
Abstract
Background:
Medial opening-wedge high tibial osteotomy (OWHTO) is a useful treatment option in patients with medial compartment osteoarthritis. Typically, the osteotomy site is filled with material such as autologous bone graft, allograft, or synthetic bone substitute. However, all these options have disadvantages.
Purpose/Hypothesis:
The purpose of this study was to describe tibial cortical autograft as an alternative to conventional graft options. It was hypothesized that the tibial rectangular cortical bone that is removed from the proximal medial cortical surface of the distal tibial fragment longitudinally could be a reliable option for recovery of the gap in the osteotomy area.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 520 patients with medial compartment osteoarthritis who underwent OWHTO between June 2009 and March 2019 were retrospectively analyzed. Patients were divided into 3 groups according to the graft material used to fill the osteotomy site: allograft in group A, iliac crest autograft in group B, and tibial autograft in group C. Bone union, evaluated by radiographs performed at 2 weeks, 4 weeks, 2 months, 3 months, 6 months, and 1 year postoperatively, was defined as occurring when at least 50% of the gap site was bridged with callus. Clinical assessment was performed using the International Knee Documentation Committee (IKDC) and Lysholm scores.
Results:
Included were 122 patients: 40 patients in group A, 42 patients in group B, and 40 patients in group C. The mean correction was 13.87°± 3.58° in group A, 12.33°± 3.92° in group B, and 14.10°± 2.99° in group C. The mean time for radiological bone union was 6.95 ± 1.40 months in group A, 4.48 ± 1.02 months in group B, and 5.07 ± 1.70 months in group C. Patients in all groups had similar IKDC and Lysholm scores at the final follow-up.
Conclusion:
This is the first report of this specific procedure in the literature. All clinical and radiological findings showed that use of tibial cortical autograft was an efficient method in patients undergoing OWHTO.
Medial opening-wedge high tibial osteotomy (OWHTO) is an effective surgical procedure for patients with osteoarthritis of the knee with varus deformities. Although it can be performed with either an opening- or closing-wedge technique, OWHTO is being employed with increasing frequency because it allows easier and more accurate deformity correction. Typically, the osteotomy site is filled with some kind of material such as autologous bone graft, allograft, or synthetic bone substitutes. However, all these options have disadvantages.4,7,11 Autogenous bone grafts harvested from the iliac crest have been considered as the standard graft material, but prolonged operating time and severe donor site pain are the primary disadvantages. 2 To overcome these disadvantages, a variety of solutions have been suggested, including allogenic bone graft, leaving the osteotomy opening unfilled, and using synthetic materials such as tricalcium phosphate, bicalcium phosphate granules, acrylic cement, and hydroxyapatite, but there is no ideal graft material identified for OWHTO.3,4,7,8
In this study, our aim was to describe the tibial cortical autograft technique as an alternative to conventional graft options. We hypothesized that the tibial rectangular cortical bone that is removed from the proximal medial cortical surface of the distal tibial fragment longitudinally could be a reliable option for recovery of the gap in the osteotomy area.
Methods
Approval for this study was granted by the local ethics committee. All participants provided informed consent before the surgery. A total of 520 consecutive patients with varus knee with medial unicompartmental osteoarthritis who had undergone OWHTO between June 2009 and March 2019 were retrospectively analyzed. All osteotomies and clinical and radiological evaluations were performed by a single surgeon (C.C.K.). The indication for surgery was medial compartment osteoarthritis of the knee with varus malalignment of the limb. No patient had a history of a disease or severe trauma involving the knee. Study exclusion criteria were patients with <1 year of follow-up, those whose osteotomy gap site was left empty without using any type of grafts (typical gap size, <15 mm), those with plates other than TomoFix at the osteotomy site (Puddu plate was widely used, especially at the first half of the retrospective evaluation period), and those whose radiographs and other clinical documents could not be obtained were excluded.
Patients who met the study criteria were divided into 3 groups according to the graft material used to fill the osteotomy site: allograft in group A, iliac crest autograft in group B, and tibial autograft in group C.
Preoperative Planning and Surgical Technique
We used full-length standing anteroposterior radiographs of the lower extremity for the preoperative planning. The level of varus was measured as the femorotibial angle, and an opening-wedge osteotomy was planned to achieve an ultimate alignment of 10° of valgus femorotibial angulation.
