
Abstract
Background:
Poor postoperative quadriceps muscle strength recovery after anterior cruciate ligament reconstruction (ACLR) leads to delayed return to sports and lower patient satisfaction.
Purpose/Hypothesis:
The purpose of this study was to examine factors that affect quadriceps muscle strength 1 year after ACLR. It was hypothesized that older age, poor preoperative quadriceps muscle strength, and residual pain would be risk factors for poor quadriceps muscle strength recovery.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Included were patients from multiple institutions who underwent primary ACLR using autologous hamstring tendon grafts between August 1, 2013, and March 31, 2018, and who had at least 1 year of follow-up data. Patients with past ligamentous injuries in the affected knee, previous injuries or operations in the contralateral knee, accompanying ligament injuries of grade 2 or 3, or inflammatory or other types of osteoarthritis were excluded. Patients were categorized as having muscle strength ≥80% (good strength recovery) or <80% (poor strength recovery) compared with the contralateral leg at 1 year postoperatively. Multivariate logistic regression analysis was performed to investigate the factors influencing postoperative quadriceps muscle strength. In addition, a categorical analysis was conducted based on factors extracted by the multivariate logistic regression analysis.
Results:
A total of 402 patients were included. Multivariate logistic regression analysis revealed that age at surgery (P = .020), preoperative quadriceps muscle strength (P = .006), and postoperative Knee injury and Osteoarthritis Outcome Score (KOOS)-Pain score (P = .002) were significantly associated with quadriceps muscle strength at 1 year postoperatively. The odds of poor muscle strength recovery according to categorical analysis were 5.0-fold higher for patients aged >40 versus ≤20 years, 4.2-fold higher for those with preoperative quadriceps muscle index <60% versus ≥80%, and 7.7-fold higher for those with a postoperative KOOS-Pain score of <85 versus 100.
Conclusion:
Older age, poor preoperative quadriceps muscle strength, and low postoperative KOOS-Pain score were risk factors for poor quadriceps muscle strength 1 year after primary ACLR. Surgical indications, including age, preoperative active rehabilitation, and pain control, should be considered for optimization of postoperative quadriceps muscle strength recovery.
Keywords
Anterior cruciate ligament (ACL) injury is a common knee injury during sports. 19 ACL reconstruction (ACLR) is the gold standard treatment for ACL injury management to achieve knee stability restoration, good patient-based subjective evaluation, and return to sports.17,27,30,31 However, muscle strength recovery greatly affects the degree of recovery after ACLR, particularly for the quadriceps femoris muscle.6,18,23,24,26 Poor postoperative quadriceps muscle strength recovery causes delayed return to sports and lowered patient satisfaction.15,32 Therefore, adequate quadriceps muscle strength recovery after ACLR is important for a safe return to sports.
Several factors affecting quadriceps muscle strength recovery after ACLR have been identified to date. Preoperative quadriceps muscle strength was reportedly associated with postoperative quadriceps muscle strength recovery after hamstring tendon reconstruction.9,12,28 A previous study reported that weak preoperative quadriceps muscle strength and small-width patellar tendons hindered postoperative muscle recovery in ACLR using a bone-patellar tendon-bone (BTB) graft. 25 Age has been considered another important factor. Although a good clinical prognosis could be achieved in ACLR, even in patients aged over 50 years, several studies showed that advanced age was associated with postoperative muscle weakness.3,4,11,28 Other factors, such as sex, graft type, and pain, reportedly affect quadriceps muscle strength postoperative recovery.8,9,28 Despite identifying these risk factors, confounding factors were not sufficiently adjusted in previous reports. Moreover, their sample sizes were not large enough for multiple regression analysis.
In this study, we aimed to examine factors that affect quadriceps muscle strength 1 year after ACLR in a large multicenter cohort so as to contribute to reconsidering pre- and postoperative management and surgical indications. We hypothesized that older age, poor preoperative quadriceps muscle strength, and residual pain would be risk factors for poor quadriceps muscle strength recovery at 1 year after ACLR.
