
Abstract
Background:
Elbow capsular release can be performed arthroscopically or through an open method to improve range of motion (ROM). However, it is unclear how frequently patients require an open capsular release after unsatisfactory results from an arthroscopic release.
Purpose/Hypothesis:
The purpose of this study was to determine the percentage of patients who underwent an arthroscopic elbow release for loss of motion who then required a repeat elbow capsular release or other subsequent surgery on the same elbow. It was hypothesized that patients who underwent arthroscopic elbow release would rarely (<5%) require a subsequent elbow release.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent arthroscopic elbow capsular release from January 1, 2010, to December 31, 2019, were identified by chart review and procedure code. Demographic parameters, pre- and postoperative ROM, and surgical history were collected by chart review. Follow-up data included patient satisfaction and the Timmerman-Andrews (TA) elbow score. Data were compared between patients who did and those who did not require subsequent elbow surgery.
Results:
Overall, of 140 study patients (116 male, 24 female; mean age, 49.6 years), 18 (12.9%) required subsequent surgery, including 6 capsular releases (4.3%; 1 open and 5 arthroscopic). The most common follow-up procedure was ulnar nerve releases/transpositions (n = 7). Total arc of elbow motion (flexion to extension) improved by a mean of 51.4°. The mean TA score was 76.5 ± 20.4 at a mean of 5.25 years postoperatively. Mean satisfaction score was 77.6 ± 26.3. In this study, 82.4% of patients stated that their symptoms either improved or resolved completely. Patients who required subsequent surgery had a significantly lower preoperative total arc of elbow motion versus those who did not require subsequent surgery (P = .046). There was no difference between the groups in symptom resolution, satisfaction, ROM, or TA score (P ≥ .279 for all).
Conclusion:
After arthroscopic elbow release, <5% of patients required a repeat elbow capsular release, 12.9% required some form of follow-up elbow surgery, and 4.3% had a new injury of the elbow. Overall, patients saw improvement in elbow ROM, but many still had residual symptoms from their underlying disease after arthroscopic elbow capsular release.
Elbow range of motion (ROM) is imperative to daily function; however, elbow stiffness is a common complaint after elbow trauma or throwing sports such as baseball. 4,11 Magermans et al 5 determined the minimum elbow ROM needed for activities of daily living as 30° to 130°. However, there are patients who do not tolerate loss of elbow motion well as they have a difficult time exercising and working. In patients who have symptomatic loss of motion of the elbow and do not respond to conservative treatments such as physical therapy or mobilization braces, 6 surgical elbow capsular release is often indicated.
Elbow release can be performed arthroscopically or through an open approach. The arthroscopic approach involves several small portals that allow access to the anterior and posterior compartments of the elbow without the need for a large incision. 7 The open approach can be performed from either the medial or lateral side of the elbow or both and involves a larger incision with more extensive soft tissue manipulation. 7 The goal of both procedures is to remove bony impingement anteriorly and posteriorly and to release/remove the capsule of the elbow, which is often constricted. A comparison of the arthroscopic and open techniques by Cohen et al 3 showed that arthroscopic release provides greater pain relief, while open release results in greater improvement in ROM. However, it remains unclear how frequently the arthroscopic approach provides unsatisfactory results, thus leading to the necessity of a future open capsular release or repeat arthroscopic capsular release.
The purpose of this study was to determine how frequently patients who underwent an arthroscopic elbow release for loss of motion required a repeat elbow release (open or arthroscopic) or other subsequent surgery on the same elbow in the future. It was hypothesized that patients who underwent arthroscopic elbow release would rarely (<5%) require a repeat elbow release on the same elbow.
