
Abstract
Background:
Many professional baseball players experience low back pain, a major cause of which is lumbar facet joint arthropathy.
Purpose:
To evaluate the relationship between the dominant hand side and facet joint morphology in baseball movement.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Participants were 25 Japanese professional baseball players (11 pitchers and 14 fielders) with low back pain and lower limb symptoms. Player age, hand dominance, and length of professional playing experience were recorded, and the lateral diameter of all lumbar facet joints was determined from the axial computed tomography scans. We defined the facet joints ipsilateral and contralateral to the dominant hand as dominant and nondominant, respectively. The nondominant-to-dominant (N/D) ratio of the lateral diameter was calculated, and differences between the pitchers and fielders were analyzed using the unpaired t test.
Results:
The average player age and length of professional playing experience were 26.9 years (range, 19-37 years) and 7.2 years (range, 1-15 years), respectively. The right hand was dominant in 9 pitchers and 5 fielders, while the left hand was dominant in 2 pitchers and 9 fielders. In pitchers, the average lateral facet joint diameter on the nondominant side was significantly larger than on the dominant side at all vertebral levels except L1 to L2 (P < .05 for all). The N/D ratio for each facet joint was 1.06 (L1-L2), 1.11 (L2-L3), 1.10 (L3-L4), 1.12 (L4-L5), and 1.12 (L5-S1). In fielders, the average lateral facet joint diameter on the dominant side was significantly larger than on the nondominant side at L3 to L4 (P < .05), with N/D ratios of 0.98 (L1-L2), 0.96 (L2-L3), 0.94 (L3-L4), 0.97 (L4-L5), and 0.98 (L5-S1). The N/D ratio was significantly larger in pitchers than in fielders at all levels (P < .05 for all).
Conclusion:
The facet joints of professional baseball players were enlarged asymmetrically, with different tendencies observed between pitchers and fielders. Although pitching and batting are movements that transmit the rotation from the lower limbs to the upper limbs, the effects of rotation and lateral flexion were associated significantly with facet joint hypertrophy.
Low back pain is a common issue in athletes, with 75% reporting ≥1 episodes of back pain during their professional career. 13 In baseball players, the prevalence of low back pain is reported to be 3% to 15%, which is a serious problem that can lead to poor performance and forced retirement.15,21 Although low back pain is an issue not only for athletes but also for the general population, a cross-sectional study by Hangai et al 8 found that college student-athletes had a higher prevalence of low back pain than nonathletes. Furthermore, when they examined the incidence of low back pain based on the type of sport, students who played baseball were 3.2 times more likely to experience low back pain in their lifetime, the second highest rate after volleyball. 8 Although there are many causes of low back pain, 15% to 40% of all low back pain in the general population is linked to facet joint arthropathy.9,10,19 Morimoto et al 12 reported that facet joint arthritis accounts for 18% of the cause of low back pain in baseball players, which is consistent with these studies. Athletes need to perform complex movements that combine flexion and extension of the lumbar spine with lateral flexion and rotation with high load and repetition. In particular, pitching and batting in baseball transmit rotational force from the lower limbs to the upper limbs, and, over time, this phenomenon is thought to cause low back pain along with inflammation and stretching of the joint capsules.14,20 Therefore, we believe that the mechanical load on the facet joints due to the characteristic movements of baseball causes hypertrophy of the facet joints, which is among the changes observed in osteoarthritis.2,6 Two studies have focused on clinical findings of low back pain related to facet joints in baseball players, but none have examined the morphology involved.5,14
The aim of this study was to compare the morphology of the facet joints of professional baseball pitchers and fielders, as pitchers spend an overwhelming amount of time pitching, while fielders spend an overwhelming amount of time batting. We hypothesized that facet joint morphology would be different between pitchers and fielders, who repeatedly flex and rotate laterally in different directions.