The operation was performed with the patient under general or spinal anesthesia. Thromboembolic prophylaxis (0.4 mL Clexane; Sanofi) and intravenous antibiotic (1 g Sefazol; Mustafa Nevzat) were used. The patient was placed on a radiolucent table. A fluoroscope was installed to visualize the knee joint in 2 planes. During the operation, patients were in a supine position in which the leg was draped free, from the iliac crest to the foot, so it was possible to check alignment intraoperatively. A tourniquet was applied on the thigh. A knee arthroscopy was first performed on each patient, to ensure an intact lateral joint compartment and to treat additional intra-articular lesions. We used an 8 to 10 cm–long medial longitudinal skin incision 3 cm distal to the joint line. The periosteum was elevated medially and L-shaped. Proximal to the pes anserinus, the medial collateral ligament was dissected from the posteromedial cortex of the tibia, and a blunt Hohmann retractor was inserted to protect the neurovascular structures.
Under fluoroscopic control, the direction of the joint line was marked parallel with a K-wire and the direction of the osteotomy in the frontal plane was marked with another K-wire (Figure 1).

The direction of the joint line was marked parallel with a 2.0-mm K-wire (top wire). The direction of the osteotomy in the frontal plane was marked with a 2.5-mm K-wire (bottom wire).
The osteotomy was started at the upper margin of the pes anserine and ended 1 cm from the lateral cortical margin, at the level of the tip of the fibula and 15 mm away from the proximal articular surface of the tibia. The osteotomy site was opened slowly and superiorly, with the proximal fragment elevated in both the front and the back and with great care taken not to break through the lateral side. About 30 mL of allograft was used to fill the gap in group A, iliac crest spongious autograft was used in group B, and tibial cortical autograft was used in group C.
For patients in group C, a rectangular tibial cortical autograft of 10 to 12 mm width and 20 to 25 mm length was taken out from 2 to 2.5 cm below the osteotomy line with the help of an Anspach microsagittal saw (DePuy Synthes) (Figure 2A). This graft was placed at the anteromedial site of the gap with the long axis of the graft parallel to the osteotomy line. The spongious (inner part) part of the graft was placed toward the gap, and the cortical site was placed between the cortical edges of the osteotomy line at the lateral site. A TomoFix plate and screws (DePuy Synthes) were used to fix the osteotomy site. Finally, rigid fixation was provided and the harvested site was left under the plate (Figure 2B).

(A) A rectangular tibial cortical autograft of 10 to 12 mm width and 20 to 25 mm length was taken from 2 to 2.5 cm below the osteotomy line. (B) Postoperative anteroposterior knee radiograph obtained in a patient in group C. The cortical autograft in the gap and the harvested area are shown with arrows.
Postoperative Rehabilitation and Evaluation
Early postoperative anteroposterior and lateral knee radiographs were taken. On the first day after surgery, isometric quadriceps, active ankle, and knee range of motion exercises were started. Flexion and extension of the knee joint were exercised both actively and passively. No braces or casts were used. Partial weightbearing was started the day after surgery. Full weightbearing was started approximately 8 weeks after surgery, depending on radiological evaluation. Postoperative alignments were measured after the eighth week on long-leg radiographs after full weightbearing.
As a routine of our clinic, follow-up visits were scheduled and follow-up radiographs were performed at 2 weeks, 4 weeks, 2 months, 3 months, 6 months, 1 year, and then annually. A modified version of the osteotomy filling index of Brosset et al 4 was used to assess the bone union at the osteotomy site, in which the site was divided into 4 zones from medial to lateral on anteroposterior radiographs, and bone union was defined when at least 50% of the gap site was bridged with callus (Figure 3). If the bridging callus was not seen in at least 50% of the gap site at 6 months, it was defined as delayed union. Preoperative and postoperative clinical evaluation of patients was performed using the International Knee Documentation Committee (IKDC) and Lysholm scores. All the measurements and assessment for union were made by an experienced orthopaedic surgeon (C.C.K.).
