
Abstract
Background:
Although the incidence of osteochondritis dissecans (OCD) of the knee may be low, an overview and comparison of sports-related outcomes with current surgical management techniques are needed.
Purpose:
To summarize the available evidence regarding outcomes for different surgical treatment options for unstable OCD of the knee in both skeletally mature and immature patients by calculating the return to sports (RTS) rate, the mean RTS time, and other sports-related postoperative outcome measures.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review of studies on RTS after surgical correction of unstable OCD within the knee was conducted utilizing PubMed, Embase, and the Cochrane databases. Included were studies discussing the treatment of unstable OCD with minimum 1-year follow-up outcomes. Multivariate analysis was used to compare studies grouped together based on RTS and skeletal maturity.
Results:
Of 2229 articles, 6 studies (197 patients; 198 knees) met the inclusion criteria and were included in our analysis. The percentage of patients who returned to the previous level of sport ranged from 52% to 100%; those returning to any level of sport ranged from 87% to 100%. Clinical outcomes did not differ between patients with open versus closed physes. Osteochondral Autograft Transfer System (OATS) procedures had a 100% RTS rate across several studies with skeletally mature and mixed cohorts, and microfracture had the lowest overall RTS rate (52%). For skeletally immature patients, all examined studies that utilized either open or arthroscopic reduction and internal fixation, 77% and 78%, respectively, had acceptable RTS rates. Arthroscopic fixation had a higher rate of revision surgery in both skeletally mature and immature patients.
Conclusion:
Our analysis indicated that the treatment of unstable OCD lesions using the OATS technique demonstrated high RTS rates across several studies, while microfracture alone exhibited the lowest RTS rate. Both arthroscopic and open internal fixation utilizing bioabsorbable screws yielded satisfactory RTS rates for juvenile patients with OCD.
Although the epidemiology of osteochondritis dissecans (OCD) has been established, its etiology remains elusive. The Research in OsteoChondritis of the Knee (ROCK) group defines OCD as a focal, idiopathic alteration of subchondral bone with a risk for instability and disruption of adjacent articular cartilage that may result in premature osteoarthritis. 17 Several theoretical etiologies have been proposed, including repetitive microtrauma, inheritance, inflammatory causation, and vascular abnormalities.2,9,11-14,25,29,30,41 Given that this pathology has increased frequency in those engaging in sporting activities, there is a strong case for repetitive microtrauma as the leading hypothesis. 7
The symptoms of OCD within the knee vary according to the stage of pathology and its site. In juvenile OCD, when lesions are considered stable, symptoms may be absent or vaguely described, are often longstanding, worsen with activity, and may occasionally lead to an antalgic gait. 8 Surgical intervention is generally indicated when there is evidence of an unstable lesion with a visible loose body or if conservative measures have failed. Several classification systems exist for the arthroscopic evaluation of OCD lesions. However, the most widely known is the arthroscopic classification, according to Andriolo et al. 4 This classification uses a simple grading system to discern stable from unstable: grade 1, intact cartilage and subchondral bone; grade 2, initial signs of fragment separation but fragment in situ, nonmobile; grade 3, partially detached mobile fragment in situ (flap lesion); and grade 4, craters with loose bodies (salvageable or unsalvageable).
Many surgical techniques have been developed to treat unstable OCD lesions of the knee, including fixation with metallic or bioabsorbable implants, as well as biologic repair with autograft or allograft osteochondral plugs, and chondrocyte transplantation. Several studies have shown better results when using procedures to reconstruct the bone and cartilage.5,22,23,27,36 Deciding on the best operative treatment depends mainly on lesion stability, grade, chronicity, and age. 24 The most common technique for juvenile OCD with unstable lesions or loose bodies is fixation, with previous studies 6 reporting success rates ranging from 91.7% to 100%. The best approach for surgical treatment of skeletally mature populations is less clear, and several studies have reported significantly worse clinical and radiographic outcomes when compared with skeletally immature patients.1,32 While patient-reported outcomes for OCD have been previously described in those engaging in sporting activities, return to sports (RTS) has not been thoroughly evaluated.
