
Abstract
Purpose
The aim of this study was to suggest treatment guidline for primary elbow OA with ulnar nerve neuropathy or high-grade stiffness by evaluating the effect of ulnar nerve decompression on the outcome of osteocapsular arthroplasty.
Methods
A total of 30 patients who underwent primary osteocapsular arthroplasty for elbow OA were retrospectively reviewed. The surgical outcomes were evaluated for pain score (visual analog scale; VAS), range of motion (ROM), and Mayo Elbow Performance Score (MEPS). The ulnar nerve decompression was performed for (1) ulnar nerve neuropathy, and (2) high-grade stiffness of flexion, defined as the flexion angle, is <90°. Patients were categorized into the two groups: ulnar nerve decompression group (UD group, n = 11) and the non-decompression group (Non-UD group, n = 19). The surgical outcome was compared between the groups.
Results
Primary elbow OA with cubital tunnel syndrome or high-grade stiffness showed comparable improvement in MEPS, VAS, and ROM arc at final follow-up in the UD group compared with the non-UD group (UD group vs. non-UD group: MEPS 85.91 vs 86.84, p-value = 0.824, VAS 1.46 vs 1.16, p-value = 0.588, ROM arc 108 vs 109, p-value = 0.949). Improvement in ROM arc at 2 years follow-up was significantly higher in UD group (UD group vs. non-UD group: ROM arc difference, 42 vs 14, p = 0.002).
Conclusion
Osteocapsular arthroplasty with ulnar nerve decompression for primary elbow OA with ulnar nerve neuropathy or high-grade stiffness provided improved motion arc and compatible clinical results.
Level of evidence
Level III, Retrospective comparative study
Keywords
Introduction
Although primary osteoarthritis (OA) of the elbow is rare as compared with OA of other joints, it is a common disorder in young to middle-aged athletes and heavy manual workers who use their upper extremities extensively. 1 Patients with elbow OA usually complain of pain, stiffness, and neurologic symptoms related to the ulnar nerve. For patients whose symptoms do not improve with nonoperative treatment, surgical osteocapsular arthroplasty is performed to relieve pain or to restore functional range of motion (ROM).2,3
In primary elbow OA, one of the main purposes of osteocapsular arthroplasty is recovery of ROM to a functional level, which is defined as 100 degrees of motion arc. 4 Both open and arthroscopic osteocapsular arthroplasty have been previously reported. 5 However, various pathomechanisms related to the stiffness in primary elbow OA have been determined, and studies regarding those mechanisms are relatively rare. Anatomically, the two main pathology to address the stiffness in primary OA are spur, and contracture of capsuloligamentous tissue. Treatment with osteocapsular arthroplasty involves targeting these structures. However, clinically, the extent of recovery of ROM is limited, although all these structures are released. To improve the outcome of ROM, more research is required.
The ulnar nerve has high risk of stretching after release of high-grade stiffness owing to tethering or increased intraneural pressure. 6 In addition, the ulnar nerve has less excursion in a contracted elbow and greater tension is expected with elbow flexion which suddenly increases after capsular release. Antuna et al. reported that ulno-humeral arthroplasty resulted in long-term symptoms of ulnar irritation after surgery in up to 33% of patients with severely stiff elbow. This irritation was caused by a combination of excessive nerve stretching and compression in a cubital tunnel that was narrowed when the elbow was flexed further. 7 Therefore, osteocapsular arthroplasty combined with prophylactic ulnar nerve decompression has been proposed. 3 Some authors have even advocated the use of a prophylactic ulnar nerve procedure (decompression or transposition) to reduce postoperative nerve symptoms.2,3,7,8 However, there are no guidelines on how to treat the ulnar nerve in procedures related to primary elbow OA. Therefore, the aim of this study was to suggest treatment guidline for primary elbow OA with ulnar nerve neuropathy or high-grade stiffness by evaluating the effect of ulnar nerve decompression on the outcome of osteocapsular arthroplasty. We hypothesized that osteocapsular arthroplasty with ulnar nerve decompression for ulnar nerve neuropathy or high stiffness elbow shows comparable improvement in clinical outcomes without ulnar nerve-related complications.