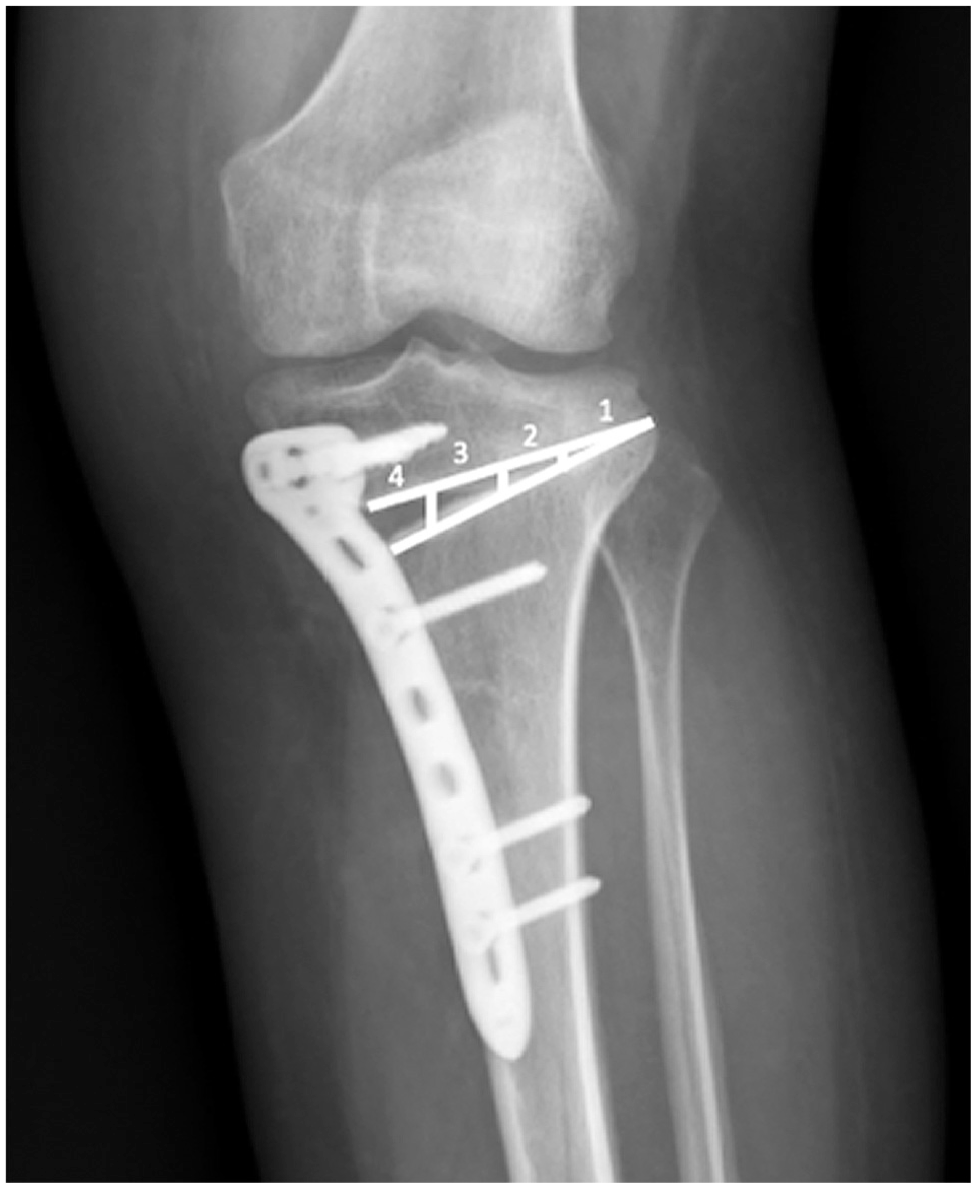
Osteotomy filling index. Bone union was defined when the callus reached zone 3 (at least 50% of the gap site).
Statistical Analysis
All statistical analyses were performed using IBM SPSS for Windows Version 20.0 (IBM Corp). Kolmogorov-Smirnov tests were used to test the normality of data distribution. Continuous variables were reported as means with standard deviations. Patient data were analyzed using the chi-square test and analysis of variance. The intergroup rate of union, clinical scores, and complications were analyzed using the Kruskal-Wallis test, and a P value of <.05 was considered statistically significant.
Results
A total of 122 patients met the study criteria: 40 patients in group A (allograft), 42 patients in group B (iliac crest spongious autograft), and 40 patients in group C (tibial cortical autograft). The patient and surgical data of all 3 groups are shown in Table 1. The mean time until at least 50% of the gap site was bridged with callus was significantly different among the groups: 6.95 ± 1.40 months in group A, 4.48 ± 1.02 months in group B, and 5.07 ± 1.70 months in group C (P = .001) (Table 1).
Patient and Surgical Characteristics Among the Study Groups a

Graft material: allograft in group A, iliac crest spongious autograft in group B, and tibial cortical autograft in group C. Data are reported as mean ± SD unless otherwise indicated. Boldface P value indicates a statistically significant difference among the groups (P < .05). FTA, femorotibial angle.