RTS can significantly influence the quality of life of those who engage in athletics. Since OCD of the knee is associated with participation in athletics, there is a need for an overview and comparison of sports-related outcomes with the current surgical management techniques. 10 This review aimed to summarize the available evidence regarding sports outcomes for different surgical treatment options in skeletally mature and immature populations by calculating the RTS rate, the mean RTS time, and data on other sports-related outcomes after the treatment of unstable OCD of the knee. We hypothesized that there would be no difference between surgical treatment options for unstable OCD of the knee with respect to sports outcomes.
Methods
A systematic literature review was conducted utilizing PubMed, Embase, and the Cochrane database. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) guidelines were followed. 34 The search was conducted using the following terms, which were combined by the Boolean operators AND/OR: “osteochondritis dissecans,”“OCD,”“osteochondral,” articular cartilage,”“repair,”“surgery,”“treatment,”“osteochondral allograft,” autologous chondrocyte implantation,”“fixation,”“unstable,”“knee,”“clinical studies,” and “return to sport.” All studies pertaining to the treatment of unstable OCDs within the knee were reviewed between April 1996 and March 31, 2022. All articles discussing the treatment of unstable osteochondral defects with reported outcomes with a minimum 1-year follow-up were included.
The exclusion criteria were published abstracts, narrative reviews, articles not written in English, commentaries, study protocols, cadaveric studies, sample size <10, nonevaluation of RTS, nonisolated unstable OCD, nonspecified surgical technique, or a minimum follow-up of <1 year. The literature search results were independently reviewed by 2 authors (R.G., G.C.), and any disagreements regarding eligibility were resolved by consensus between the reviewers.
The full texts from all included studies were reviewed. These articles were categorized based on the surgical technique and the skeletal maturity of the study population. Studies were stratified based on the population they examined as follows: skeletally mature, skeletally immature, and mixed cohorts. Because of the heterogeneity of reported outcomes, the mean results were not pooled but instead reported as a range of means.
Quality Assessment
The methodological quality of nonrandomized studies was evaluated using the MINORS (Methodological Index for Non-Randomized Studies) criteria. Each study was graded on methodological quality by 2 independent reviewers (R.G., G.C.), with any conflicting outcomes resolved by discussion. In case of persisting conflict, the senior author (M.E.B.) was consulted, whose opinion was decisive. The revised Cochrane risk of bias tool was used for assessing randomized control trials. 39
Data Extraction
A standardized form was used to retrieve data on study characteristics. Acquired data on patient characteristics included study properties (authors, publication year, level of evidence, and the number of patients), patient characteristics (age, sex, surgical history, and sport played), lesion characteristics (location, size, method to determine instability, and physeal status), surgical details, outcomes (patient-reported outcome scores; functional, clinical, radiographic, and outcomes; and RTS), complications, failures, and reoperations. The described treatment techniques were examined per study, and they were divided into corresponding treatment groups. If other sports-related clinical outcomes were present, these were additionally extracted from the studies and recorded as well as subsequently analyzed where possible.
Data Analysis
For this study, 2 types of RTS were considered: (1) return to the previous level of sport, where patients had to perform in the same sport at the preinjury level and (2) return to any level of sport, whereby the patients could participate in any sport at any level, regardless of their performance before their injury. With regard to skeletal maturity, the terms “immature,”“juvenile” (open physeal plate), and “mature” (closed physeal plate) were accepted as indicative of physeal status.
Statistical Analysis
Results of the individual studies were extracted and synthesized for qualitative and quantitative analysis. Descriptive and central tendency statistics were outlined, and categorical values were compared using chi-square analysis or Fisher exact tests. Statistical significance was set at P < .05. All statistical analyses were performed with R studio software Version 3.6.3 (RStudio).
Results
The database search identified 2229 records. After title and abstract screening, the full texts of 82 articles were reviewed, and the reference lists were checked to avoid missing other articles. Six studies21,28,31,33,43,45 met the inclusion criteria and were included in our final analysis (Figure 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) flowchart of the study inclusion process. OCD, osteochondritis dissecans; RTS, return to sports.