Methods
This is a retrospective analysis of all patients who underwent an arthroscopic elbow capsular release at 1 institution from January 1, 2010, to December 31, 2019. Patients were indicated for this procedure because of elbow stiffness impacting their quality of life. This study was approved by the corresponding Institutional Review Board (Approval number 21E.547). Patients were excluded from this study for any previous surgery on the ipsilateral elbow and an age <18 years at the time of surgery. Patients were identified based on current procedural technology codes 29834, 29835, 29837, 29838, and 24300, and surgical procedure was confirmed by chart review. Preoperative demographics (age, sex), indications for surgical intervention (osteoarthritis [OA], elbow contracture, etc), preoperative elbow ROM, and postoperative elbow ROM (using most recent noninjured follow-up) were collected via chart review. Chart review was also performed on included patients to determine who had a subsequent procedure on the ipsilateral elbow. In addition, patients were contacted via RedCap surveys to determine whether any subsequent elbow surgeries occurred at another institution and to answer patient-reported outcome surveys. Postoperative elbow functional capacity was assessed using the Timmerman-Andrews (TA) score, which contains a subjective component (pain, swelling, locking/catching, and activities) and an objective component (flexion contracture, pronation/supination, and sagittal arc of motion). Given that the ROM data for the objective component was not collected at the same follow-up time as the subjective component, the subjective TA score is used in this study, with outcomes classified as poor (<60), fair (60-79), good (80-89), or excellent (90-100). 13 Satisfaction was scored on a scale of 0 to 100, with a score of 100 indicating complete satisfaction.
All procedures were performed under a tourniquet, with a regional block of the brachial plexus and the patient placed in the lateral decubitus position. Capsulectomy was performed with an electric shaver, excising the capsule from proximal to distal and from medial to lateral until the brachialis muscle fibers were fully visible. Soft tissue was elevated off the humerus anteriorly and posteriorly. Manipulation was performed once all soft tissues were released. Postoperative care included the arm being placed in a sling for 2 weeks, prescription of indomethacin for prophylaxis against heterotopic ossification and some painkillers to take as needed, and the recommendation of physical therapy starting the day after surgery. Patients continued physical therapy for 2 to 3 months and followed up in the office at 2 weeks, 6 weeks, and 3 months after surgery. The primary outcome of this study was a repeat elbow capsular release, which can be performed in an open or arthroscopic manner. The decision of what technique to use for this procedure was made with a patient-centered approach in a discussion between the patient and the physician. Therefore, repeat elbow capsular release will be reported as a single outcome regardless of whether this was done through an open or arthroscopic approach.
Statistical Analysis
Comparison of postoperative outcomes between patients who did and did not undergo subsequent elbow surgery was performed via t test for parametric continuous data and Mann-Whitney tests for nonparametric continuous data. Chi-square or Fisher exact test was used to compare categorical data. P <.05 were deemed statistically significant. Statistical analysis was performed using R studio (Version 3.6.3).
Results
Overall, 161 arthroscopic elbow capsular release patients were identified via chart review; of these 161 patients, 3 declined to participate and 18 were unable to be contacted. Thus, 140 patients (87%) were included in the final analysis (116 male, 24 female; mean age at surgery, 49.6 ± 13.6 years). Among the 140 patients, 69 (49.3%) responded to the follow-up survey, which provided additional data including the subjective TA score (Figure 1).
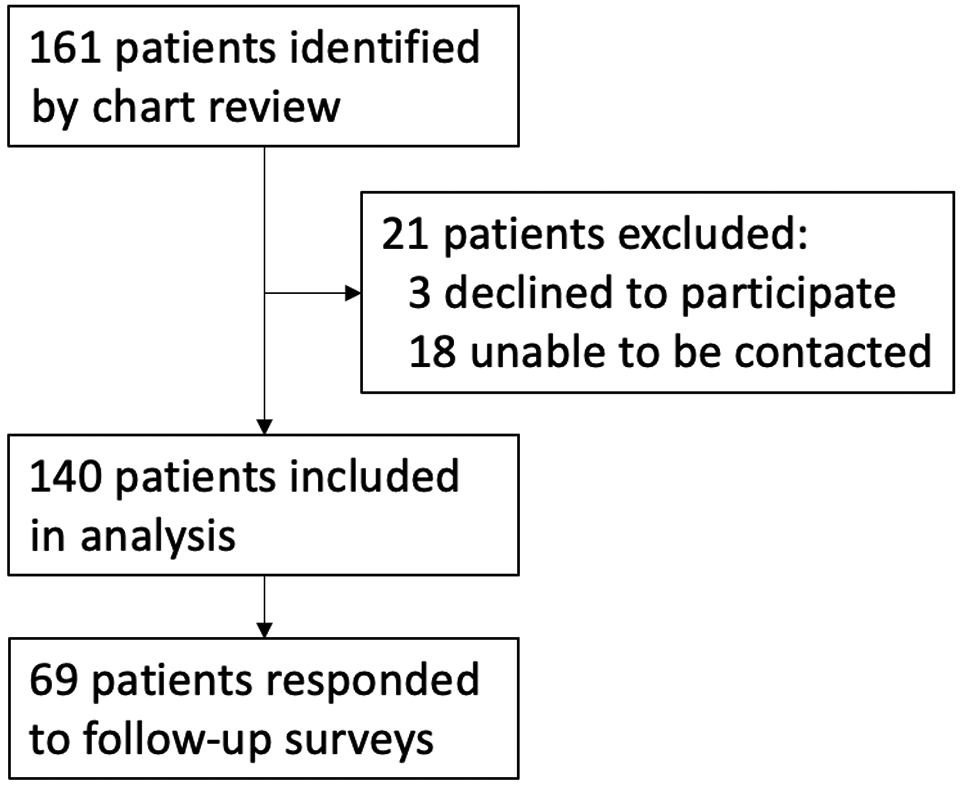
Flowchart of patient inclusion/exclusion.
