
Abstract
Background:
Semitendinosus/gracilis (STG) tendon autograft has been used effectively for restoring knee stability after anterior cruciate ligament (ACL) rupture. Though ACL reconstruction with STG autograft is an effective surgical technique for return to sports, short-term hamstring strength asymmetries exist after surgery. Although imaging evidence has demonstrated regrowth and reorganization of the semitendinosus (ST) tendon, no studies show whether the regrowth is associated with residual muscle function. Continuous shear wave elastography (cSWE) using an external actuator and high–frame rate ultrasound is a promising technique for evaluating the mechanical properties of regrown tendons in vivo.
Purpose:
To demonstrate recovery of the mechanical properties of the hamstring tendons after ACL reconstruction using an STG tendon autograft.
Study Design:
Case series; Level of evidence, 4.
Methods:
Thirteen patients underwent an STG autograft reconstruction after ACL rupture. Regrowth of the ST tendon was confirmed via b-mode ultrasound between 6 and 24 months postreconstruction. The shear elastic (µ 1) and viscosity moduli (µ 2) of the ST tendons were ascertained through cSWE using an external actuator and high–frame rate ultrasound.
Results:
Significant differences in both shear elastic (129.4 vs 73.0 kPa) and viscous moduli (192.6 vs 114.3 Pa·s) existed bilaterally for uninvolved and involved limbs, respectively. Additionally, a positive correlation between time postoperative and shear elasticity was observed (r = 0.60). More than 12 months were required for patients to regain a large percentage of the tendon’s mechanical properties compared with the contralateral side (µ 1, 80.6% at >12 months vs 39.9%; µ 2, 78.7% at >12 months vs 46.0%).
Conclusion:
The imaging and elastography data demonstrate tendon regrowth and recovery of functional biomechanical properties with time. The elastic modulus of the recovered tendon indicates the ability to transmit muscle force across the joint and recovery of semitendinosus function after its use for an ACL graft.
Anterior cruciate ligament (ACL) tears are common sports injuries that have devastating short-term performance repercussions with the possibility of long-term debilitating effects. ACL tears are estimated to occur at a rate of 85 tears per 100,000 people in individuals between the ages of 16 and 39 years. 10 Short-term ramifications for those undergoing ACL reconstruction (ACLR) include the loss of sport participation and performance, with 82% of patients returning to competitive sport and only 64% returning to their preinjury competitive levels after ACLR. 1 Long-term effects of ACL rupture include strength asymmetries, residual pain, and osteoarthritis. The quality of life of the average patient is poorer 5 years after ACL rupture, and greater than 50% have signs of osteoarthritis 10 years after injury. 14,21 While the ability to return to sports has improved, surgeons have not been as successful in returning athletes at their preinjury participation levels and preventing the long-term consequences of ACL rupture and reconstruction.
Use of autografts yields a higher return-to-sport rate and lessened chance of rerupture than allografts, but harvesting autografts causes morbidity, including short-term strength deficits in the donor limb. 1 Understanding the consequences of the autograft resection will enable a greater understanding of strength asymmetry and postoperative surgical performance and will improve postoperative rehabilitation.