Table 1 summarizes the characteristics of the included studies. Outcome data were available on 197 patients, with ages ranging from 15 to 25 years old. Overall, 139 men and 29 women were evaluated within the included studies—not all studies provided information regarding patient sex. Sample sizes varied, with the average study including 32 patients (range, 17-57 patients). Studies generally were of level 4 evidence, retrospective, and performed as a single-institution case series. Four retrospective case28,31,33,43 series, 1 prospective case series, 45 and 1 randomized controlled trial were included. 21 Overall, 2 studies28,43 were conducted on isolated juvenile OCDs, 3 studies33,43,45 on isolated skeletally mature patients, and 2 studies21,31 on both skeletally mature and immature patients. The mean follow-up length for studies consisted of midterm (2-8 years) in 4 studies28,31,33,43 and long term (≥8 years) in 2 studies.21,45
Characteristics of the Included Studies a

ARIF, arthroscopic reduction and internal fixation; HTO, high tibial osteotomy; LOE, level of evidence; LRL, lateral retinacular lengthening; MACT, matrix-assisted chondral transplantation; MF, microfracture; MINORS, Methodological Index for Non-Randomized Studies; NR, not reported; OATS, Osteochondral Autologous Transfer; ORIF, open reduction and internal fixation.
Reported as mean ± SD or mean (range).
The surgical technique was also heterogeneously distributed, with 2 studies28,43 examining fixation using bioabsorbable screws (n = 62 patients) and others performing an Osteochondral Autograft Transfer System (OATS) with high tibial osteotomy (n = 30 patients), 33 hybrid OATS with bioabsorbable nail fixation (n = 17 patients), 31 matrix-assisted chondral transplantation (MACT) (n = 31 patients), 45 microfracture (n = 29 patients), 21 or mosaicplasty (n = 28 patients). 21 Both studies28,43 that isolated skeletally immature patients performed open or arthroscopic reduction and internal fixation (n = 36 patients) (Table 1).
The mean defect size ranged from 2 to 3.8 cm2 across all included studies. Most of the studies (5 of 6) reported lesion location, with the medial femoral condyle being the most commonly affected (71.2%), followed by lateral femoral condyle (13.7%), trochlea (14.4%), and lastly, patella (0.7%) (Table 2).
Defect Size and Location a

Data are shown as mean ± SD or mean (range). LFC, lateral femoral condyle; MF, microfracture; MFC, medial femoral condyle; NR, not reported.
Quality Appraisal
Using the MINORS system to assess study quality, the mean quality score for the studies we identified was 15.3 (range, 9-19) (Table 1). Only 1 of the studies identified was performed as a randomized controlled trial. 21 To assess its quality, the revised Cochrane risk of bias tool was utilized. 40 Five domains were examined to address important mechanisms by which bias can be introduced into the results of a trial based on a combination of empirical evidence and theoretical considerations. The study was judged to be at an overall low risk of bias.
Return to Sports
The percentage of patients who returned to the previous level of sport ranged from 52% to 100%, and the percentage of those returning to any level of sport ranged between 87% and 100%. The time to return to the previous level of sport ranged between 6.5 months and 9.7 months for all studies. RTS timelines varied by surgical technique, rehabilitation protocol, and study design (Table 3).