Materials and methods
Institutional review board approval was obtained prior to this study (Asan medical center IRB No. 2020-0176). Data from all patients who underwent primary elbow osteocapsular arthroplasty by a single surgeon, who had experience for more than 10 years in elbow surgery, for primary elbow OA between January 2010 and April 2019 at a tertiary university hospital were retrieved from the medical records and radiographic archives and retrospectively reviewed by two orthopedic surgeons (H.J.K., E.K.) with a blinded control. All patients were followed up for 3 weeks, 3 months, 6 months, 1 year, and 2 years after surgery. After the review of medical records from the database, 63 patients were collected.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) arthroscopic or open osteocapsular arthroplasty, (2) documentation of no previous trauma at the affected site, and (3) availability of medical information for follow-up. We excluded 33 patients with (1) follow-up loss (n = 25), (2) revision surgery (n = 3), (3) rheumatoid arthritis or infection (n = 3), (4) condition combined with burn injury (n = 1), and (5) congenital deformity of radial head dislocation (n = 1). After excluding those patients, 30 patients were eligible and provided consent for this study.
Indication of ulnar nerve decompression
Subgroup information of ulnar nerve decompression group (UD group) according to EMG/NCV, ulnar nerve, and demographic data.

UNSx: ulnar nerve symptoms; UN: ulnar neuropathy.
We divided the patients into two groups: ulnar nerve decompression group (UD group) and non-ulnar nerve decompression group (non-UD group) (Figure 1). Ulnar nerve decompression was performed by either transposition or in situ decompression. In open osteocapsular arthroplasty, we instituted ulnar nerve anterior transposition (n = 3), and in arthroscopic osteocapsular arthroplasty, we did mini-open in situ endoscopic decompression (n = 8) before the osteocapsular arthroplasty (Figure 2).7,9,10 Study design. The case (56 years old age, male) in ulnar decompression group, which got arthroscopic osteocapsular arthroplasty combined with in-situ ulnar decompression for stiff elbow with ulnar neuropathy confirmed by EMG/NCV. FC, flexion contracture; FF, further flexion; Preop., preoperative; Postop., postoperative; FCU, flexor carpi ulnaris.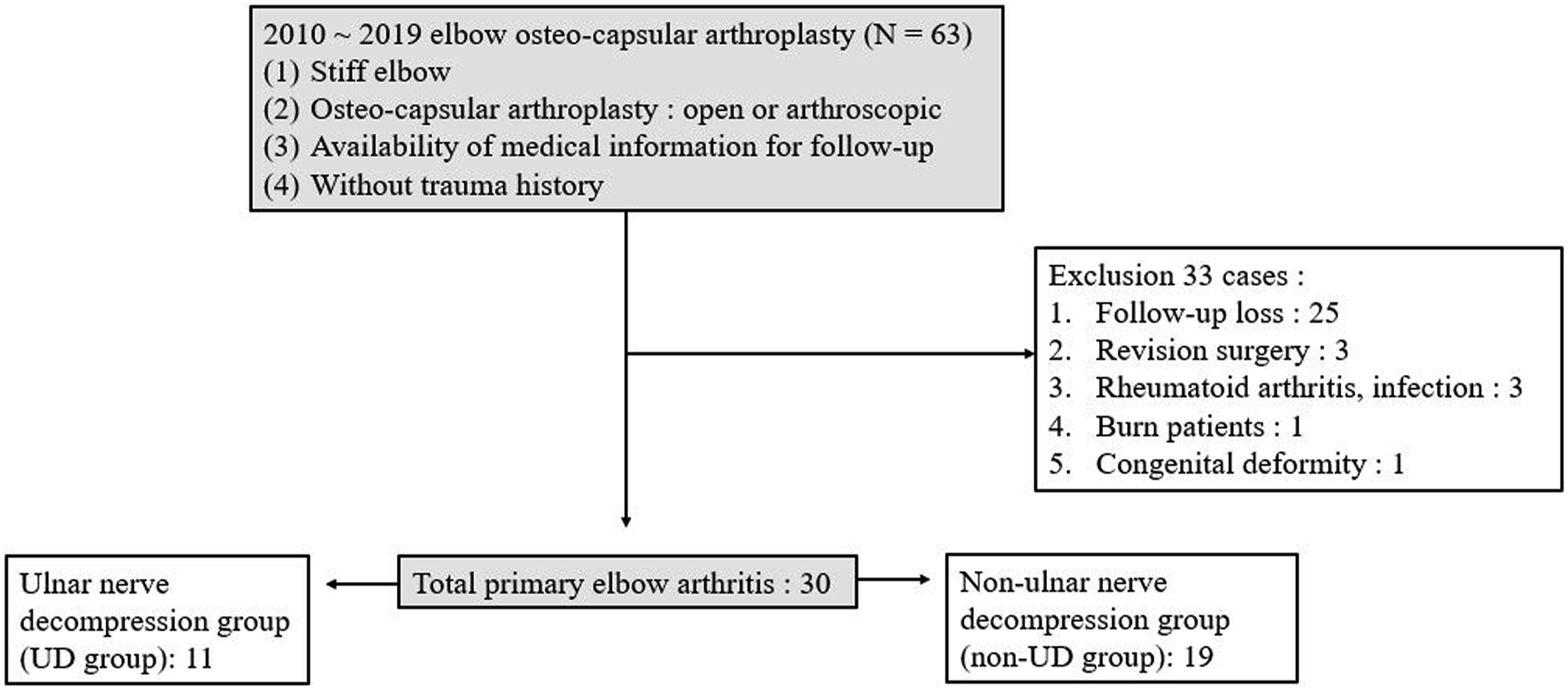

Assessment of clinical outcomes

Comparison of patient demographic characteristics between ulnar nerve decompression group (UD group) and non-ulnar nerve decompression group (non-UD group).