Of the 140 patients, 36 (25.7%) were self-described athletes before the index procedure. Associated diagnoses for the 140 patients undergoing arthroscopic elbow capsular release included capsular contracture from OA (n = 118), loose body formation (n = 73), nonsport-related trauma (n = 18), ulnar neuropathy (n = 14), osteophyte formation (n = 13), inflammatory or rheumatoid arthritis (n = 9), radial head fracture (n = 8), cubital tunnel syndrome (n = 6), synovitis (n = 5), lateral epicondylitis (n = 4), osteochondritis dissecans (OCD) of the capitellum (n = 3), sport-related trauma (n = 2), joint effusion (n = 2), synovial chondromatosis (n = 2), and scarring/plica formation (n = 1), with patients often having a combination of diagnoses. Mean preoperative arc of motion (flexion to extension) was 84.8° ± 40.5°. Mean preoperative pronation was 81.2° ± 16.3°, and mean preoperative supination was 78.9° ± 18.3°. Patients underwent an average of 3.28 weeks of preoperative physical therapy before surgery.
Postoperative ROM measurements were collected at an average 87.4 days after surgery (range, 58-185 days). Postoperative mean total arc of motion was 134°± 21.6°, which was a significant improvement (P < .001). Patients averaged an improvement of 51.4° ± 44.9° in total arc of motion from before to after surgery. Mean postoperative pronation was 85.6° ± 9.5°, and mean postoperative supination was 85.0° ± 10.4°, both of which were significant improvements (P < .001). Pronation and supination achieved an average improvement of 4.4° and 6.1°, respectively.
Of the 140 patients, 18 (12.9%) had follow-up elbow surgery, including 6 repeat open or arthroscopic capsular releases (4.3%; 1 open and 5 repeat arthroscopic procedures). Other follow-up procedures included 7 ulnar nerve releases/transpositions, 2 lateral collateral ligament repairs, 2 loose body removals, and 1 bursectomy. Of the patients who required a subsequent procedure, 4 were participating in sports before the initial arthroscopic elbow capsular release, and 14 were not participating in sports. There was no significant difference between the patients who did and did not have subsequent elbow surgery regarding the percentage of patients who reported that their symptoms improved (46.2% vs 60.0%, respectively) or whose symptoms completely resolved (23.1% vs 25.5%, respectively) at final follow-up (P = .46). Of the patients who had subsequent surgery, 38.5% achieved subjective full postoperative ROM, which was not significantly different from patients who did not have a follow-up surgery (48.1%, P = .467). Table 1 shows a comparison of preoperative ROM data, postoperative ROM data, TA score, and satisfaction score for patients who did and did not have a subsequent elbow surgery.
Comparison of Preoperative and Postoperative Clinical Data Between Groups According to the Need for Subsequent Elbow Surgery a

a Data are shown as mean ± SD. Boldface P value indicates statistically significant difference between groups (P < .05). TA, Timmerman-Andrews.