RTS Outcomes a
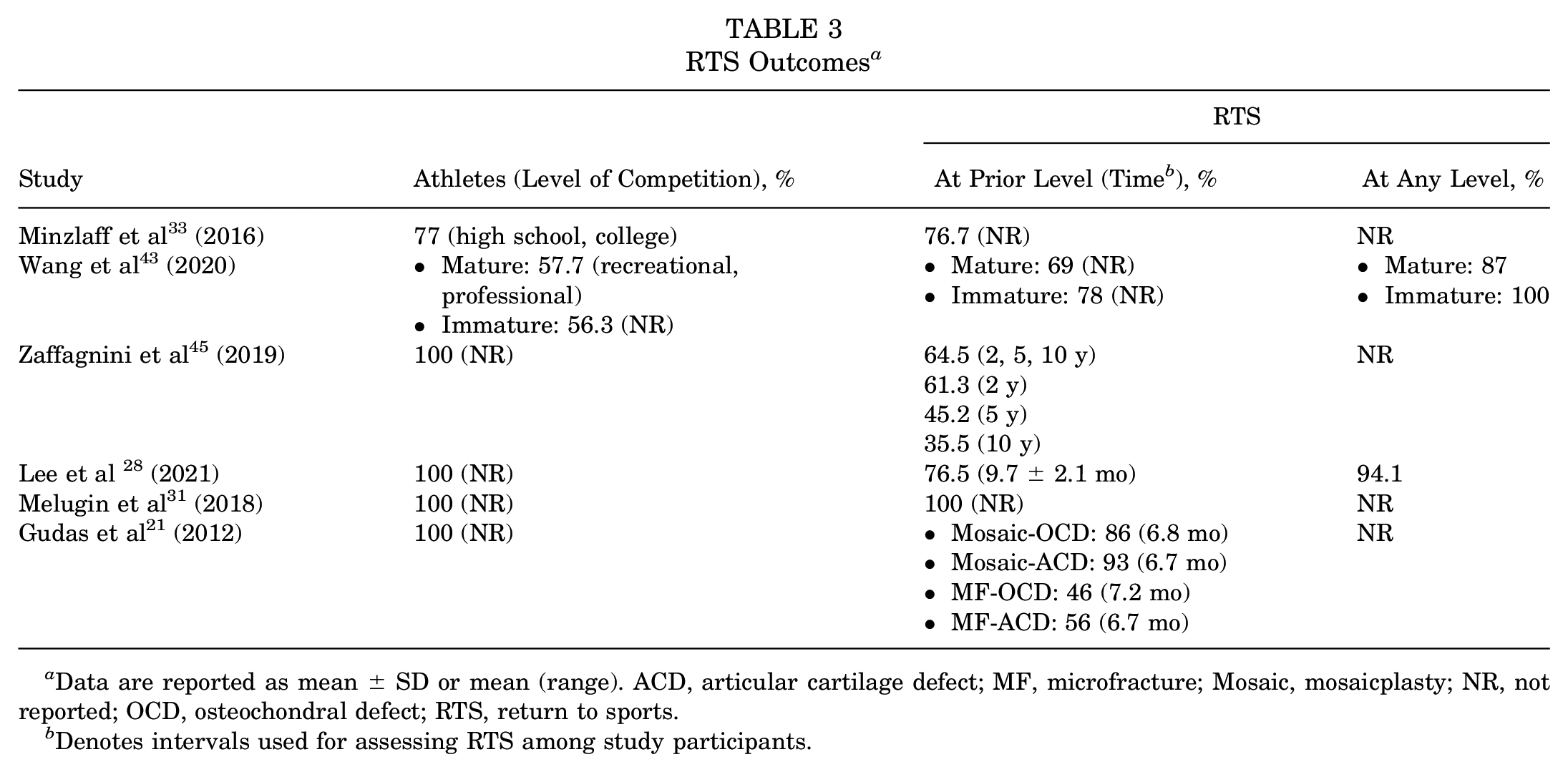
Data are reported as mean ± SD or mean (range). ACD, articular cartilage defect; MF, microfracture; Mosaic, mosaicplasty; NR, not reported; OCD, osteochondral defect; RTS, return to sports.
Denotes intervals used for assessing RTS among study participants.
Microfracture
Gudas et al 21 examined RTS after microfracture and compared outcomes with those after mosaic-type OATS (mosaicplasty). At the 10-year follow-up, 45% of patients (n = 13) who underwent microfracture were able to play at their previous level of sport, with a mean RTS time of 7.2 months in patients with OCD and 6.2 months in patients with articular cartilage defect.
Matrix-Assisted Chondral Transplantation
The study by Zaffagnini et al 45 evaluated RTS after MACT. The mean age in this group of 31 patients was 22.6 ± 6.3 years and consisted of all men. These patients had autologous bone grafts harvested from the ipsilateral tibia to fill the subchondral defect before continuing MACT. Return to the competitive level of sport was found to be 64.5%, with 58.1% returning to preinjury levels. Notably, multivariate analysis demonstrated that previous surgery was the single most influencing factor for returning to the same sport level (P = .010), with 84% of athletes who had no previous history of surgery able to RTS as opposed to 33% of athletes who had undergone previous surgery.