Preop.: preoperative; OP: operation; Arthro: arthroscopy; ROM: range of motion; VAS: visual analog score; MEPS: Mayo Elbow performance score.
* p < 0.05.
Pain score (VAS), ROM arc, missing ranges of improvement percentage (missing ROM, %), and MEPS were evaluated at four different time points: preoperatively and 3 months, 1 year, and 2 years postoperatively. Any patients who experienced aggravated preoperative ulnar nerve symptoms (sensory change, motor weakness, and 2 pinch distance) or had newly developed ulnar neuropathy at the final follow-up were recorded.
Radiographic assessment
To evaluate the preoperative radiographic severity of elbow OA between the two groups, preoperative CT images were graded according to Kwak’s CT-based staging system.11,12 All evaluations were assessed by two orthopedic surgeons (H.J.K., E.K.) through consensus. The CT-based classification comprised the following definitions for quantification of spurs and joint narrowing:
11
Stage 0: No involved fossa with intact joint space Stage 1: Unicompartmental involved fossa with intact joint space Stage 2: Bicompartmental involved fossa with intact joint space Stage 3: Joint space narrowing regardless of the state of the fossa
Statistical analyses
All statistical analyses were conducted using SPSS (version 21.0; IBM, Armonk, NY, USA). The 80% power was calculated under the assumption that the effect size was 1.203 in a total of 30 patients. The Kolmogorov–Smirnov normality test was conducted to assess the normality distribution. Dichotomous variables were compared by chi-square test and Fisher’s exact test. Nonparametric data of VAS and MEPS were compared between groups using a Mann–Whitney U test, and parametric data for ROM were compared using the Student t test. For multiple comparisons over four different time periods (preoperatively and 3 months, 1 year, and 2 years postoperatively) a repeated analysis of variance was performed and followed by Bonferroni post hoc analysis. All statistical tests were performed with a significance level of 0.05.
Results
Patients’ demographic details are summarized in Table 2. Eleven patients were included in UD group and 19 patients in non-UD group. The mean follow-up duration in each group was 48.3 and 45.9 months. The average ages of the patients in each group was 55.0 (SD, 5.7) and 54.1 (SD, 7.5) years.
There were no significant differences between the two groups in demography, except for preoperative further flexion angle (100 ± 16 in UD group and 112 ± 13 in non-UD group, p = 0.035) and preoperative ROM arc (70 ± 24 in UD group and 90 ± 16 in non-UD group, p = 0.014).
