTO. We hypothesized that (1) a higher LHF detection rate would be seen on CT scans versus plain radiographs and (2) LHF incidence would be related to opening gap width and hinge position.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A total of 97 MOWHTO cases were included. The presence and types of LHF were determined from plain radiographs and CT scans. Radiographic parameters were measured on plain radiographs taken 6 weeks postoperatively. Anterior and posterior opening gap widths, coronal and sagittal osteotomy slopes, and fibular height were calculated from CT scans. The wedge-hinge relationship and the zone of hinge position were assessed, and the patient and radiographic factors related to LHF occurrence were evaluated.
Results:
Seventeen LHF cases (20.5%) were detected on plain radiographs, while significantly more (37 cases; 44.6%) were found on CT scans (P = .001). Based on Takeuchi classification, 28 LHF cases were considered type 1, 7 were type 2, and 2 were type 3. Logistic regression analysis revealed that opening gap width (odds ratio, 1.615; 95% confidence interval, 1.232-2.118; P = .001) and posterior opening gap width (odds ratio, 3.731; 95% confidence interval, 1.642-4.351; P = .008,) differed significantly between patients with versus without LHF. Other patient and radiographic factors were not significantly related to LHF occurrence. Receiver operating characteristic curve analysis identified the opening gap width cutoff values for LHF as 11.0 mm (area under the curve, 0.81; sensitivity, 78.4%; specificity, 73.9%).
Conclusion:
The incidence of LHF after MOWHTO can be underestimated on plain radiographs compared with CT scans. Only large opening gap width, especially posterior gap width, was found to have a statistically significant relationship with occurrence of LHF. Therefore, special caution for possible LHF may be needed if a large correction is planned.
Keywords
Medial opening-wedge high tibial osteotomy (MOWHTO) is simple to perform and allows precise adjustment of correction angle. 13 However, it is associated with a major risk of intraoperative lateral hinge fracture (LHF). 7,9,12,27,35,38,40 The reported incidence of LHF after MOWHTO ranges from 0.3% to 35%. 1,8,22,25,31,36,38,39 Previous studies have reported that LHF is a major cause of instability, leading to serious complications such as malunion and nonunion. 11,23,24,34,38 Generally, MOWHTO is performed using the elasticity of the lateral cortex as a biomechanical stabilizer. But excessive opening gaps beyond elasticity increase the risk of LHF. 28,38,39 To prevent LHF, the lateral hinge should be left with continuity targeting the upper-third of the proximal tibiofibular joint. 3,37 A variety of ideal hinge positions have been described in previous studies. 7,26,38,40 In addition, various factors affecting LHF, such as fibular position, osteotomy gap height, and wedge-hinge relationship, have been introduced. 6,15,26,29 However, data regarding the predictors of LHF are lacking.
LHF is mainly detected using intraoperative fluoroscopy or plain radiography immediately after surgery, but it may not be detected in some undisplaced fractures. Computed tomography (CT) can be used as a complementary diagnostic tool, but controversy remains about the usefulness of postoperative CT for the diagnosis of LHF. 16,19,20
In the current study, we aimed to compare the incidence of LHF on plain radiographs versus CT scans as well as investigate the factors related to the development of LHF after MOWHTO. We hypothesized that (1) a higher LHF detection rate would be seen on CT scans versus plain radiographs and (2) LHF incidence would be related to opening gap width and hinge position.
Methods
Study Population
The study protocol was approved by our institutional review board. We enrolled 97 knees (81 patients) and collected data retrospectively. All surgeries were performed by a single surgeon (W.C.) between January 2016 and December 2019. The primary surgical indication was symptomatic medial compartment osteoarthritis with varus malalignment. Lateral compartment arthritis, inflammatory arthritis, and flexion contractures >15° were contraindications. Patients who underwent MOWHTO and who underwent CT scans within 2 weeks after surgery were included in the study. The exclusion criteria were as follows: (1) age >65 years, (2) revision surgery, (3) low-quality CT scans, and (4) concomitant tibial tuberosity osteotomy and ligament surgery. From an initial 97 knees, 14 knees were excluded because of the selection criteria, leaving 83 knees (70 patients) enrolled in the present study (Figure 1). Patient characteristics and imaging parameters were compared between patients with LHF and those without LHF.