Methods
The study protocol was approved by the ethics review board of our institution, and all participants provided written informed consent. Included were 25 Japanese professional baseball players (11 pitchers and 14 fielders) with an average of 7.2 years (range, 1-14 years) of professional playing experience, who were referred to our department of orthopaedics for further diagnosis or treatment for low back pain and lower limb symptoms such as sciatica and/or numbness. The average age of the players was 26.9 years (range, 19-37 years), and they had a mean height of 1.81 m (range, 1.71-1.90 m) and mean weight of 84.0 kg (range, 66-93 kg). The right hand was dominant in 9 pitchers and 5 fielders, while the left hand was dominant in 2 pitchers and 9 fielders.
Data Collection
All players were administered a questionnaire with items including age, dominant hand, and length of professional playing experience, and we measured the lateral diameter of the lumbar facet joints (L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1) as determined on axial computed tomography (CT) scans. Lumbar CT was performed with the consent of the patient, and multiplanar reconstruction images with 3 orthogonal directions (axial, sagittal, and coronal) were evaluated using commercial imaging viewer software (Aquarius NET Viewer; TeraRecon Inc).
The lateral diameter of each lumbar facet joint was defined as the distance connecting the center point between the superior and inferior articular processes at the superior endplate level of the vertebral body (Figure 1). The facet joints ipsilateral and contralateral to the dominant hand were defined as dominant and nondominant, respectively, and the nondominant-to-dominant (N/D) ratio was calculated by dividing the diameter on the nondominant side by the diameter on the dominant side. All measurements were performed independently by 2 certified orthopedic surgeons with more than 10 years of experience (H.M. and M.M.), and the average of the 2 values was used.

Lateral diameter of the facet joint ipsilateral to the dominant hand (dominant) and contralateral to the dominant hand (nondominant) as measured on axial CT scans for (A) right-handed players and (B) left-handed players. CT, computed tomography; D, dominant; L, left; N, nondominant; R, right.
Statistical Analysis
The interobserver reliability of the facet joint measurements was assessed. To assess intraobserver reliability, the observers measured twice within an interval of 1 month. Intra- and interobserver agreement was calculated using the weighted kappa statistic, with κ values being interpreted as poor (≤0.2), mild (>0.2≤0.4), moderate (>0.4≤0.6), good (>0.6≤0.8), or excellent (>0.8≤0.1).
Facet joint diameter between the dominant and nondominant sides in pitchers and fielders were analyzed by a paired t test. The differences in the N/D ratio between the pitchers and fielders were analyzed by an unpaired t test. In addition, we analyzed the correlation between the N/D ratio and player age as well as length of professional playing experience. P < .05 was considered statistically significant for all comparisons. All analyses were conducted using the Statistical Package for Social Sciences (Version 24; IBM Corp)
Results
The intra- and interobserver reliability of the facet joint diameter measurements indicated excellent agreement, with κ coefficient of 0.940 for intraobserver reliability and 0.978 for interobserver reliability.
The facet joint diameters for the dominant and nondominant sides are summarized in Table 1. In pitchers, the diameter of the nondominant side was significantly larger than that of the dominant side at all levels except L1 to L2 (P < .05 for all) (Table 1 and Figure 2A). The average N/D ratio for pitchers was >1.0 at all facet joint levels (Figure 2B). In fielders, the diameter of the dominant side was significantly larger than that of the nondominant side at L3 to L4 (P = .013) (Table 1 and Figure 3A), and the mean N/D ratio was <1.0 at all facet joint levels (Figure 3B).
Comparison of Facet Joint Diameter Between the Dominant and Nondominant Sides in Pitchers and Fielders a

Data are presented as mean ± SD. Boldface P values indicate statistically significant difference (P < .05).

Mean (A) lateral diameter and (B) N/D ratio for each facet joint in pitchers. Error bars indicate standard deviations. Significant difference: *P < .05, **P < .01. N/D, nondominant-to-dominant; ns, nonsignificant.

Mean (A) lateral diameter and (B) N/D ratio for each facet joint in fielders. Error bars indicate standard deviations. Significant difference: *P < .05. N/D, nondominant-to-dominant; ns, nonsignificant.
When the N/D ratios between pitchers and fielders were compared, the values were significantly larger in pitchers than in fielders at all vertebral levels (P < .05 for all) (Table 2 and Figure 4). There was no significant correlation between N/D ratio and age or length of professional playing experience at any vertebral level in pitchers or fielders (Appendix Figures A1 and A2).