The semitendinosus (ST) and gracilis (GRA) muscles contribute to knee internal rotation and flexion strength. Hamstring strength is therefore affected by the use of an autologous ST/GRA tendon (hamstring) graft. Research has shown bilaterally symmetrical peak knee flexion torque at various time points of 12 months, 17 24 months, 16 and 18 to 51 months 15 postreconstruction, with subsequent hamstring muscles hypertrophy to compensate after greater than 10 years. 3,23 The regeneration and restructuring of the tendon progresses from the initial neotendon until 24 months after surgery. 7,8,18,20
Continuous shear wave elastography (cSWE) is a novel ultrasound imaging technique that evaluates the viscoelastic properties of soft tissue in vivo. 4,24 The amount a tendon stretches when loaded, or elasticity, is what enables it to pass force from the muscle to bony attachment and create joint torque. The tendon reorganizes as it heals, and this is related to the elastic properties of the tendon. 19,22 The ability to measure the elastic properties of the ST tendon in vivo could establish the functional ability of the tendon and, hence, its biomechanical competence. Therefore, the purpose of this study was to evaluate the viscoelastic properties of the regrown ST tendon post-ACLR, using cSWE, and compare them with the contralateral, uninvolved limb. We hypothesized that there will be a significant difference in the shear elastic modulus between the involved and uninvolved ST tendon after tendon resection. We also hypothesized that the symmetry of the tendons’ mechanical properties will be related to time postoperative. Identifying the tissue quality and time course of functional recovery of the ST tendon would create an opportunity to reduce strength and kinematic deficits by aiding in developing a rehabilitation protocol to leverage the regrowth phenomenon.
Methods
Thirteen patients (age, 21.0 ± 2.5 years; height, 174.5 ± 9.8 cm; mass, 75.7 ± 13.0 kg; 10 males, 3 females) who had sustained a unilateral ACL rupture with no concomitant ligament tears of greater than grade I were recruited through the physical therapy clinic associated with the researching university. Each patient had an ACLR using ST/GRA tissue as the ACL autograft. Patients were between 6 and 24 months postreconstruction. Nine participants without an ACL tear or any other lower extremity injury served as the comparison group (age, 27.1 ± 6.6 years; height, 171.2 ± 10.4 cm; mass, 64.3 ± 13.0 kg; 4 males, 5 females). The same imaging procedure was performed in both the injured and control groups. Each participant read and signed an informed consent form approved by the governing university’s institutional review board.
Imaging
Patients lay prone on an examination table with their knee at 45° of flexion to bring the ST tendon more superficial and allow better imaging with ultrasound (Figure 1). The patient's involved tendon was palpated and imaged to confirm it was indeed the ST tendon. Using real-time, b-mode ultrasound imaging, the ST tendon was traced to the muscle in the longitudinal plane. The ultrasound probe was rotated into the axial plane to confirm the muscle to which the tendon was attached (Figure 2). The probe was returned to the longitudinal plane, and the patient contracted his or her hamstring to verify the regrown tendon was attached, that is, there was motion of the tendon during contraction. A mark was placed on the skin’s surface at the location of the ST tendon, and the process was repeated for the contralateral side.

Setup for the collection of shear waves propagating through the tendon. The examination table was elevated to bring the knee to a 45° knee flexion angle. Note: The actuator is proximal to the transducer so the shear waves travel from origin to insertion.
Longitudinal view of (A) the semitendinosus (ST) tendon and (B) axial view of the ST muscle. The ST tendon and muscles are traced in red.
cSWE was performed on both the involved and uninvolved ST tendons. The cSWE method used to determine viscoelastic properties of the ST tendon has been described by Cortes et al. 4 cSWE requires a mechanical stimulus to be applied to the tissue of interest and a high–frame rate ultrasound unit to collect the raw radiofrequency (RF) data. Data were then postprocessed using a custom Matlab signal transformation and analysis code. An ultrasound unit (Ultrasonix MRP) with an attached 128-channel data acquisition unit (DAQ) (Analogic) collected the RF data at 6450 Hz. The DAQ system allowed single lines of RF data from each element to be collected. A 38-mm-wide, L14-5/38 probe with a 0.29-mm spacing between piezoelectric elements was used in the data collection. Shear waves were applied to the tendon by means of a Bruel & Kjaer 4810 mechanical actuator (Bruel & Kjaer). The ultrasound probe was placed approximately 2 cm proximal to the knee joint along the ST tendon, and the actuator was placed 3 cm proximal to the transducer (Figure 1). The transducer was set to produce a mechanical impulse along the tendon at 323 Hz. A dataset of more than 60 frames was collected. Five additional sets of data were collected at 340, 358, 379, 403, and 430 Hz, with the transducer and actuator held in a fixed position.