Flowchart of the study population that had open wedge HTO and CT scans. CT, computed tomography; HTO, high tibial osteotomy.
Surgical Technique and Postoperative Rehabilitation
Conventional biplanar MOWHTO was performed under fluoroscopic control after concomitant arthroscopic procedures. During the approach, the superficial medial collateral ligament tibial attachment was partially reflected until the posteromedial cortex of the proximal tibia bone was exposed, and the pes anserinus was retracted distally. The osteotomy was performed using osteotomes, and a calibrated distractor was used to open the osteotomy site to achieve the target hip-knee-ankle axis of 3° valgus, as planned preoperatively. 18 The intraoperative alignment was confirmed under fluoroscopy using an alignment rod through a line intersecting the knee joint between the center of the femoral head and the ankle joint center. 30 Fixation of the osteotomy was performed using an anatomic locking plate (Tomofix; Depuy Synthes) without a gap filler. Patients were encouraged to start passive range of knee motion and active quadriceps strengthening exercises the day after surgery with hinged knee brace protection. Partial weightbearing with crutches and a brace was maintained for 4 weeks, followed by full weightbearing as tolerated. Patients with Takeuchi classification 38 types 2 and 3 LHF kept partial weightbearing until 12 weeks.
Imaging Evaluation
For imaging evaluation, anteroposterior and lateral weightbearing plain radiographs were taken at 6 weeks postoperatively, and a CT scan was performed within 2 weeks postoperatively to evaluate LHF and type. Radiographic parameters were measured twice by 2 orthopaedic surgeons (W.C., S.-J.L.) at an interval of 8 weeks using a picture archiving and communication system (Maroview; Marotech); all measurements were calibrated using a standardized round marker. Safe zone achievement and opening gap width were measured on radiographs, and anterior and posterior opening gap widths, coronal and sagittal osteotomy slopes, and fibular height were calculated on CT scans. Also, the wedge-hinge relationship and the zone of hinge position were evaluated on both coronal and axial CT. LHF was assessed on both imaging modalities, and the cases were divided into 3 types using the Takeuchi classification (Figure 2). 38

Takeuchi classification of lateral hinge fracture. 38 The arrow indicates the fracture site. Type 1, the fracture reaches just proximal to or within the tibiofibular joint; type 2, the fracture reaches the distal portion of the proximal tibiofibular joint; and type 3, a lateral plateau fracture.
The osteotomy gap width was defined as the distance between the 2 medial edges of the osteotomy margin. The safe zone was defined as the shortest distance from the fibular styloid base to the fibular tip (Figure 3A). 4 Fibular height was measured on CT scans as the distance from the base of the fibular styloid process to the lateral tibial plateau on a coronal image, which showed the entire articular surface of the proximal tibiofibular joint (Figure 3B). 7 The coronal and sagittal osteotomy slopes were measured using the angle between a line perpendicular to the tibial shaft axis and the distal osteotomy margin on each CT view (Figure 3C). 19 The anterior and posterior gap widths between the edges of the 2 osteotomy margins were measured on the image of the anteromedial osteotomy edge of biplanar osteotomy on sagittal CT scans (Figure 3D). 33 The wedge-hinge relationship and the hinge position were divided as described by Ogawa et al, 32 as follows. The type of osteotomy was classified according to the pattern of its extent in relation to an anteroposterior line tangential to the medial edge of the head of the fibula on the axial CT scans: type A, both anterior and posterior osteotomies extend over the lateral zone; type B, only the anterior osteotomy extends; type C, only the posterior osteotomy extends; and type D, neither osteotomy extends (Figure 4). The hinge level was classified as high, mid, or low using the intersection of the sclerotic line of osteotomy on CT scans according to the height of the endpoint, based on the proximal and distal margin of the proximal tibiofibular joint (PTFJ) (Figure 5).