Ulnar nerve Decompression group
Flexion contracture angle and further flexion angle were significantly improved after surgery at final follow-up point (flexion contracture angle 27°–10°, p-value = 0.011; further flexion angle 90°–110°, p-value = 0.005). All other clinical outcomes, such as VAS, ROM arc, and MEPS improved after surgery, but did not show any statistically significance (VAS 5.18–3.34, p-value = 0.443; ROM arc 71–102, p-value = 0.075; MEPS 62.27–78.82, p-value = 0.126) (Figure 3). No postoperative ulnar nerve neuropathy has been reported. Ulnar nerve decompression without transposition was the main procedure performed in eight patients. Among these patients, preoperative ulnar nerve symptoms were reported in 3 patients with confirmation by EMG/NCV, and the other patients showed high-grade stiffness. Three patients had ulnar nerve anterior transposition and high-grade stiffness without any ulnar nerve symptoms or positive signs on EMG/NCV (Table 1). Outcome of primary osteoarthritis after surgery in ulnar nerve decompression group (UD) and non-ulnar nerve decompression group (non-UD). (*p < 0.05). VAS, visual analog scale; ROM, range of motion; MEPS, Mayo Elbow Performance Score.
Non-Ulnar nerve Decompression group
Comparison of outcomes between the two groups at final follow-up.
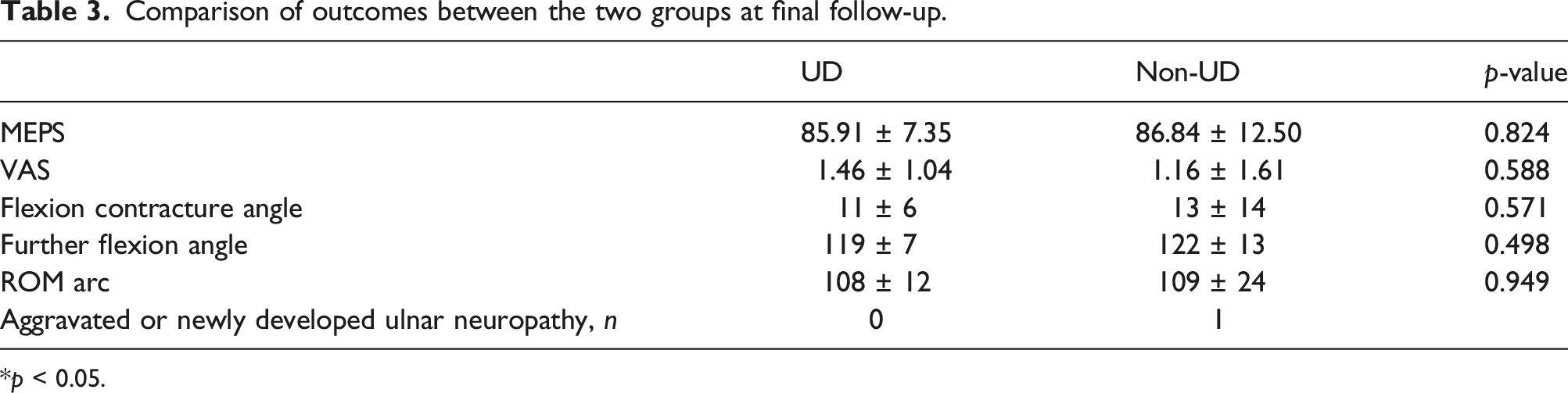
*p < 0.05.
Comparison of Clinical Outcomes between two groups
There was a significant difference in the changes of the following outcomes: flexion contracture angle difference, further flexion angle difference, ROM arc difference, and missing ROM between UD and non-UD groups (flexion contracture angle difference 20 vs 7, p = 0.014; further flexion angle difference 22 vs 7, p = 0.015; ROM arc difference 42 vs 14, p = 0.002; and relative ROM changes 51.67 vs 25.13, p = 0.023) (Figure 4). The trends of each outcome (ROM arc, VAS, and MEPS) during the follow-up are presented in Figure 5. There was no significant difference between the two groups at any time point. Comparison of the changes in outcome after surgery between the two groups at final follow-up (*p < 0.05). FC, flexion contracture; FF, further flexion; diff., difference. Comparison of the trends between the two groups regarding the outcomes in primary osteoarthritis: ROM, VAS, MEPS.

Discussion
Our study demonstrated that osteocapsular arthroplasty combined with ulnar nerve decompression for primary elbow OA with ulnar nerve neuropathy or high-grade stiffness resulted in greater motion arc gain without complications related to ulnar nerve. Furthermore, the clinical outcomes were comparable to non-ulnar nerve decompression group at 2-years follow-up.