At an average of 5.3 years postoperatively (range, 1.1-10.8 years), 69 patients responded to the follow-up surveys. The mean postoperative subjective TA score was 76.5 ± 20.4 (range, 20-100) (Figure 2), with scores classified as poor in 13 patients, fair in 17 patients, good in 18 patients, and excellent in 24 patients. Most patients (82.4%) stated that their symptoms either improved or resolved completely, while 7.3% felt no change in symptoms, and 10.3% felt that their symptoms worsened; 6 patients (4.3%) sought treatment for new elbow diagnoses at a mean of 16.4 ± 18.2 months after the index arthroscopic release surgery. The injuries included cubital tunnel syndrome (n = 2), progression of OA (n = 2), elbow fracture (n = 1), and medial epicondylitis/golfer’s elbow (n = 1). Among athletes, 23 (63.9%) were able to return to sport at a mean of 4.5 ± 5.0 months (range, 0.5-24 months) after surgery: 6 patients (26.1%) returned at a lower level, 15 (65.2%) at the same level, and 2 (8.7%) at a higher level of sport. The mean satisfaction score was 77.6 ± 26.3.
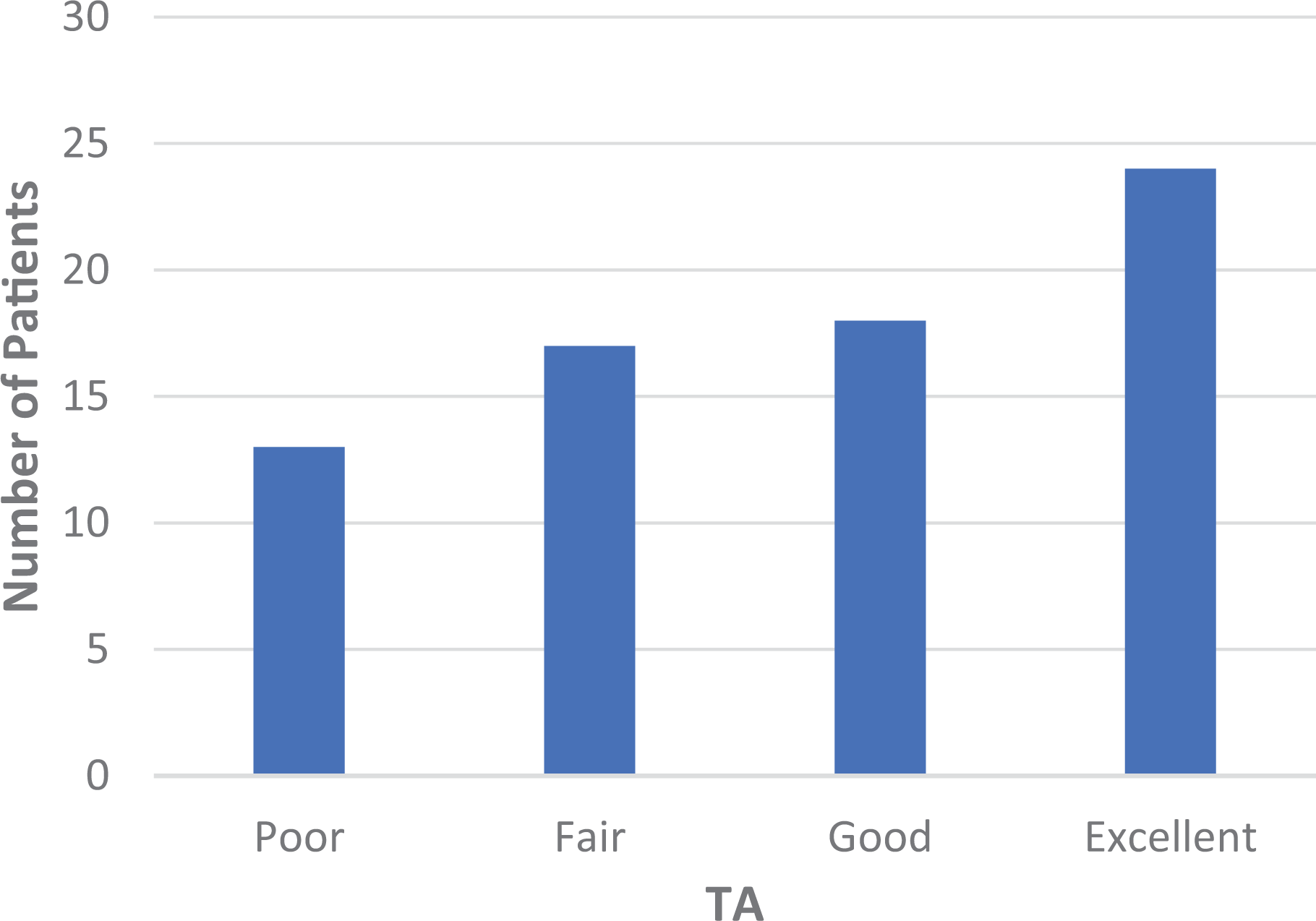
Distribution of subjective TA scores among the study cohort. Poor, <60; fair, 60-79; good, 80-89; excellent, 90-100. TA, Timmerman-Andrews.