(A) The safe zone (SZ) on radiograph, defined as the distance from the circumference line of the fibular head to the fibular tip. The asterisk indicates the medial opening gap width, measured as the distance between the 2 medial edges of the osteotomy margin. (B) The fibular height (FH) on CT scan, calculated as the distance from the circumference line of the fibular head to the lateral tibial plateau. (C) Coronal slope (CS; left) and sagittal slope (SS; right), assessed as the angle between a line perpendicular to the tibial shaft axis and the distal osteotomy margin on the appropriate CT view. (D) Anterior gap (AG) and posterior gap (PG) widths. On the image slice showing the anteromedial osteotomy edge in sagittal view, anterior and posterior gap widths were measured between the edges of the 2 osteotomy margins. CT, computed tomography.

Classification of wedge-hinge relationship. Type A, both anterior and posterior osteotomies extend over the lateral zone; type B, only the anterior osteotomy extends; type C, only the posterior osteotomy extends; and type D, neither osteotomy extends.

Zone classification of hinge position. The hinge level was classified according to the height of the endpoints, with levels high (H), mid (M), and low (L) based on the proximal and distal margin of the proximal tibiofibular joint.
Statistical Analysis
The Kolmogorov-Smirnov test was used to assess distribution. Patient characteristics and radiologic parameters were compared between patients with versus without LHF using paired Student t tests. Descriptive statistics were calculated as means with standard deviations and ranges. Univariate and multivariate logistic regression analysis with a forward elimination method was performed to evaluate factors related to LHF with a 95% confidence interval. For categorical variables, we recoded them to dummy variables and performed regression analysis. In addition, the Fisher exact test was performed to evaluate the relationship of the LHF and sufficient osteotomy (sufficient group [type A] vs insufficient groups [types B-D]). Intra- and interobserver reliability were evaluated by calculating the intraclass correlation coefficient and Cohen kappa coefficient between the measurements by the 2 surgeons. The data were analyzed using PASW SPSS Version 22.0 (IBM Corp). P values <.05 were defined as significant. Given the retrospective nature of the study, we could not perform a priori sample size analysis. Instead, a post hoc power analysis was done using G*Power Version 3.0.10 (Heinrich-Heine-University).
Results
Of the 83 knees included in the study, 46 did not have an LHF, and 37 had an LHF. The mean follow-up duration was 2.7 ± 0.4 years (range, 2.2-3.0 years). The patient characteristics and imaging parameters are shown in Table 1. Age, sex, side, height, weight, and body mass index were not significantly different between the 2 groups. Inter- and intraobserver reliabilities were satisfactory on each parameter (Table 2).
Descriptive Data and Radiologic Parameters a

a Data are reported as mean ± SD (range) unless otherwise indicated. Dashes indicate not applicable. Bolded P values indicate statistically significant difference between groups (P < .05). CT, computed tomography; LHF, lateral hinge fracture; XR, radiograph.