Data Management and Analysis
Postprocessing signal analysis yielded the mean shear wave speeds for each frequency. Postprocessing included a Fourier transform of the signal to calculate the signal phase. The difference in phase of the shear wave across the length of the transducer allowed for the speed of the wave to be calculated. A Voigt model was used as the minimization criteria of an optimization algorithm to determine the viscoelastic properties by relating the shear speed to frequency,

where the shear modulus is represented by µ 1 (kPa) and the viscosity modulus by µ 2 (Pa·s), which will be reported as the ratio of involved to uninvolved moduli for regrowth assessment. V s is the shear wave speed, ω is the shear wave frequency, and ρ is the tissue density of 1600 kg/m3 for tendon. 11
A 2-tailed paired t test determined differences between the involved and contralateral tendons (P < .05) for both viscoelastic moduli. The same t test was performed for the control participants, using the left and the right as matched-pair comparisons. A Pearson correlation coefficient determined the relationship of the viscoelastic moduli to recovery time postoperatively. An interclass correlation coefficient ICC(3, 1) was used to determine the reliability of the measurement. A post hoc power analysis was performed using G*Power 3.1.10 software (Franz Faul). It was found that there were sufficient patients to power the study (power >0.95). An ICC(3, 1) equal to 0.90 was determined from the postprocessing output, establishing cSWE as a repeatable measure within the ST tendon. The injured group was also analyzed as 2 groups: greater and less than or equal to 12 months postoperatively.
Results
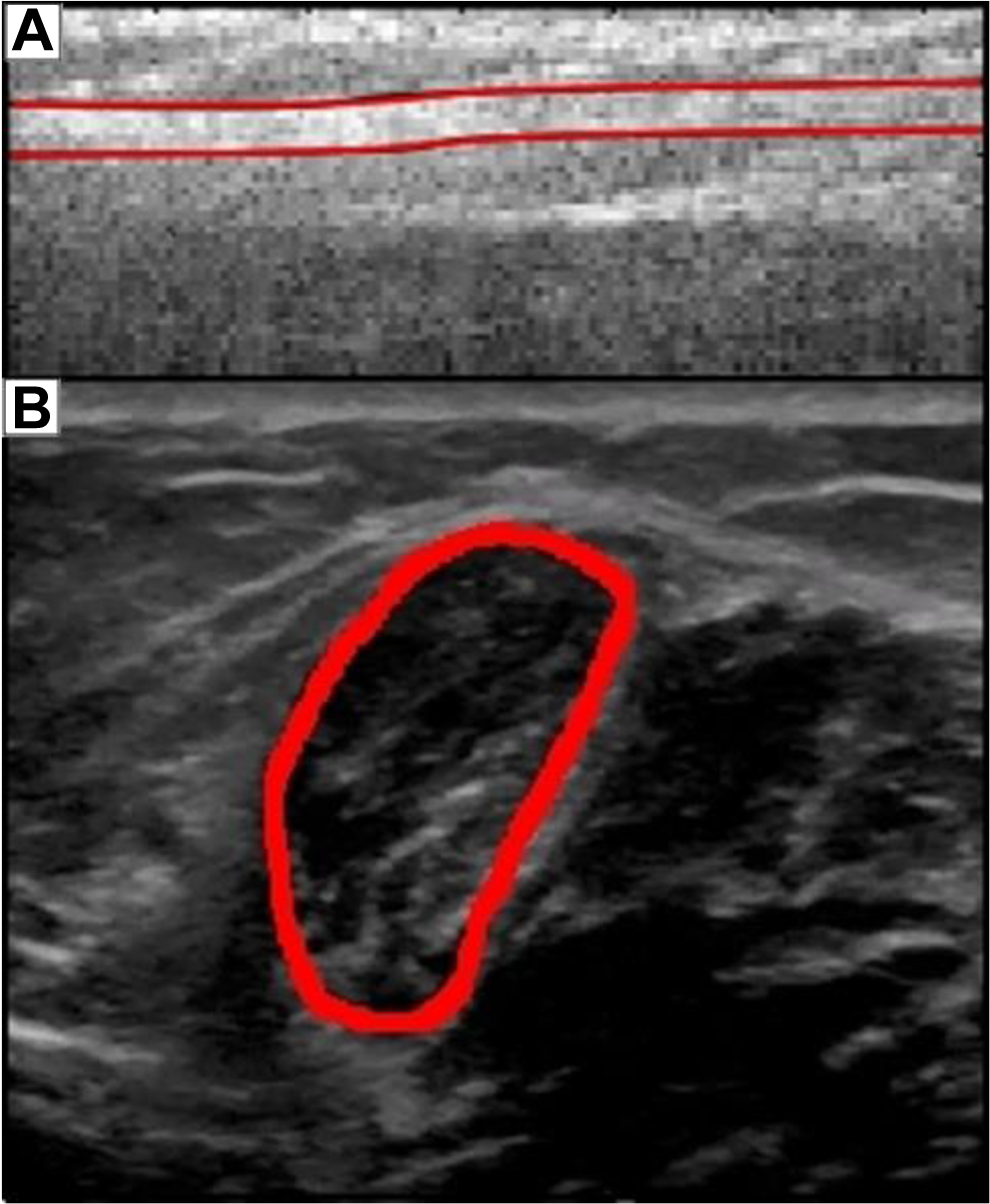
Thirteen patients were analyzed for ST regrowth 6 to 24 months post-ACLR (mean time post-ACLR, 13.2 ± 5.8 months). Twelve of 13 patients (92%) had ST regrowth that was visualized by b-mode ultrasound. Marked differences were visually apparent between involved and uninvolved tendons via ultrasound (Figure 3).