Osteochondral Autograft Transplantation
Two studies evaluated RTS data after OATS (47 patients, 48 knees), with Minzlaff et al 33 examining skeletally mature patients and Melugin et al 31 examining a mixed cohort. Melugin et al utilized a hybrid technique that involved fixation with nails, screws, or plugs of salvageable fragments and replacement of unsalvageable fragments using an OATS technique. Magnetic resonance imaging assessment at a mean of 7.8 months postoperatively demonstrated a mean MOCART score of 87.5. Overall, both studies showed successful RTS rates in a skeletally mature athletic population using an OATS technique; Melugin et al reported that 100% of their patients returned to their previous level of sport, and Minzlaff et al 33 reported an RTS rate of 76.7%.
Mosaicplasty
Gudas et al 21 found a significantly higher RTS rate and lower failure rates after mosaicplasty when compared with microfracture at a 10-year follow-up.
Fixation
We identified 3 studies28,31,43 that evaluated RTS data after fixation of knee OCD lesions. All studies used bioabsorbable nails or screws. Two studies28,43 that examined skeletally immature patients found a mean return to the previous level of sport ranging from 76.5% to 78%. The range for mean return to any level of sport was 94% to 100%. Only 1 of the examined studies reported time to return to the previous level of sport (9.7 ± 2.1 months). 28 Notably, Lee et al 28 examined a population of only trochlear lesions, wherein 94.1% were able to return to any level of sport. Melugin et al 31 utilized a hybrid procedure that used bioabsorbable nails to fix salvageable fragments and an OATS procedure for the unsalvageable portions. Although no RTS times were reported, 100% of the patients in this study could return to their previous level of sport.
Comparative Studies
The study by Gudas et al 21 directly compared mosaicplasty and microfracture techniques within their cohort of athletes, with a long-term follow-up of 10 years. The study had a mix of skeletally immature and mature patients. Return to a previous level of sport was found to be 86% in the mosaicplasty group and 46% in the microfracture group. The mean time to RTS differed between the mosaicplasty and microfracture groups, with patients able to RTS after a mean of 6.8 and 7.2 months, respectively. Revision rates also differed significantly between mosaicplasty and microfracture groups, with 14% and 38% needing a revision within the follow-up period, respectively.
Wang et al 43 directly compared outcomes in skeletally mature and immature patients by performing a subgroup analysis. In this study, it was found that 100% of skeletally immature and 78% of skeletally mature patients were able to return to the previous level of sport utilizing a reduction and internal bioabsorbable screw fixation. However, no statistically significant difference in either RTS overall or RTS at the same level was found between groups (P = .511 and P = .657, respectively). 43
Patient-Reported Outcomes
Patient-reported outcomes were heterogeneously reported and available for 5 studies21,28,31,33,45 (Table 4). Although there was no consistent use of outcome measures throughout the included studies, the most commonly used patient-reported outcome measures were the Tegner (4 studies28,31,33,45) and International Knee Documentation Committee Subjective Knee Form (IKDC) scores (3 studies28,31,45). The mean postoperative Tegner score ranged between 5 and 8.9. Three studies28,31,33 reported no significant change in the Tegner score after surgery, and 1 study 45 reported an increase in the mean Tegner score. The mean postoperative IKDC score ranged between 88.7 and 95.2, with all 3 studies28,31,45 reporting increased IKDC scores after surgery.
Outcome Measures and Study Summaries a

ACD, articular cartilage defect; EQVAS, EuroQol-visual analog scale; HTO, high tibial osteotomy; HSS, Hospital of Special Surgery; ICRS, International Cartilage Repair Society; IKDC, International Knee Documentation Committee Subjective Knee Form; KOOS, Knee injury and Osteoarthritis Outcome Score; LFC, lateral femoral condyle; MF, microfracture; MFC, medial femoral condyle; MOCART, Magnetic Resonance Observation of Cartilage Repair Tissue; MRI, magnetic resonance imaging; OATS, Osteochondral Autograft Transfer System; OCD, osteochondritis dissecans; postop, postoperative; preop, preoperative; RTS, return to sports.