Methods
Study Design
The protocol for this study received approval from the institutional review board (IRB) of Tokyo Medical and Dental University (TMDU), and all participating sites either obtained approval from the local IRB or delegated their approval to the TMDU IRB. This prospective longitudinal multicenter cohort study was conducted from August 1, 2013, to March 31, 2018. Our study group, the TMDU Multicenter Arthroscopic Knee Surgery (TMDU MAKS) Group, comprised more than 30 sports orthopaedic surgeons from 12 academic medical centers. Each surgeon was permitted to decide on the surgical indications and methods, although the same surgical records and evaluation forms were required. Before participating in the study, all surgeons completed a training course at TMDU on knee arthroscopy, and all surgeons received instructions to assess physical examination findings in the same manner.
Participants
Included in this study were patients who were registered in the multicenter study database as having undergone primary ACLR with autologous hamstring tendon graft between August 1, 2013, and March 31, 2018. The semitendinosus tendon was used, and the gracilis was also harvested when necessary. In principle, a single-bundle reconstruction was performed by folding the harvested tendon into quadruple folds (4 strands), and a double-bundle reconstruction was performed by folding the harvested tendon into double folds (2 strands). All patients had at least 1 year of follow-up data. Exclusion criteria were as follows: (1) past ligamentous injuries in the affected knee; (2) previous injuries or operations in the contralateral knee; (3) accompanying ligament injuries of grade 2 or 3; and (4) inflammatory or other types of osteoarthritis. Patients with missing data and those with reinjuries within 1 year after surgery were also excluded.
The included patients were divided into 2 groups. Patients with good muscle strength recovery (GR group) had 80% or more of quadriceps muscle strength compared with that of the unaffected leg at 1 year after ACLR, while patients with poor muscle strength recovery (PR group) had less than 80% of quadriceps muscle strength at 1 year postoperatively. Based on a study by de Jong et al, 5 who reported that a quadriceps strength deficit of almost 20% persists 1 year after ACLR, we selected 80% of muscle recovery as the cutoff value.
Patients completed a registration form with questions about their age, sex, and social background. The form also included questions about their occupation, education level, sports engagement, and activity or sports at the time of injury. The Knee injury and Osteoarthritis Outcome Score (KOOS), Lysholm knee scale, and International Knee Documentation Committee (IKDC) subjective score were used for assessment of patient-reported outcomes.
At the time of surgery, surgeons completed a data form documenting physical examination findings under anesthesia, arthroscopic findings (including status of the meniscus and articular cartilage), and treatment details (including graft choice and fixation methods). Postoperatively, prospective patient follow-ups were conducted at 3 months, 1 year, 2 years, and annually thereafter. Surgeons filled out a postoperative form with all physical examination findings pertaining to the menisci and ligaments of the knees. The patients also completed the KOOS, Lysholm, and IKDC scores at each visit.
Patients underwent nearly the same rehabilitation protocol before and after surgery (Supplemental Table S1). However, there were differences in the initiation timing of range of motion exercises and weight-restriction period, which depended on concomitant procedures (eg, meniscal procedures). The protocol, composed of a time-based menu according to the time after surgery, was conducted in the outpatient rehabilitation center of each hospital or clinic. Patients were allowed to be discharged from the hospital when the following criteria were met: (1) knee flexion achieved more than 90°; (2) straight-leg raises were able to be performed; (3) walking was smooth with the aid of crutches and braces; and (4) the wound was clear, not infected. Most patients returned home about 2 weeks after the operation. After discharge, patients periodically visited the hospital for rehabilitation and were supervised by a physical therapist while exercising. Patients who recovered more than 60% muscle strength compared with the healthy side were allowed to begin jogging 3 months postoperatively, based on previous studies.10,14,20 Patients who recovered more than approximately 90% muscle strength were permitted full athletic activities at a minimum of 6 months postoperatively.
Measurements Evaluated
We included assessments of quadriceps maximal isokinetic muscle strength from preoperatively and 1 year postoperatively. The muscle strength test was conducted using a dynamometer (Biodex System 4; Biodex Medical Systems) with the patient in a sitting position with the trunk firmly fixed on the seat at 90° of hip flexion and 90° of knee flexion. Patients were warmed up using the equipment for 5 minutes at low resistance, then the test was conducted, first on the unaffected leg and next on the affected leg. Every patient performed 5 maximum effort contractions at 60 deg/s, and the maximum extension torque was measured. The quadriceps strength index was computed by normalizing the peak torque of the affected leg to that of the unaffected leg.