Ultrasound images of (A) the regenerating (involved) semitendinosus (ST) tendon and (B) the uninvolved ST tendon from a single patient, 14 months postoperative. Note the wavier, disorganized layout of the ST tendon on the involved limb compared with the uninvolved limb, though the involved limb appears to be thicker than the uninvolved.
The cSWE protocol produced shear and viscosity moduli maps for each of the tendons, of which an average was taken over the entire region of interest to report a single value for each tendon (Figure 4). The mean shear modulus of the uninvolved ST tendon was 129.4 ± 55.3 kPa and the average viscosity modulus was 192.6 ± 80.9 Pa·s, while that of the involved side was 73.0 ± 16.7 kPa and 114.3 ± 22.2 Pa·s, respectively. A significant difference between the involved and uninvolved limbs existed for the shear modulus (P = .004; 95% CI, 27.51-95.01) and the viscosity modulus (P = .007; 95% CI, 34.16-135.16) (Table 1). The mean shear modulus recovery was 56.4% of the uninvolved tendon, and the viscosity modulus recovered a mean of 59.4%. The improvement of the tendons’ shear modulus, demonstrated by the involved to uninvolved modulus ratio, had a strong positive correlation with time (r = 0.60, P = .039). The improvement in viscosity with regard to symmetry also yielded a positive correlation, though it did not reach significance (r = nonsignificant, P = .208) (Figure 5). The shear modulus value of the involved side was a mean 39.9% of the uninvolved leg in those within 12 months of ACLR and 80.6% in those 12 to 24 months post-ACLR. Similarly, the viscosity modulus of the involved side was a mean 46.0% of the uninvolved leg in those within 12 months of ACLR and 78.7% in those 12 to 24 months after ACLR. Height and weight had no significant effect on viscoelastic parameter recovery. The data for the uninjured comparison group showed no significant side-to-side difference in μ 1 or μ 2 (P = .875 and P = .779, respectively) (Table 1).