Compared with preoperative values, the postoperative IKDC and Lysholm scores revealed significant enhancements in all groups (P < .05 for all), with no significant differences in scores among the groups at the last follow-up (P > .05) (Table 2).
Clinical Outcomes Among the Study Groups a

Data are reported as mean ± SD. IKDC, International Knee Documentation Committee.
There was a statistically significant difference between group A and other groups (P < .005) in radiograph the day after surgery. In the early postoperative radiograph, the femorotibial axis was at a mean of 7.88°± 2.81° valgus in group A, 6.98°± 2.60° in group B, and 7.08°± 2.49° in group C. The mean correction was 13.87°± 3.58° in group A, 12.33°± 3.92° in group B, and 14.10°± 2.99° in group C. Delayed union was seen in 19 patients in group A, 1 patient in group B, and 4 patients in group C (P < .001). Other complications are shown in Table 3.
Postoperative Complications Among the Study Groups a

Data are reported as No. of patients. Dash indicates that complications did not occur. Boldface P value indicates a statistically significant difference among the groups (P < .05).
Discussion
In the current study, we showed that tibial cortical autograft for gap filling in OWHTO had a faster union rate than allograft. Furthermore, it had a similar union rate with iliac crest autograft (P > .05), without donor site morbidity risk. Although fracture at the graft harvest site was a potential complication, overlaying the plate on the place where the graft was taken appears to have provided sufficient support.
A bone graft from the iliac crest has been widely recognized as the gold standard among bone graft options for OWHTO. This type of bone graft is osteogenic, osteoinductive, and osteoconductive and confers no risk of immunogenicity or infection transmission. 13 However, possible donor site comorbidities of autologous iliac crest bone harvesting include chronic pain, infections, and sensory changes. 12 There are also other complications, such as gluteal artery injury, deep wound infection, sciatic nerve injury, and iliac bone linear fracture, which have been reported to be associated with this process.1,5,6,15,17 The autogenic graft we used, obtained from the distal tibial fragment, is also osteoconductive and osteoinductive and has an osteogenic effect and the advantage of not producing donor site morbidity because it was taken from the same surgical site. 13
Because of extra surgical time for graft harvesting, donor site pain, and the risk of inflammation, allogenous bone grafts have been suggested as an alternative to the iliac crest graft in many studies.6,9,14-16 However, allogenic grafts are just osteoconductive and are not osteoinductive or osteogenic. 13 Their advantages over autogenous bone grafts include no donor site–related complications and a theoretically unlimited supply, whereas the disadvantages are slow remodeling, the risk of disease transmission, high cost, and immunologic reactions. 8 Synthetic grafts have been used as an alternative to autografts and allografts in OWHTO. For this purpose, there are usually graft substitutes, such as tricalcium phosphate, bicalcium phosphate granules, acrylic bone cement, and hydroxyapatite. However, there are also several disadvantages of this technique, such as delayed incorporation into bone, infections, and soft tissue irritation. 16
Jung et al 10 used another autograft to fill the gap rather than iliac crest. They obtained the autograft from the ipsilateral femoral condyle by using Osteochondral Autograft Transfer System donor cutting tubes to extract bone from the medial femoral condyle and compared the union rate with those of 2 other groups. Tricalcium phosphate was used as a graft to fill the gap in one group, and the gap in the other group was left unfilled. As a result, patients with autograft had a faster union rate and improved clinical knee scores. However, because of the limited supply of the autograft from the medial femoral condyle, they used a mixture with tricalcium phosphate. Therefore, it has the potential disadvantages of synthetic grafts, such as infection and soft tissue irritation. Furthermore, donor site morbidity could also be seen as with an iliac crest autograft.
Limitations
The current study has limitations. The most important one is that we were only able to include <25% of the patients who underwent OWHTO surgery because others did not meet the criteria. A second limitation is that the measurements and assessment of union on radiographs were made by a single orthopaedic surgeon. Finally, the retrospective study design is a limitation of this study.
Conclusion
In the current study, the rectangular cortical autograft we obtained from the same surgical site as the OWHTO procedure had the advantages of the gold-standard iliac crest autograft method while avoiding the disadvantages associated with obtaining graft material from a different surgical site. It also avoids other potential disadvantages such as low union rate and infection transmission risk. The only disadvantage of the tibial cortical autograft might be an increased fracture risk at the donor site. However, we have not encountered any fractures.
Footnotes
Final revision submitted August 16, 2023; accepted August 30, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kocaeli Universitesi (reference No. E-80418770-020-178961).