The 13 patients with TA scores classified as poor had a preoperative pronation of 74.2° ± 24.7°, preoperative supination of 75° ± 22.8°, and preoperative arc of motion of 80° ± 23.0°. Postoperative pronation was 80.8 ± 14.4, postoperative supination was 76.3° ± 18.5°, postoperative arc of motion was 129.4°± 20.2°. Improvement in arc of motion was 49.4° ± 30.2°. A total of 3 of 13 patients had follow-up elbow surgeries. There was no significant difference in preoperative ROM, postoperative ROM, or improvement in ROM between patients with poor TA scores versus those with fair, good, or excellent scores (P ≥ .134); 3 of 13 (23.1%) patients with poor scores had follow-up elbow surgeries, including 1 (7.7%) repeat capsular release.
All patients had a preoperative diagnosis of capsular contracture; 11 patients had isolated capsular contracture, with the remainder having a combination of diagnoses. A total of 28 patients had contracture without degenerative joint disease (DJD). A total of 105 patients had a preoperative diagnosis of DJD/OA of the elbow. Of these patients, 9 had isolated DJD/OA, with the remainder having a combination of diagnoses; 23 patients had DJD without contracture. There was no significant difference in preoperative ROM, postoperative ROM, improvement in ROM, or TA score between all patients with capsular contracture and all patients with DJD/OA. When comparing patients with contracture without DJD with patients with DJD without contracture, patients with capsular contracture had a significantly lower preoperative pronation (P = .040) and preoperative arc of motion (P = .022) than patients with DJD. A total of 12 patients with capsular contracture had subsequent elbow surgeries, including 5 repeat capsular releases. Similarly, 12 patients with DJD/OA had subsequent elbow surgeries, including 5 repeat capsular releases.
Of the 71 patients who did not respond to the survey, the associated diagnoses included capsular contracture (56 patients), DJD/OA (52 patients), loose bodies (29 patients), synovial chondromatosis (2 patients), osteophytes (4 patients), ulnar neuropathy (8 patients), cubital tunnel syndrome (3 patients), radial head fracture (4 patients), rheumatoid/inflammatory arthritis (2 patients), synovitis (2 patients), effusion (1 patient), OCD of the capitellum (2 patients), nonsport trauma (11 patients), and lateral epicondylitis (3 patients). There was no significant difference in preoperative or postoperative ROM data between these patients and patients who did complete the survey (P ≥ .252). Of the 71 patients who did not complete the survey, 4 (5.6%) had a follow-up elbow surgery (2 elbow capsular release [2.8%], 1 had a bursectomy [1.4%], and 1 had a nerve release [1.4%]).
Discussion
In this retrospective analysis of patients who underwent arthroscopic elbow capsular release, patients overall had improved outcomes after this procedure. Our hypothesis was confirmed, as 6 patients (4.3%) needed a repeat elbow capsular release.