Also evaluated were the pivot-shift test, Lachman test, and KT-1000 arthrometer readings at 1 year postoperatively. The pivot-shift test was assessed in accordance with the IKDC criteria (negative; 1+, glide; 2+, clunk; 3+, gross). The Lachman test was assessed using 4 grades of negative, 1+, 2+, or 3+, according to the IKDC criteria. The KT-1000 arthrometer (MED Metric) manual maximal test (side-to-side difference between the affected and unaffected knees in 0.5-mm increments) was used to indicate anterior knee laxity.
Statistical Analysis
Data between the GR and PR groups were compared using the chi-square test for categorical variables and the Student t test or Mann-Whitney U test for continuous variables with normal or nonnormal distributions, as appropriate. We then performed a univariate logistic regression analysis, with the objective variable being quadriceps muscle strength at 1 year postoperatively. Explanatory variables in demographic, preoperative, and intraoperative items included age, sex, preoperative Tegner score, preoperative quadriceps muscle strength, reconstruction method (single- or double-bundle), meniscal procedure (excision or repair/lateral or medial meniscus), and operation time. Explanatory variables at 1 year postoperatively were extension and flexion range of motion, Lachman test, pivot-shift test, side-to-side difference in anterior knee laxity, and KOOS-Pain score. Multivariate logistic regression analysis using a forced-entry method was then performed on variables with a P value <.2. In addition, we performed a categorical analysis of factors extracted from the multivariate analysis. Statistical analyses were performed using the EZR software. 13 Statistical significance was set at P < .05 for all tests.