ICC and Cohen Kappa Values for Intra- and Interobserver Reliability a
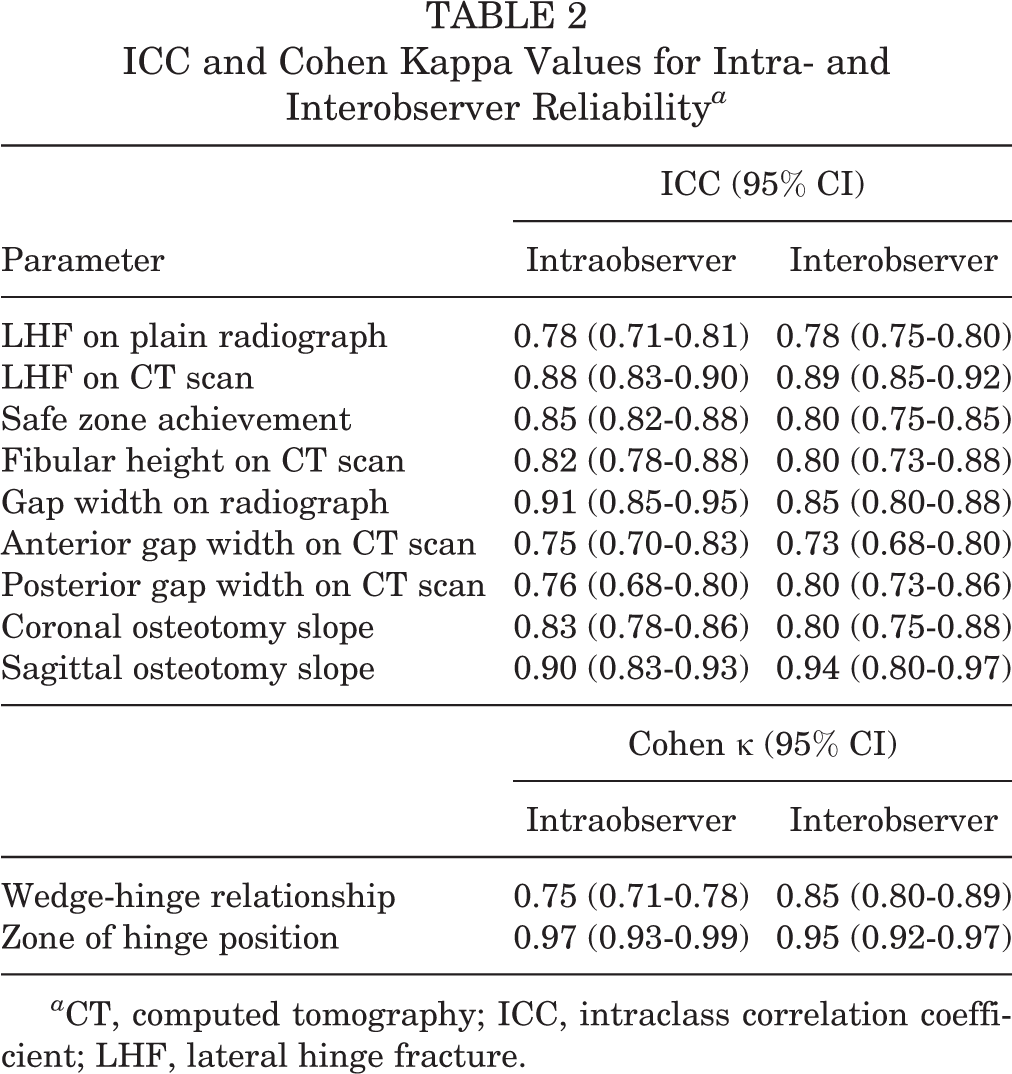
a CT, computed tomography; ICC, intraclass correlation coefficient; LHF, lateral hinge fracture.
A total of 17 LHF cases (20.5%) were detected on plain radiographs, while significantly more (37 cases; 44.6%) were found on CT scans (P = .001). According to the Takeuchi classification, 38 there were 28 cases (75.7%) of type 1 LHF, 7 cases (18.9%) of type 2, and 2 cases (5.4%) of type 3. A significant difference was found in gap width on plain radiographs and anterior and posterior gap widths on CT scans between the knees without LHF and with LHF. The mean difference in opening gap width between the 2 groups was 2.55 mm. In univariate regression analysis, 4 factors were shown to be statistically significant: age, gap width on plain radiographs, and anterior and posterior gap widths on CT scans. Logistic regression analysis revealed that opening gap width (odds ratio, 1.615; P = .001) and posterior opening gap width on CT scans (odds ratio, 3.731; P = .008) were predictive factors of LHF occurrence. Other patient and radiographic factors, including hinge position, were not related to LHF occurrence (Table 3). There was no significant relationship between the insufficiency of the osteotomy and the occurrence of LHF (P = .601). Post hoc power analysis showed a power of 99.8% to detect a significant difference between the 2 groups (with LHF vs without LHF), assuming an alpha error level of 5% and a change in opening gap width after surgery as the primary dependent variable.