Our current study has several important findings. First, osteocapsular arthroplasty for complicated elbow OA with ulnar nerve neuropathy or high-grade stiffness showed comparable clinical outcomes. In a systematic review of the surgical outcome of primary OA elbow, 5 1.2%–1.5% of ulnar nerve neuropathy occurred after osteocapsular arthroplasty. In addition, approximately 1.2%–4.2% patient undergo reoperation with ulnar decompression after osteocapsular arthroplasty. 13 Blonna et al. reported 11% incidence of delayed-onset ulnar neuritis after arthroscopic contracture release of the elbow. 13 Antuna et al. suggested that prophylactic ulnar nerve decompression or mobilization should be considered in patients with severe elbow ROM limitation. 7 Kwak et al. employed a similar concept and performed ulnar nerve decompression and transposition in patients with ulnar nerve neuropathy, ulnar nerve symptoms, or elbow flexion of <90°. 9 According to these previous studies, the clinical outcomes of osteocapsular arthroplasty for primary elbow OA combined with ulnar nerve neuropathy or severe contracture were unexpectable. However, based on the results of comparison in two groups, even more complicated cases showed compatible results. Therefore, it would be the basis for more aggressive application of osteocapsular arthroplasty in complicated elbow OA, if combined with ulnar nerve decompression.
Furthermore, we found that osteocapsular arthroplasty with ulnar nerve decompression improved ROM significantly based on both absolute difference and relative difference comparison. We found only one case of aggravation of ulnar neuropathy or newly developed ulnar neuropathy in non-UD group. Patients in UD group, they underwent an ulnar nerve-related procedure, did not experience any aggravated symptoms or complications related to ulnar nerve. UD group shows that all of the ROM measurements, including flexion contracture angle and further flexion angle, were improved in the postoperative period (Figure 2). However, the improvement in non-UD group was only in the ROM arc. The changes in ROM arc were more improved in UD group than in non-UD group (Figure 4). The missing ROM (%) changes were also evaluated to confirm the relative improvement of ROM after surgery. This important finding can be explained by the idea that, considering the ulnar nerve anatomical course 14 , gaining a greater angle of flexion after surgery could cause the ulnar nerve to be stretched and thus injured. Without ulnar nerve decompression, the patient can experience discomfort when attempting to achieve greater than usual flexion such as washing face or hair in daily activity, resulting in reduced flexion, although the patient may not have had any mechanical or soft-tissue tightness after surgery.
Lastly, with regard to the trends of outcomes, osteocapsular arthroplasty with ulnar nerve decompression (UD group) provided improved ROM arc, VAS, and MEPS according to clinical follow-up. (Figure 5). We could infer from these mid-term results that treatment of ulnar neuropathy provide more effective results in the long term. It is our impression that from limited excursion of the ulnar nerve, ulnar nerve can be caused by a slight increase in ROM, even after sufficient resolution of pathological factors and elimination of increased pressure of the cubital tunnel in elbow OA. As a result, function and pain could worsen over time.
The strength of our study is that it is the first to compare the clinical outcomes of ulnar nerve decompression with osteocapsular arthroplasty with those of without decompression group. According to previous studies, ulnar neuropathy is associated with the important pathology of primary elbow OA.15–17 Based on the findings of this study, we suggest that to improve the clinical outcomes and prognosis, especially ROM, in patients with primary elbow OA, treatment of the ulnar nerve should be considered. This recommendation can serve as an important treatment guideline for elbow OA.
Limitations
Several limitations should be considered. First, the study was performed using retrospective data collection and was not randomized. The ulnar nerve procedure was indicated (1) to avoid ulnar nerve event for a severe stiff elbow and (2) for definite ulnar nerve symptoms. We are aware that the nature of self-selection of this decision and retrospective nature of this study are prone to selection bias. Nevertheless, we believe that the rationale of performing ulnar nerve procedure is unavoidable considering the ethical reasons. Second, the proportion of patients lost to follow-up was relatively high, which may limit the extrapolation to bigger population. Third, our procedures for osteocapsular arthroplasty were mixed with open and arthroscopic methods. However, both groups showed no difference in the procedures, and main target pathologic lesion was similar in open and arthroscopic procedure. Lastly, only a mid-term follow-up evaluation was performed. Further studies are required to examine long-term outcomes and the clinical course.
Conclusion
Osteocapsular arthroplasty with ulnar nerve decompression for primary elbow OA with ulnar nerve neuropathy or high-grade stiffness provided improved motion arc and compatible clinical results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.