The incidence of revision procedures after arthroscopic elbow capsular release found in this study is similar to the rate published in previous studies. A previous study by Sevimli et al 9 found that no patients required a follow-up elbow surgery at a mean of 28.4 months after arthroscopic capsular release. However, that study had a smaller sample size with 22 included patients, compared with the 140 patients in the present study, as well as a shorter follow-up duration (about 2.4 years compared with 5.3 years in the present study). A similar study of 10 arthroscopic elbow capsular release patients found that 2 required a revision arthroscopic release and 1 needed an open osteophyte removal. 12 The 7 subsequent ulnar nerve transpositions that were required in this cohort are interesting as ulnar neuritis is often present in patients who have elbow contractures. Improvements in ROM may sometimes exacerbate underlying ulnar nerve symptoms. Furthermore, ulnar nerve entrapment can also be the cause of an elbow contracture. 14 Hence, while these 7 subsequent surgeries were not performed to restore motion, these revisions may be been avoided if these patients underwent an open elbow release through a medial approach with a concomitant ulnar nerve transposition or if a concomitant ulnar nerve transposition was performed.
Although the postoperative mean subjective TA score in this study was classified as fair (76.5), the most frequent score classification at final follow-up for the patients in this study was excellent. Interestingly, this finding was not associated with subsequent elbow surgeries, as the distribution of patients with follow-up surgeries per TA score group was similar (3 patients with poor, 3 patients with fair, 4 patients with good, and 3 patients with excellent scores; 4 TA scores not available). In addition, the mean satisfaction score of 77.6 out of 100 is lower than that reported by Ball et al 1 of 8.4 out of 10. However, in the context of 82.4% of patients stating that their symptoms either improved or resolved completely, these findings reflect good overall outcomes after arthroscopic capsular release with room for improvement. The reality of an elbow release is that the joint is often no longer normal secondary to the disease pathology, so persistence of pain is common as the joint is still arthritic, although it moves better.
The improvement in postoperative arc of motion found in this study is similar to the amount of improvement reported by previous investigators, which tends to average around 50°. 1,7,8,10 The significant improvement in pronation and supination after arthroscopic capsular release found in this study has also been reported by other studies. 1,2,8,10 Schreiner et al 8 reported an improvement of 18% in pronation and supination after arthroscopic elbow capsular release, while the mean improvement of 4.4° (5.4%) pronation and 6.1° (7.7%) supination found in this study is lower than this reported value. This improvement can occur from the manipulation or removal of loose bodies.
The patients in this study who required subsequent elbow surgery after the initial arthroscopic capsular release had a significantly greater preoperative arc of motion than patients who did not require a subsequent surgery. This could be the result of concomitant pathology in these patients, as many of the follow-up procedures were focused on anatomic corrections such as nerve transpositions and loose body removals.
The low rate of subsequent surgeries supports the existing literature that shows arthroscopic elbow release to be a safe and effective method to improve elbow ROM. 2 Considering that arthroscopic elbow release has a lower complication rate than open elbow release, 3 the results of this study support the continued use of this procedure. Future studies that directly compare clinical outcomes between arthroscopic and open elbow capsular release both for athletes and nonathletes will further clarify the indications for these procedures.
Limitations
Limitations to this study include the retrospective, observational study design preventing certain factors such as surgical technique and rehabilitation protocol from being controlled. Follow-up outcomes were not able to be collected at the same postoperative duration, as patients had surgeries at various points throughout the 10-year study window. Furthermore, some office notes only reported total arc of motion so we could not separate improvements in flexion versus extension, and data on patients whose symptoms had improved versus resolved completely were grouped together. Also, the survey response rate limited the statistical power of the TA and satisfaction scores. The study also only evaluated ROM in the short term and had a significant loss to follow-up for TA scores. Furthermore, there was no stratification of results by occupation or sport.
Conclusion
After arthroscopic elbow release, <5% of patients required a repeat elbow capsular release, 12.9% required some form of follow-up elbow surgery, and 4.3% had a new injury of the elbow. Overall, patients have marked improvement in elbow ROM, but many still had residual symptoms from their underlying disease after arthroscopic elbow capsular release.
Footnotes
Final revision submitted April 15, 2023; accepted April 27, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.G.C. has received grant support from Arthrex and DJO. F.P.T. has received consulting fees from DePuy/Medical Device Business Services and hospitality payments from Smith+Nephew. B.J.E. has received grant support from Arthrex; education payments from Arthrex, Pinnacle, and Smith & Nephew; consulting fees from Arthrex and DePuy Synthes; nonconsulting fees from Arthrex; and hospitality payments from Linvatec. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Thomas Jefferson University (approval No. 21E.547).