Raw ultrasound data for a single patient. The uninvolved tendon (A, B, C) with no overlay (A), the shear modulus map overlay (B), and viscosity modulus map overlay (C). The involved tendon (D, E, F) with no overlay (D), the shear modulus map overlay (E), and viscosity modulus map overlay (F). Note the lower viscoelastic properties for the involved side.
Mean Shear Modulus (µ 1) and Viscosity Modulus (µ 2) of the Involved and Uninvolved Semitendinosus Tendons a

a Given there is no involved side for the healthy controls, the right side is listed as the uninvolved side. Note the greater than 40% improvement in shear modulus from less than 12 months to greater than 12 months. *Since there is no operation in the healthy group, there is no data for time postsurgery to report. Inv, involved; ST, semitendinosus; UnInv, uninvolved.
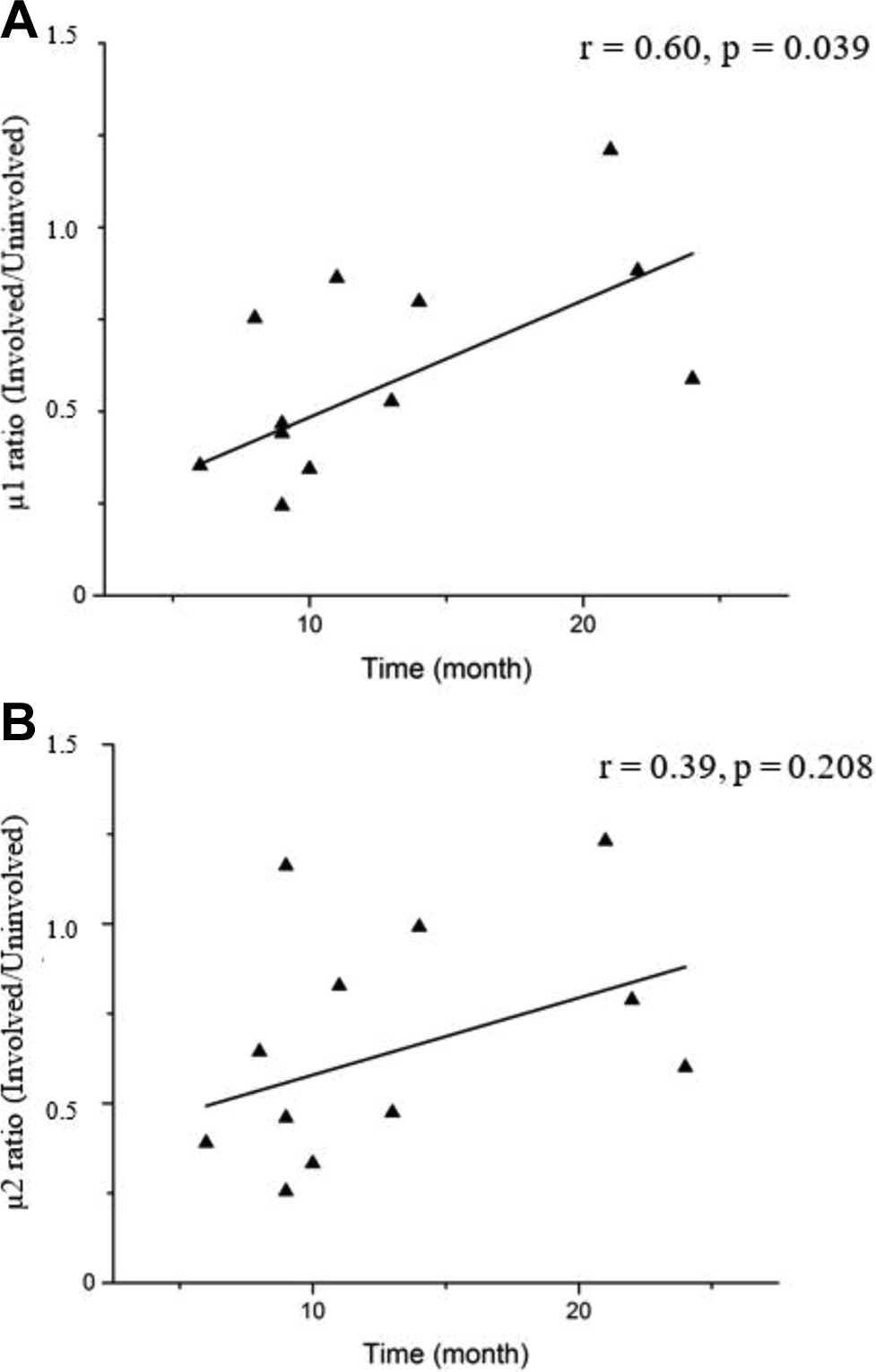
Correlation between the (A) shear and (B) viscosity moduli symmetry and time in months. Note the positive correlation, indicating improvement in the viscoelastic properties with time postoperative.