Revision Rates and Complications
Complications reported in this review consisted of superficial infection, painful hardware due to screw back out, and intraoperative K-wire incarceration (Table 5). The rates of revision ranged33,43 from 0% to 40%. Overall, there was an observable difference in revision rates between arthroscopic (40%) and open fixation (5.9%) techniques in skeletally immature studies.28,43 Arthroscopic fixation had higher revision rates in both skeletally mature and immature cohorts when compared with alternate techniques on the same population. 31
Surgical Techniques and Complication Rates a

MACT, matrix-assisted chondral transplantation; MF, microfracture; OATS, osteochondral autologous transplantation; OCD, osteochondritis dissecans.
Discussion
The main findings of this study are 2-fold. First, microfracture alone led to lower rates of RTS (46%) compared with other surgical techniques (64.5% MACT, 76.7% OATS, 94% fixation). Second, RTS rates were good in skeletally immature patients undergoing resorbable screw fixation performed either arthroscopically or open (100%), although arthroscopic fixation had a higher rate of revision surgery (40% vs 5.9%).
There has yet to be a consensus on the gold standard treatment for patients with unstable OCD lesions. The goal of surgical correction of osteochondral defects is to promote healing by interrupting the sclerotic interface between fragment and healthy bone, thereby facilitating the reintegration of blood supply. This can be achieved by drilling, allogenic or autologous transfer of bone graft, and fixation techniques. Younger patients with open physes are typically treated conservatively for 3 to 6 months and re-evaluated for progression. Still, surgery may be a first-line treatment if the lesion is unstable or if there are loose bodies present. 3
Patient sex, age, lesion location, physeal status, and lesion size have all been implicated as prognostic factors of surgical success and complete healing of OCD lesions. 3 The studies within this review were predominantly men, which is supported by epidemiologic studies showing a higher incidence in men compared with women. 35 Moreover, several studies have demonstrated poor outcomes and lower rates of healing with larger OCD lesions.8,26,39,42 In the present review, most studies reported a mean lesion size of ?3 cm2. However, 1 study 43 reported a mean defect size of 3.83 cm2, with a return to a previous level of sport of 69%. Everhart et al 19 demonstrated a significantly greater risk for total knee arthroplasty in patients with full-thickness cartilage defects >2 cm2 compared with those with lesions <2 cm2. This alone has implications on RTS and must be taken into account when evaluating technique-based differences.
RTS has become a widely used measure of quality of life and clinical outcomes, particularly in the young athletic population. When evaluating RTS, it is crucial to understand any variables that may affect the rates at which athletes RTS, such as extrinsic pressures to discontinue sport because of age and level of sport or intrinsic concerns over reinjury, concomitant pathology, and other patient-related factors. 15 Furthermore, rehabilitation protocols play a critical role in RTS. This was demonstrated in a study by Della Villa et al, 13 where a standardized rehabilitation protocol after autologous chondrocyte implantation was compared with a specialized on-field rehabilitation protocol, and it was found that those in the specialized group had significantly earlier RTS compared with the standard (mean, 10.6 and 12.4 months, respectively). This was further elucidated by Ebert et al, 16 who demonstrated that an accelerated rehabilitation (8-week) protocol reduced pain and symptoms and had a faster return to normal function 2 years after MACT compared with a conservative protocol (12 weeks). In the present review, the method of evaluating RTS varied between studies, making it difficult to identify a timeline for RTS conclusively.