Comparison of N/D Ratio Between Pitchers and Fielders a

Data are presented as mean ± SD. Boldface P values indicate statistically significant difference (P < .05). N/D, nondominant-to-dominant.
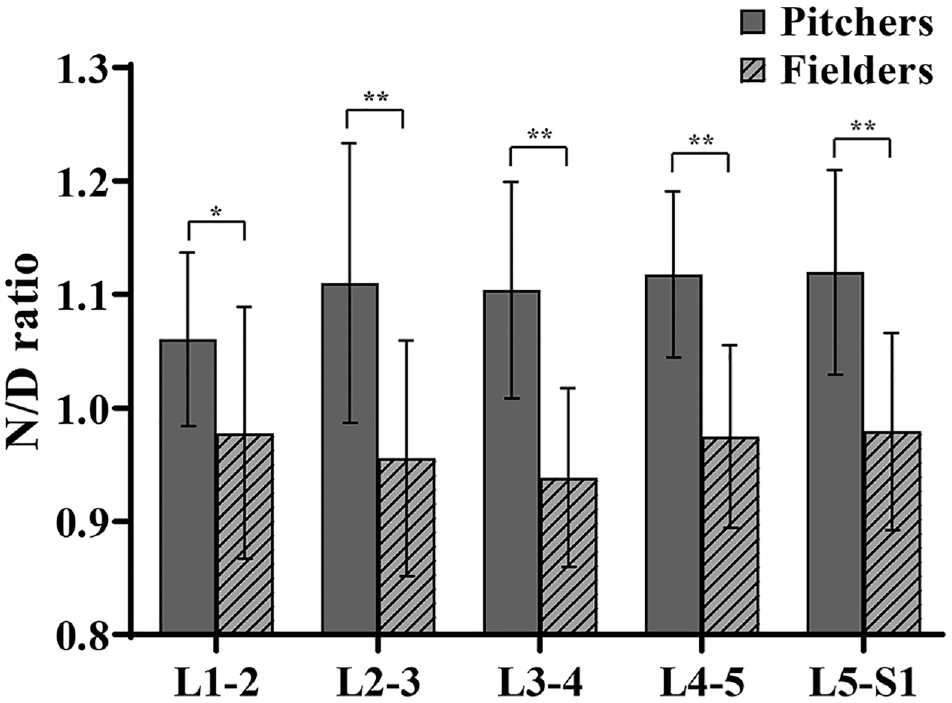
Comparison of mean N/D ratio for each facet joint between pitchers and fielders. Error bars indicate standard deviations. Significant difference: *P < .05, **P < .01. N/D, nondominant-to-dominant.
Osteoarthritic changes such as subchondral osteosclerosis and osteophytes were observed in the hypertrophic facet joints, and these changes were remarkable on the nondominant side in pitchers and on the dominant side in fielders (Figure 5).

Representative axial CT scans of study participants. (A) Right-handed pitchers showed osteophyte hypertrophy, subchondral osteosclerosis, and hypertrophy on the left facet joint, and left-handed pitchers showed these changes on the right facet joint. (B) Right-handed fielders showed similar changes of osteophyte hypertrophy, subchondral osteosclerosis, and hypertrophy in the right facet joint, and left-handed fielders showed these changes on the left facet joint. Circles show osteoarthritic changes. CT, computed tomography; L, left; R, right.
Discussion
Our major findings from this research revealed that the N/D ratio for pitchers was >1.0 for all facet joints (L1-L2, 1.06; L2-L3, 1.11; L3-L4, 1.10; L4-L5, 1.12; and L5-S1, 1.12), while the N/D ratio for fielders was <1.0 (L1-L2, 0.98; L2-L3, 0.96; L3-L4, 0.94; L4-L5, 0.97; and L5-S1, 0.98), and the N/D ratio was significantly greater for pitchers than for fielders at all vertebral levels (P < .05). This suggests that the facet joints were hypertrophied on the contralateral side of the dominant hand for pitchers and on the ipsilateral side for fielders. Furthermore, there was no significant correlation between N/D ratio and age or length of professional playing experience.