The sample size of this study was estimated as follows. Based on a previous study, 10 the standard deviation of quadriceps strength 1 year after ACLR was fixed at approximately 18.5%. Given that a 10% difference in preoperative quadriceps muscle strength is clinically significant, 28 156 patients were required as the minimum sample size to obtain an α of .05 and a β of 0.80.
Results
Based on the eligibility criteria, 597 patients were included in this study. Of these patients, 195 (32.7%) were lost to follow-up; thus, data from 402 patients were ultimately included in the study (Figure 1). There were 312 patients in the GR group and 90 patients in the PR group. Patient demographic, preoperative, intraoperative, and postoperative data are presented in Table 1. The mean ±SD quadriceps index 1 year after surgery was 90.8% ± 16.1%. Significant differences between the 2 groups were found regarding age at surgery, preoperative Tegner activity scale, preoperative quadriceps muscle strength, operation time, KOOS-Pain score, and quadriceps muscle strength at 1 year postoperatively.
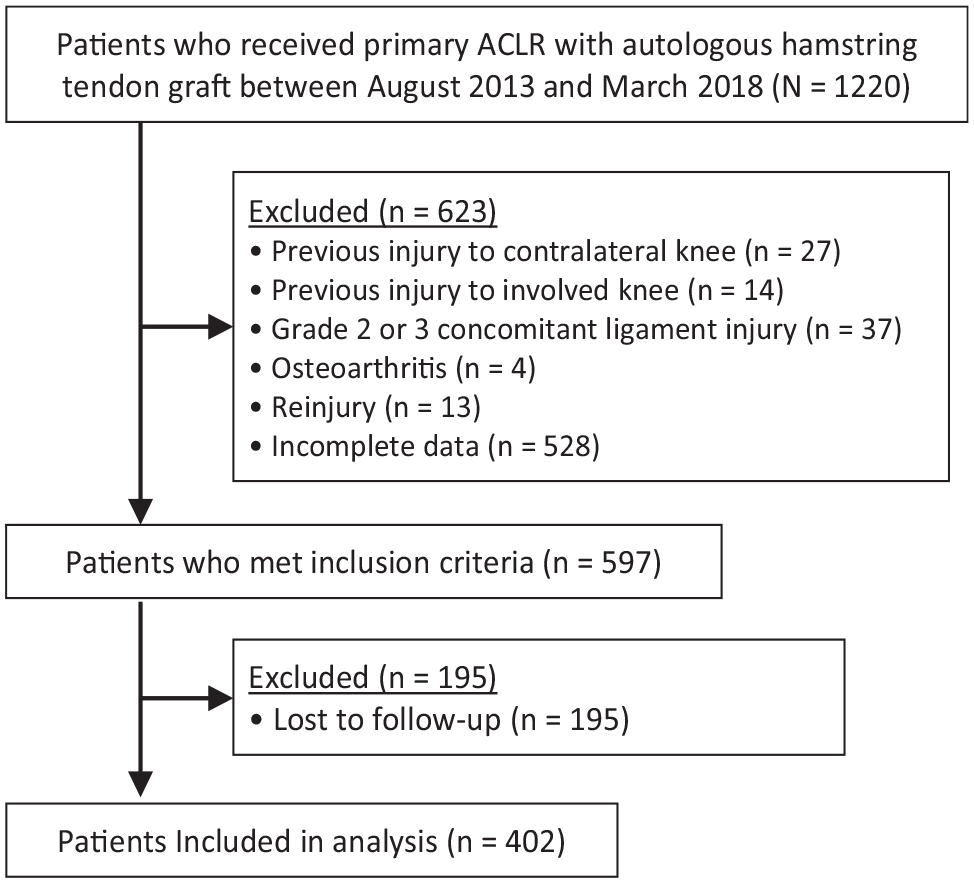
Flow diagram of patient recruitment and inclusion. ACLR, anterior cruciate ligament reconstruction.
Patient Preoperative, Intraoperative, and Postoperative Data a
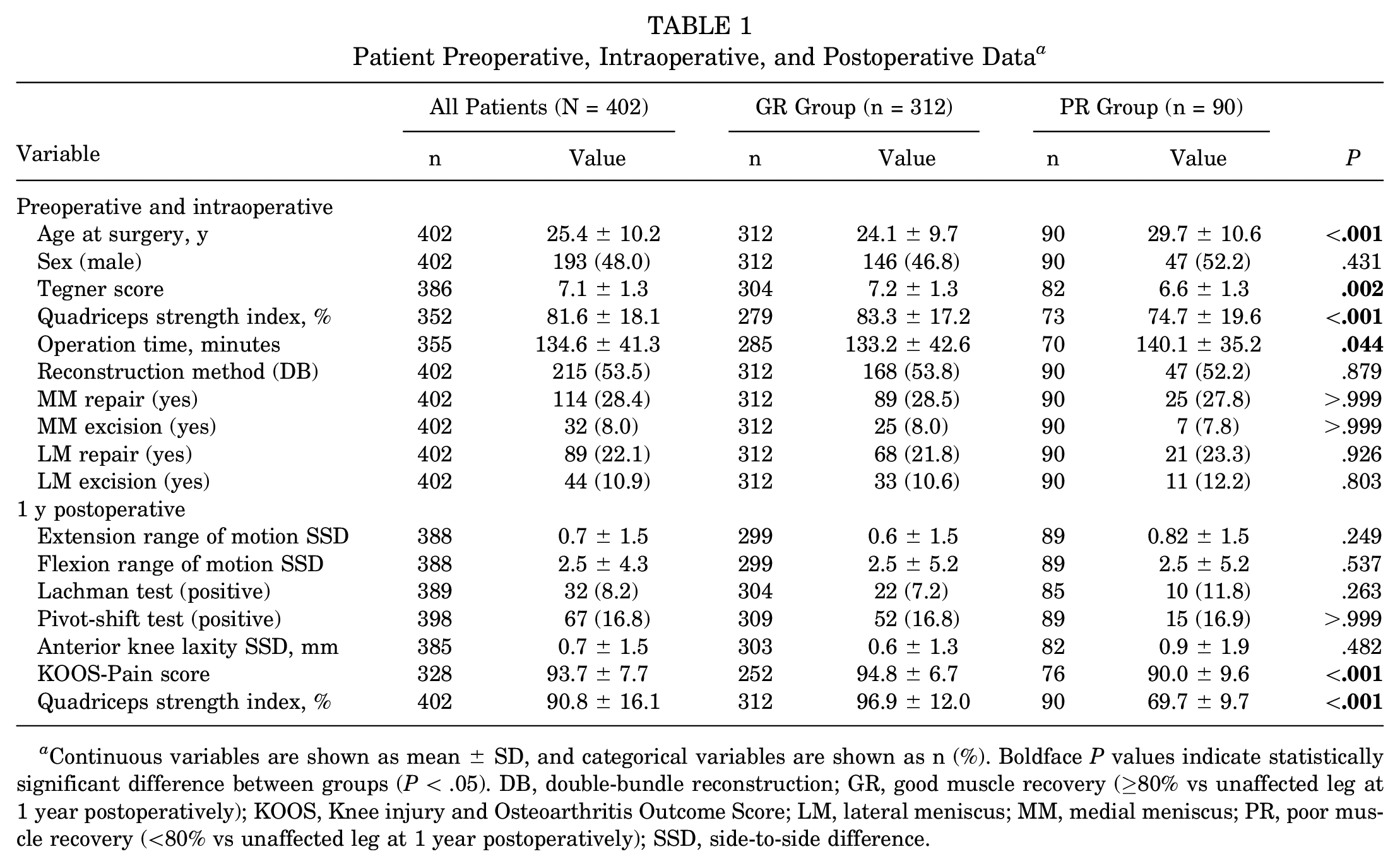