There are many factors that surgeons need to consider when choosing a surgical approach that may offer a better outcome for their patients. Despite this, the current literature does not reveal much in terms of an optimal surgical technique. A 2020 systematic review of biologic techniques for the repair of cartilage injury showed that rates of return to preinjury levels of sport were highest after MACT (69.3%), followed by OATS (62.3%), osteochondral allograft (57.1%), and microfracture (55.1%), while return to any level of sporting participation for MACT and OATS was 74% and 84%, respectively. 37 Although the aforementioned review did not isolate unstable OCD lesions, the findings of this study are in agreement with previous studies, demonstrating MACT to be an acceptable option for patients with defects not amenable to fixation with good clinical outcomes. 45 Moreover, the OATS technique demonstrated the highest RTS rate and previous level of sport in the current review, thereby supporting its efficacy as a surgical option for patients with OCD. Conversely, microfracture demonstrated the lowest RTS rate (52%) and higher revision rate in 10 years (38%). The belief behind the microfracture technique is that the holes made provide spacing for the marrow to hold and adhere as durable cartilage while the subchondral plate is preserved.20,38 This, in turn, provides an environment where tissue regeneration can occur with the bodies endogenous healing capabilities. 18 When used alone, microfracture shows inferior outcomes compared with other cartilage repair procedures. This is similar to the results in our study, where we noted good RTS with OATS and MACT, while microfracture alone led to lower rates of RTS.
Considerations for skeletally immature populations are considerably more nuanced, given their potential for recovery. Previous studies have shown no statistical difference in survivorship between skeletally mature and immature patients after screw fixation. 44 When examining fixation techniques in skeletally immature patients, both open and arthroscopic techniques led to satisfactory RTS rates; however, the arthroscopic procedures were found to have a higher rate of revision surgeries when compared with open fixation procedures.28,43 One consideration for the higher revision rates seen here may be the mean lesion size of the cohort. However, of the skeletally immature studies examined in this review, only Wang et al 43 reported the mean defect size, further emphasizing the need for future high-quality studies in skeletally immature populations. As a whole, limited RTS data are available on the skeletally immature population with unstable OCD in the sports medicine literature, leaving much to be understood about the overall impact of various surgical techniques on sports-related outcomes.
The comparative studies within our review showed 3 major considerations for surgical intervention. Most notably, for the consideration of skeletally immature populations, Wang et al 43 demonstrated that arthroscopic reduction and internal fixation had acceptable outcomes in both skeletally mature and immature patients with no significant differences in RTS. Second, 1 of the significant factors associated with fixation failure was undergoing a previous surgical procedure to address the OCD lesion. In addition, not considering physeal status, a subgroup analysis by Gudas et al 21 demonstrated the superiority of mosaicplasty in younger patients (<25 years) compared with older patients (>25 years; <41 years), with significantly higher subjective patient outcomes and lower incidence of failure after 10 years compared with microfracture.
Limitations
This study has several limitations that are worth noting. The small number and quality of studies included in this review limit the generalizability of conclusions made herein. The quality of studies assessed using the MINORS criteria mainly was low or very low. Second, there was only 1 randomized control trial; however, the study did not isolate physeal status. Moreover, treatments were heterogeneous and did not follow a standardized treatment algorithm. Therefore, these studies were open to surgeon selection bias, and this review was relegated to a qualitative examination of the included studies. Osteochondral allograft was not a treatment method in any of the studies we included, not allowing us to comment on its efficacy. Validated patient-reported outcomes were not consistently used in all studies and, therefore, could not be examined objectively across all studies. Last, postoperative rehabilitation was not examined because of a lack of reporting, and its impact on RTS could not be further investigated. Further studies conducted in a prospective manner with either a comparison or randomization of surgical techniques in patients with open or closed physeal status are warranted to further support the findings of this study.
Conclusion
Our analysis revealed the treatment of unstable OCD lesions using the OATS technique demonstrated high rates of RTS across several studies. At the same time, microfracture alone exhibited the lowest RTS rate. Further, both arthroscopic and open internal fixation utilizing bioabsorbable screws yielded satisfactory RTS rates for juvenile patients with OCD.
Footnotes
Final revision submitted September 29, 2023; accepted January 1, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.B.F. has received grant support from Vericel; education payments from Liberty Surgical; consulting fees from Vericel, Innocoll, and Medical Device Business Services; nonconsulting fees from Vericel; and honoraria from Vericel. M.E.B. has received grant support from Arthrex; education payments from Arthrex and Smith+Nephew; and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.