Discussion
There was evidence of regrowth of the ST in 92% of patients after harvesting STG autograft for ACLR. There was a significant difference between the shear and viscosity moduli of the involved and uninvolved tendons in the entire sample (Figures 3 and 4) as well as a positive correlation between time post-ACLR and the bilateral difference of the tendons’ shear moduli. Our hypothesis that a significant difference in mechanical properties between the involved and uninvolved sides was confirmed. The hypothesis of the mechanical property symmetry being correlated with time was also confirmed.
An increase in the shear modulus will enable the muscle to contribute to joint torque with time. The improved viscosity modulus appears to be less associated with patient recovery time across patients (r = 0.39), but the correlation is still positive. The recovery of these mechanical properties indicates the possibility of restoring the ST muscle-tendon complex function after ACL autograft reconstruction with an ST tendon.
The understanding and evaluation of the shear modulus is essential for determining the potential strength contributions of the ST muscle. In vitro, the shear modulus is linearly related to the elastic modulus. 5 If the shear modulus is linearly related to the elastic modulus and the shear modulus is correlated to postoperative recovery time, the elastic modulus will be correlated with time as well. Given that the healthy control group demonstrated no significant differences in viscoelastic properties bilaterally, the increase in ST tendons shear modulus with time postoperative in the ACLR group implies a possible recovery of the elastic modulus to the levels of symmetry of healthy controls. Recovery of the elastic modulus is important in restoring joint torque as it allows the muscle to pass force across the joint and contribute to knee torque. The elastic modulus is a direct measure of the amount of energy absorbed by the tendon during a contraction. The amount of energy lost to tendon stretch is energy that is not transmitted across the joint and can manifest as lower torque. The mechanical property contribution to joint torque may explain the findings of Janssen et al, 12 which showed the visual presence of the ST tendon, via ultrasound, 12 months postoperative does not correlate to a recovery of isokinetic hamstring strength. The present study demonstrated that only 39.9% of ST tendon elasticity had recovered by 12 months postoperative (Table 1). An increased elastic modulus causes the tendon to be stiffer and have less deformation when a force is applied. The reduced elasticity of the tendon results in more energy lost to tendon stretch during contraction, creating a torque deficit at the joint. It may be that hamstring regrowth is linked to strength recovery, but the true determining value is the mechanical property recovery and not the visual presence or apparent structure of the tendon. The involved tendons’ viscosity being only 46.0% of the uninvolved tendon may not affect the isokinetic hamstring strength but it would be integral to preventing reinjury. Given that viscosity is the stiffness of a material at a given rate of deformation, with rapid perturbation, increased viscosity would cause increased stiffness, aiding in the protection of the joint through greater ST muscle strength.