Factors Affecting Lateral Hinge Fracture in Univariate and Multivariate Logistic Regression Analyses a
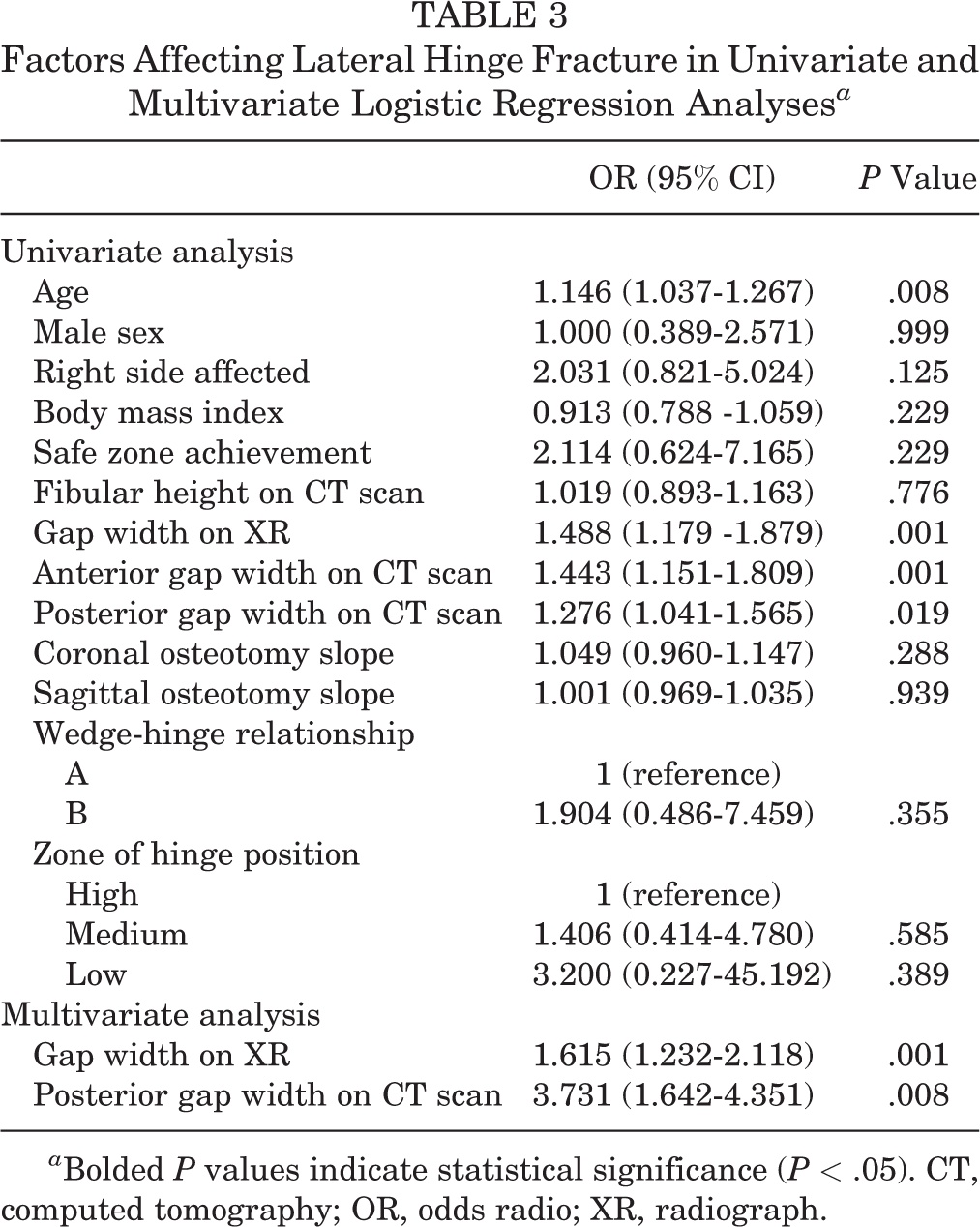
a Bolded P values indicate statistical significance (P < .05). CT, computed tomography; OR, odds radio; XR, radiograph.