Lumbar facet joint disease is closely related to low back pain, not only in baseball players but also in athletes of various other sports. 3 For example, it has been reported that about 70% of asymptomatic elite teenage tennis players have at least 1 level of evidence of facet joint disease. 1 Therefore, it is very important to elucidate the mechanism of facet joint disorders in sports activities. In baseball, both pitching and batting movements transmit rotation from the lower limbs to the upper limbs via the trunk. For professional players in particular, these movements are repeated a large number of times in a specific direction, and it is therefore thought that considerable load is applied to 1 side of the lumbar spine. In the present study, the facet joints of the professional baseball players were asymmetrically enlarged, with different tendencies observed between pitchers and fielders. There are 2 possible causes for this discrepancy.
The first possibility is lumbar rotation. Facet joint injuries usually occur during rotation with the lumbar in extension and are well known to cause lumbar and trunk disorders,3,22 especially in the direction opposite to rotation.2,20 Interestingly, hypertrophy of the facet joint in the direction opposite to rotation has been reported in hammer throwers who repeatedly perform extension rotation. 18 To explain this phenomenon, Sairyo et al 17 used finite-element analysis to show that rotation added to lumbar extension results in maximum load around the facet joint opposite to the direction of rotation. In pitchers, rotation added to lumbar extension occurs in the direction of the dominant hand in the late cocking phase when the lumbar spine is hyperextended (right for right-handed pitchers, left for left-handed pitchers). 4 As a result, the facet joint in the direction opposite to the dominant hand becomes loaded. In contrast, in fielders, the lumbar spine becomes hyperextended in the follow-through phase, during which right-handed fielders rotate to the left and left-handed fielders rotate to the right. Therefore, turning to the side opposite the dominant hand causes loading of the ipsilateral facet joint.
The second possible cause is the effect of lateral bending. Lateral bending of the lumbar spine in sports activities is also a cause of lumbar disorders and has been reported in biomechanical studies to cause loading of the facet joints.7,11,16 Immediately before the release of the ball, which requires maximum power, the pitcher bends laterally to the side opposite the dominant hand. 4 It has been reported that pitchers with inadequate spinal stabilization have increased lumbar hyperextension and lateral bending of the trunk from the moment of max cocking through ball release. 5 In contrast, fielders laterally bend to the same side as the dominant hand at the moment of contact with the ball. In other words, the opposite direction of lateral flexion at the moment of maximum output occurs that the facet joint hypertrophy is also opposite. These 2 factors strongly support the results of the present study. The reason why there was no correlation between N/D ratio and age and years of professional playing experience is thought to be that asymmetric enlargement of the facet joints had already appeared because even young players had already undergone repeated rotation and lateral bending of the lumbar spine due to a considerable amount of practice before becoming professional baseball players.
Limitations
There are several limitations to this study. First, only the lateral diameter of the joint was measured and morphology was not evaluated in detail. Currently, there is no established method for the classification of osteoarthritis based on CT findings. If the degree of facet joint degeneration could be scaled, detailed assessment and common recognition might be easier. Second, although there was a maximum age difference of approximately 20 years between the athletes in this study, age-related changes were not taken into account. Morimoto et al 12 reported that the incidence of lumbar degeneration-related diseases increases with age in professional baseball players. Such degenerative changes in the bilateral facet joints might result in a smaller lateral diameter ratio that would affect the accuracy of the results. Last, only a morphological evaluation was made and clinical symptoms of facet joint disease such as low back pain were not considered. It should be noted that CT findings do not always correspond to clinical findings.
Conclusion
The facet joints of professional baseball players were enlarged asymmetrically, with different tendencies observed between pitchers and fielders. Although pitching and batting are movements that transmit the rotation from the lower limbs to the upper limbs, the effects of rotation and lateral flexion were significantly associated with facet joint hypertrophy. These findings can help our understanding of the mechanism of facet joint disorders in professional baseball players and all athletes who perform repetitive rotational movements.
Footnotes
Appendix
Final revision submitted May 22, 2023; accepted July 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support was received from the Japan Orthopaedics and Traumatology Research Foundation (grant J4437). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tokushima University (reference No. 3060).