The mechanisms responsible for the time correlation to viscoelastic recovery are important to understanding recovery of optimal performance. The tendon has a disorganized structure consisting of more type 3 collagen than the stronger type 1 collagen in the initial stages of tendon healing after rupture. 2,6 The tendon becomes stronger with rehabilitation and the type 1 collagen replaces the type 3 collagen. It has been shown that the regrowth and reorganization stem from mechanical forces being placed on the tissue. 25 This is supported by tendon rehabilitation, which shows that early function, while the tendon is composed of this disorganized collagen mass, produces the best outcomes. 13 The viscoelastic property recovery is correlated with time postsurgery. The tendon not only needs time to regrow but also needs to be placed under tension to facilitate faster reorganization. The use of b-mode ultrasound can detect the presence of the tendon during rehabilitation, and elastography can determine whether the tendon's mechanical properties have started recovering. This information can be used to determine the best exercise regimen to facilitate tendon healing.
This is the first time the mechanical properties of the ST tendon have been demonstrated in vivo and provides an understanding of what is filling the tendon gap postresection. Knowing the tendon gap recovers tendinous material, which, on average, has regained less than half of its stiffness within a year, indicates that a longer recovery time is necessary after ACLR. This would permit the medial ST hamstring muscle to begin contributing torque across the knee and add protection to the reconstructed ACL, as the ST muscle contributes to resisting anterior tibial translation.
The patient population was collected from a number of different surgeons who did not report surgical technique. A variety of graft harvest techniques exist for the semitendinosus that can affect regeneration of the tendon. Transecting the distal end of the graft at the periosteum produced a regrowth rate of 82%, 18 while leaving a 4-cm distal stump led to a 100% regrowth rate. 9 This study sample size was not large enough to use each surgeon as a separate factor for regrowth rate. There was 1 surgeon in this study from which the majority of patients were recruited (6/13). The surgeon performs a technique that is intended to promote tendon regrowth. The GRA and ST tendons are freed from the original tendon attachment for 10 cm up the thigh to assure ease of stripping without preventing graft resection. The ST tendon sheath (synovial membrane surrounding the tendon) is entered, and an open stripper is placed around the tendon. The stripper travels proximally until the tendon is released from the muscle. The sheath is then closed using sutures, leaving a path for tendon regeneration. This technique yielded a 100% regrowth rate in this study. There have been no reports regarding the influence of graft harvest technique on tendon structure reorganization or mechanical property recovery rate, which may be of interest during future mechanical property testing, including cSWE.
This study has the limitation of including only participants from a single time point within a high school and college competitive age range. To increase generalizability, a longitudinal study of patients from a wider range of ages is needed. While the age range was limited, the results are comparable to other studies demonstrating regrowth over a larger age range. 20 This would indicate that the return of mechanical properties would also progress similarly in a broader age demographic. The graft harvesting technique of the surgeon performing the ACLR determines the effectiveness of the ST tendon regrowth, and it is unknown whether it affects the regrowth rate. Additionally, variation in rehabilitation protocol and sports activity were not controlled. The differences in rehabilitation protocols and postrehabilitation exercise programs may have caused the tendon to reorganize differently depending on the stresses put on the tendon during regrowth. There may have been changes of the ST tendon on the contralateral limb in addition to the involved side, although the values seen in the contralateral side were similar to those of controls (Table 1). It is also necessary to note that the recovery of the tendon's mechanical properties does not guarantee the recovery of torque production. If the muscle of the resected tendon retracts postoperatively and is not stretched by the recovering tendon, only a minimal amount of force-generating potential would exist in that muscle-tendon complex.
This study showed that the majority of patients regrew their tendon, which then proceeded to recover bilateral mechanical properties that were associated with time after surgery. Viscoelastic properties were substantially more symmetrical in the second postoperative year.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: The research reported in this publication was supported by the National Institute of General Medical Sciences and by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under grants R01-HD087459, P20-GM103333, U54-GM104941, and R21-AR067390.
Ethical approval for this study was obtained from the University of Delaware Institutional Review Board (study 373521-6).