A receiver operating characteristic (ROC) analysis was carried out to determine the possible cutoff value for opening gap width and LHF. The ROC analysis identified the opening gap width cutoff value for LHF to be 11.0 mm (area under the curve, 0.81; sensitivity, 78.4%; specificity, 73.9%).
Three patients presented with suspicious superficial wound infection. Two of them (1 with LHF and the other without LHF) were treated via oral antibiotics administration. One patient underwent wound debridement with intravenous antibiotics treatment and the infection was alleviated without any problem. One patient required conversion to total knee arthroplasty 23 months after MOWHTO because of undercorrection and worsening symptoms. However, there was no patient with LHF displacement, delayed union, or nonunion.
Discussion
The main findings of the present study were that (1) the detection rate of LHF on CT scans (44.6%) was higher compared with the detection rate on simple radiographs (20.5%); (2) opening gap width on plain radiographs and posterior opening gap width on CT scans were significantly larger in the LHF group than the no LHF group; and (3) the opening gap width cutoff value for LHF was 11.0 mm, with 78.4% sensitivity and 73.9% specificity. These results supported our primary and secondary hypotheses that CT scans would show a higher LHF detection rate than would plain radiographs and opening gap width would be related to the occurrence of LHF, but the relationship between hinge position and LHF was rejected.
Several studies have reported that the detection rate on CT scans is higher than that on plain radiographs. The detection rate on plain radiographs is 29.2% to 66.7% of the rate on CT scans. 6,17,19,20,22 This low accuracy is attributable to the low quality and direction of radiographs. Lee et al 17 revealed that most cases of LHF occur intraoperatively but about 50% are detected on fluoroscopy or immediate postoperative plain radiographs. Our study showed a 45.9% detection rate on plain radiographs compared with CT scans (20.5% on plain radiographs, 44.6% on CT scans). Only 3 of 7 (42.8%) type 2 cases were detected on plain radiographs. Considering that rehabilitation protocols may change depending on the detection of LHF, these results support the utility of postoperative CT scans.
Various clinical and radiological factors have been previously studied to identify the factors that contribute to LHF (Table 4). The medial opening gap width is one of the most commonly reported risk factors of LHF. 6,15,19,20,26,33 In the present study, opening gap width on a plain radiographs and posterior gap width on CT scans also showed significant differences between the 2 groups in logistic regression analysis. There were 2 prior studies on the association between gap width and LHF. Nakamura et al 26 suggested that the mean wedge opening distance in patients with LHF is significantly larger than that in patients without LHF (11.9 and 10.6 mm, respectively). The other, by Lee et al, 20 also showed a significant difference between the 2 groups (11.7 and 9.5 mm, respectively). The latter authors suggested that attention should be paid to opening gap widths ≥12 mm to prevent LHF. Our study also showed a significant difference in mean opening gap width between the LHF and the no LHF groups (12.56 and 10.01 mm, respectively). Furthermore, ROC analysis in the current study indicated that the most appropriate cutoff value for LHF was 11.0 mm, with 78.4% sensitivity and 73.9% specificity. Although we could not identify an exact cutoff value that had a combination of high sensitivity and specificity, care should be taken when correcting an opening gap width >11.0 mm.