Continuous variables are shown as mean ± SD, and categorical variables are shown as n (%). Boldface P values indicate statistically significant difference between groups (P < .05). DB, double-bundle reconstruction; GR, good muscle recovery (≥80% vs unaffected leg at 1 year postoperatively); KOOS, Knee injury and Osteoarthritis Outcome Score; LM, lateral meniscus; MM, medial meniscus; PR, poor muscle recovery (<80% vs unaffected leg at 1 year postoperatively); SSD, side-to-side difference.
Univariate logistic regression analysis revealed significant differences between the GR and PR groups in age at surgery, preoperative Tegner score, preoperative quadriceps strength index, and KOOS-Pain score (P < .001 for all). Side-to-side difference in anterior knee laxity was included in the subsequent analysis of factors with P < .2 (Table 2).
Results of the Univariate Logistic Regression Analysis a
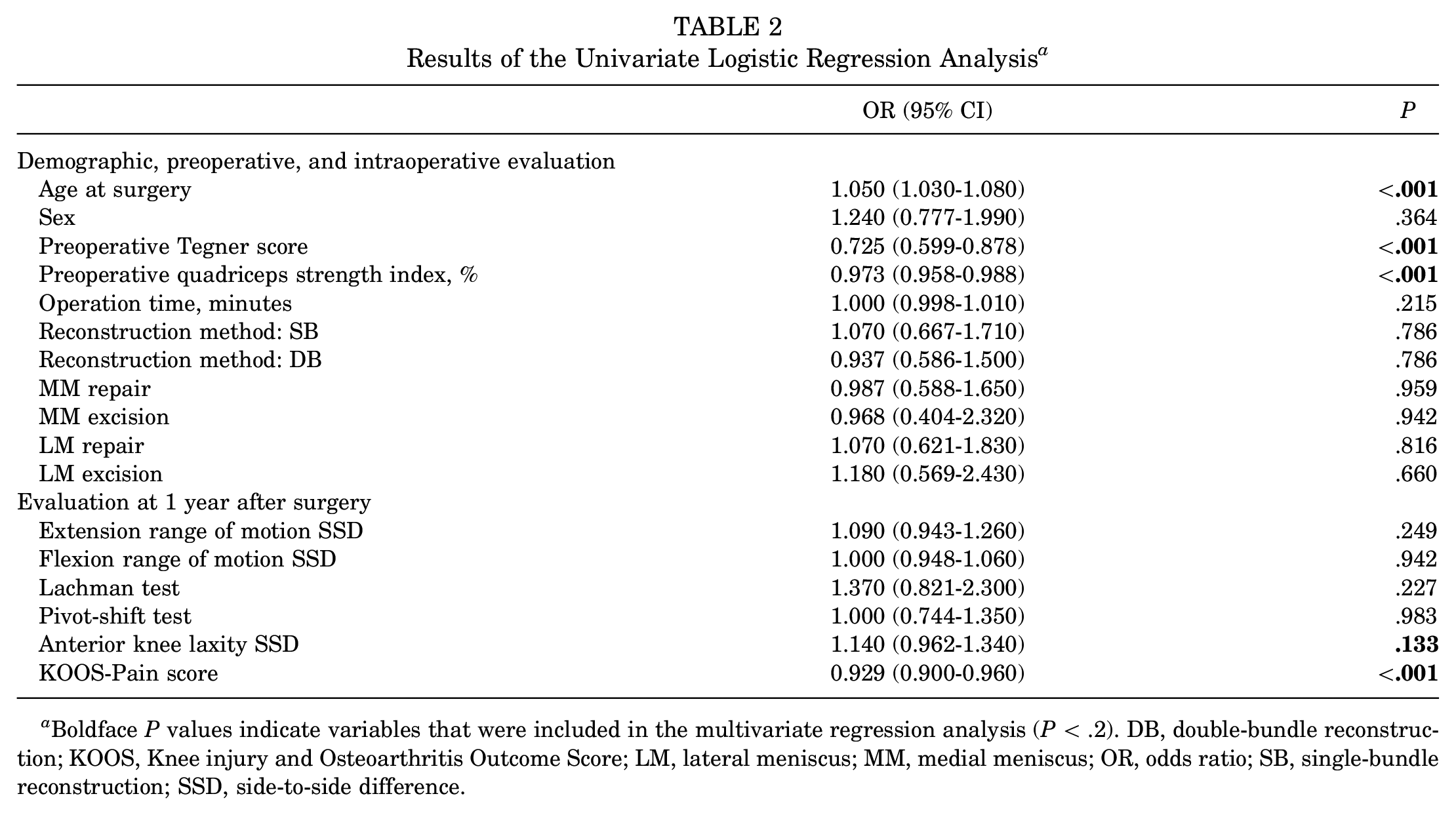
Boldface P values indicate variables that were included in the multivariate regression analysis (P < .2). DB, double-bundle reconstruction; KOOS, Knee injury and Osteoarthritis Outcome Score; LM, lateral meniscus; MM, medial meniscus; OR, odds ratio; SB, single-bundle reconstruction; SSD, side-to-side difference.
Multivariate logistic regression analysis revealed that age at surgery (odds ratio [OR], 1.040; 95% CI, 1.010-1.070; P = .020), preoperative quadriceps muscle strength (OR, 0.976; 95% CI, 0.959-0.993; P = .006), and postoperative KOOS-Pain score (OR, 0.940; 95% CI, 0.905-0.978; P = .002) were associated independently with quadriceps muscle strength at 1 year after surgery (Table 3). In an additional univariate/multivariate analysis with a cutoff of 90%, only postoperative KOOS-Pain score (OR, 0.960; 95% CI, 0.924-0.997; P = .034) was associated independently with quadriceps muscle strength at 1 year after surgery (Supplemental Tables S2 and S3).
Results of the Multivariate Logistic Regression Analysis a

Boldface P values indicate statistical significance (P < .05). KOOS, Knee injury and Osteoarthritis Outcome Score; OR, odds ratio; SSD, side-to-side difference.
Categorical analysis of the 3 significant factors from the multivariate analysis was performed. We classified age at surgery into 6 categories (≤20 [reference variable], 21-25, 26-30, 31-35, 36-40, >40 years), preoperative quadriceps strength index into 4 categories (≥80% [reference variable], 79.9%-70%, 69.9%-60%, and <60%), and postoperative KOOS-Pain into 5 categories (100 [reference variable], 99.99-95, 94.99-90, 89.99-85, and <85) and compared the OR of quadriceps muscle strength at 1 year postoperatively in each category against the reference variable (Table 4). The risk of poor quadriceps muscle recovery was 5.0-fold higher in patients aged >40 versus ≤20 years, 4.2-fold higher in patients with a preoperative quadriceps muscle index of <60% versus ≥80%, and 7.7-fold higher in patients with a postoperative KOOS-Pain score of <85 versus 100 points.
Results of Categorical Analysis a

Boldface P values indicate statistically significant difference compared with reference variable (P < .05). KOOS, Knee injury and Osteoarthritis Outcome Score; OR, odds ratio.