Comparison With Previously Suggested Factors Affecting the Occurrence of LHF a
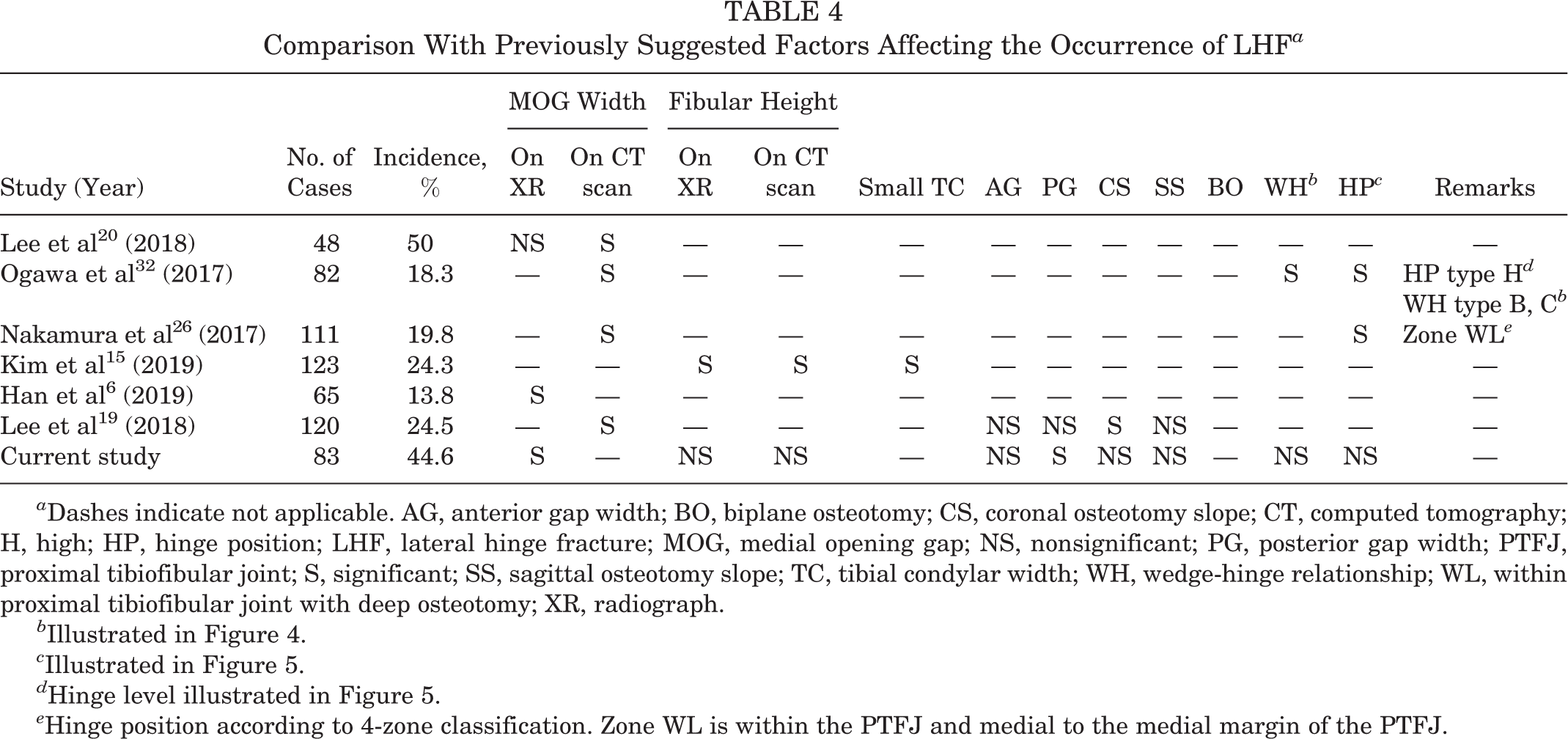
a Dashes indicate not applicable. AG, anterior gap width; BO, biplane osteotomy; CS, coronal osteotomy slope; CT, computed tomography; H, high; HP, hinge position; LHF, lateral hinge fracture; MOG, medial opening gap; NS, nonsignificant; PG, posterior gap width; PTFJ, proximal tibiofibular joint; S, significant; SS, sagittal osteotomy slope; TC, tibial condylar width; WH, wedge-hinge relationship; WL, within proximal tibiofibular joint with deep osteotomy; XR, radiograph.
b Illustrated in Figure 4.
c Illustrated in Figure 5.
d Hinge level illustrated in Figure 5.
e Hinge position according to 4-zone classification. Zone WL is within the PTFJ and medial to the medial margin of the PTFJ.