Discussion
The most important finding of this study was that older age at surgery, poor preoperative quadriceps muscle strength, and low postoperative KOOS-Pain score were associated independently with poor quadriceps muscle strength (<80% of the unaffected leg) at 1 year after primary ACLR with autologous hamstring tendon graft.
Some studies have reported that age affected the recovery of quadriceps muscle strength after ACLR. Using logistic regression analysis, Iriuchishima et al 11 reported that age was the only factor associated with the recovery of quadriceps muscle strength after ACLR. They suggested that rehabilitation for elderly patients after ACLR needs to be continued carefully because of mild knee osteoarthritis. Ueda et al 28 used multivariate logistic regression analysis and reported that age was associated with recovery of quadriceps muscle strength after ACLR. These authors included only patients with a preinjury Tegner activity scale of at least 7, and even the mean age of the group with poor quadriceps strength recovery was young (22.0 ± 7.3 years). In light of these studies, older age at the time of surgery could lead to poorer recovery of quadriceps muscle strength after ACLR. In the current study, the OR for postoperative quadriceps muscle recovery was reversed between the age group of 31 to 35 years and the group of 36 to 40 years in the categorical analysis (Table 4). However, overall, older age was a risk factor for poor postoperative quadriceps muscle recovery.
Preoperative quadriceps muscle strength has been most frequently reported to be associated with postoperative quadriceps muscle strength recovery after ACLR.5,6,9,12,25,28 Iwame et al 12 performed a multiple regression analysis in a study of 101 patients who underwent double-bundle ACLR using the hamstring tendon and reported that preoperative muscle strength was the only factor affecting quadriceps muscle strength recovery after ACLR. Shelbourne and Johnson 25 reported that patients with preoperative quadriceps muscle strength index >90% showed significantly better quadriceps muscle strength at 1, 2, 3, 12, and 24 months after ACLR using a BTB graft. de Jong et al 5 compared the recovery of quadriceps muscle strength after ACLR in patients who received a BTB graft versus those who received a hamstring tendon graft and revealed a significant correlation between the pre- and postoperative quadriceps muscle strength indices. These reports indicated that preoperative quadriceps muscle strength was an independent factor affecting postoperative quadriceps muscle strength, regardless of the reconstruction method, graft type, or analysis method, which was supported by our results.
Pain was reportedly associated with deficits in quadriceps strength.21,28 Natri et al 21 divided 119 patients after ACLR into acute and chronic groups according to the time from injury to surgery and analyzed the determinants of muscle strength recovery. Using a multiple stepwise regression analysis, the authors reported that patellofemoral pain was significantly associated with poor extension muscle recovery in both acute and chronic groups. Although this finding supported our results, our study is the first to independently report a logistic regression analysis using the KOOS-Pain score. In addition, several reports indicated that postoperative pain was stronger in women, and there was a correlation between sex and pain.2,8,22 However, sex was not independently identified as a risk factor for poor quadriceps muscle recovery in this study. The association between sex and quadriceps muscle strength after ACLR should be investigated further in future clinical studies. Several studies also reported that rehabilitation was useful for muscle strength recovery, range of motion, and pain relief.7,29 It is important to reevaluate the timing, method, and duration of rehabilitation for muscle recovery after ACLR.
In this study, it appeared that some patients still had positive Lachman and pivot-shift tests postsurgery. Akoto et al 1 reported that 15% to 17% of the patients showed positive Lachman and pivot-shift tests at 1 year after ACLR with quadrupled hamstring tendon grafts. This result was similar to, or slightly worse than, our findings. Another study showed that almost 50% of patients who underwent initial ACLR with 4-strand semitendinosus-gracilis autografts showed positive Lachman and pivot shift tests, although the assessment was performed 2 years after ACLR. 16
Strengths and Limitations
This study has some strengths. First, it was a relatively large-scale multicenter study that met the requirement of the calculated sample size. While various factors that affected postoperative muscle recovery have been identified, the sample sizes of many previous studies were limited. In this regard, our findings supported previous results with adequate statistical power. Second, this study provides information on the reliability of results obtained previously through multivariate analysis by including more explanatory variables. Previous studies may have led to biased results due to a lack of consideration for the relationships between necessary factors for multivariate analysis. Furthermore, by clarifying the degree of risk associated with the identified factors through categorical analysis, it would be easier for each surgeon to recognize the risks, create treatment plans, and explain the risks to patients.
This study also has some limitations. First, variables related to postoperative muscle recovery, such as body mass index and time from injury to surgery, were not included. However, most related factors mentioned in previous reports were included. Second, the follow-up period was relatively short. However, considering the time to return to sports, muscle strength 1 year after surgery might be a reasonable evaluation period. Third, we did not consider inter- and intrarater reliabilities in muscle strength measurements. However, all surgeons received instructions to measure muscle strength in the same manner as before the study initiation. Fourth, there were many lost data and low follow-up rates, which could represent a bias. Fifth, this study did not include cases with a BTB graft or a quadriceps tendon autograft. Sixth, due to multicenter studies, many physical therapists were involved in different hospitals, and rehabilitation could not be completely standardized even though our group was trained in the same academic university and all surgeons had the same principle of rehabilitation. This could affect muscle recovery after ACLR. Finally, rehabilitation compliance was not measured in this study.
Conclusion
Older age at surgery, lower preoperative quadriceps muscle strength, and lower KOOS-Pain score were associated with poor quadriceps muscle strength 1 year after primary ACLR with autologous hamstring tendon grafts. Surgical indications, including age, recovery of quadriceps muscle strength before surgery, and pain control after surgery and during the subsequent rehabilitation period, should be considered for quadriceps muscle strength recovery after ACLR.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231194593 – Supplemental material for Older Age, Poor Preoperative Quadriceps Muscle Strength, and Residual Pain as Risk Factors for Poor Quadriceps Muscle Strength Recovery at 1 Year After ACL Reconstruction: A TMDU MAKS Study of 402 Patients
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231194593 for Older Age, Poor Preoperative Quadriceps Muscle Strength, and Residual Pain as Risk Factors for Poor Quadriceps Muscle Strength Recovery at 1 Year After ACL Reconstruction: A TMDU MAKS Study of 402 Patients by Shoichi Hasegawa, Yusuke Nakagawa, Aritoshi Yoshihara, Tomomasa Nakamura, Hiroki Katagiri, Masaya Hayashi, Hideya Yoshimura, Tsuyoshi Nagase, Ichiro Sekiya and Hideyuki Koga in The Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Atsushi Okawa, MD, PhD, for continuous support; Tatsuhiko Anzai for consultation of data analysis; and Masayo Tsukamoto and Miyoko Ojima for data registration. The authors acknowledge the following study collaborators: Akiho Hoshino, MD, PhD; Toru Takahashi, MD, PhD; Etsuko Matsumura, MD, PhD; Kaori Nakamura, MD, PhD; Mari Uomizu, MD, PhD (Kawaguchikogyo General Hospital); Tomohiko Tateishi, MD, PhD, and Tadanori Shimizu, MD, PhD (Doai Memorial Hospital); Koji Asano, MD, PhD, and Mindae Kim, MD, PhD (Yokohama Minato Red Cross Hospital); Jyu Neishin, MD, PhD, and Mio Udo, MD, PhD (Tama-Hokubu Medical Center); Jun Kitahama, MD (Nitobe Memorial Nakano General Hospital); Shinichi Shirasawa, MD, PhD (Suwa Central Hospital); Katsuaki Yanagisawa, MD, PhD (Nissan Tamagawa Hospital); Shinpei Kondo, MD, PhD (National Hospital Organization Disaster Medical Center); Daisuke Hatsushika, MD, PhD (Tsuchiura Kyodo General Hospital); Arata Yuki, MD, PhD (Soka City Hospital); Enichi Nakatsuru, MD (Tokyo Bay Urayasu Ichikawa Medical Center); and Naoko Araya, MD; Masaki Amemiya, MD; Jae-Sung An, MD; Kazumasa Kawata, MD; and Masaaki Isono, MD (Tokyo Medical and Dental University Hospital).
Final revision submitted March 29, 2023; accepted May 4, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tokyo Medical and Dental University (study protocol: 1547).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.