With an appropriate hinge position in a safe zone within the PTFJ, deep osteotomy has been confirmed to reduce strain and risk of fractures. 26,32,38 A previous study reported that osteotomy with a hinge position within the PTFJ decreases the occurrence of LHF and having a hinge position higher than the PTFJ is significantly related to the incidence of LHF. 32 Anatomically, the safe zone within the PTFJ has an increased bone mineral density compared with the area above the level of the PTFJ. 21 It has been suggested that many soft tissue insertions, such as insertion of the fibular collateral ligament, popliteofibular ligament, and biceps femoris tendon, provide stability. 21 However, our study results showed no significant difference in safe zone achievement and hinge position related to the occurrence of LHF between the 2 groups.
Insufficient osteotomy oblique to the anteroposterior axis is related to a higher incidence of LHF. 25,32,38 Ogawa et al 32 reported that LHF was induced even with a low opening gap width because of residual cortical bone in an insufficient osteotomy. This result was caused by anatomic features of cortical bone, which are weaker in bending forces than is cancellous bone. Our study did not show a significant difference between the 2 groups. However, all 4 type D cases, in which the anterior and posterior osteotomies do not extend to the lateral zone, developed LHF. Although this is not a statistically significant result, it supports the notion that insufficient osteotomy is more likely to cause LHF.
When Takeuchi type 2 or 3 fractures are detected during surgery, we address them by adding 1 or 2 cannulated screw to the lateral tibial condyle and delaying full weightbearing until 12 weeks postoperatively. For intraoperatively detected type 1 fracture, a K-wire to intersect the cutting plane close to the lateral hinge is temporarily inserted during medial plate fixation. Routine rehabilitation protocol is applied for type 1 cases. When LHF is detected from the postoperative CT scan, delayed weightbearing is recommended for type 2 or 3 without any additional fixation. Probably, most type 2 or 3 fractures only detected from CT scans are non- or minimally displaced fractures, and conservative rehabilitation may be sufficient for managing those cases. 14 Previous studies have reported that protective wire or screw insertions may reduce the occurrence of hinge fractures and further displacement. 2,5,10 Based on these results, we suppose that a protective K-wire fixation may help prevent the LHF when a large correction (>11 mm of gap width) is planned.
There were some limitations to the present study. First, this was a retrospective study, and sample size calculations could not be performed in advance. However, a post hoc power analysis was carried out, which showed a power of 99.8%. Second, general and focal bone mineral density in each patient was not considered. We included patients aged <65 years, but patients with low bone mineral density are more likely to have fractures. Third, the cutoff value was defined as the width of the gap, but in practice, this value could be different for each person depending on the size of the tibia. 18 We usually perform surgery on the assumption that the correction angle measured via preoperative planning is 1 mm wedge height per degree. However, depending on the tibial width of each individual, the gap width can increase proportionally. Since the mean difference in opening gap width between the 2 groups was only 2.55 mm, a precise method of calculating the cutoff value is needed.
Conclusion
The incidence of LHF was 44.6% on CT measurements; this incidence may be underestimated when determined on plain radiographs only. Large opening gap width, especially posterior gap width, may cause LHF. Therefore, special caution and preparations for possible LHF occurrence may be needed if a large correction is planned.
Footnotes
Final revision submitted April 5, 2021; accepted May 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.C. received support from the National Research Foundation of Korea grant funded by the Korean government (No. 2020R1F1A1050436). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from CHA Bundang Medical Center (study No. 2020-07-012).