
Abstract
Background
Minimizing intra-articular bleeding and swelling is crucial in preventing the development of stiffness around the elbow. Tranexamic acid (TXA) has been shown to be an effective adjunct in reducing perioperative bleeding after surgery.
Purpose:
To determine the effect of intravenous (IV) TXA on postoperative drain tube output in arthroscopic osteocapsular release of the elbow for primary degenerative arthritis.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors performed a retrospective cohort study of 83 consecutive patients with primary degenerative elbow arthritis who underwent an arthroscopic osteocapsular release between 2015 and 2018. They organized patients into a no-TXA group (control) and a group that was given 1.0 g of IV TXA before tourniquet release. The primary outcome measure was drain tube output, and secondary outcome measures included postoperative day 1 pain levels on a visual analog scale and early range of motion at 8 weeks. Differences between groups were analyzed using 1-way analysis of variance, the Mann-Whitney U test, or the Fisher exact test.
Results:
There were 43 patients in the no-TXA group and 40 patients in the TXA group. Administration of IV TXA resulted in a 51% decrease in mean intra-articular bleeding for the TXA group, as measured via drain tube output (88.8 ± 80.5 mL [no-TXA] vs 43.4 ± 52.4 mL [TXA]; P = .0016). In both groups, there were significant increases in elbow arc of motion when compared with preoperative measurements. There were no between-group differences in early range of motion (129.7° ± 12.4° [no-TXA] vs 131.7° ± 9.2° [TXA]; P = .549) or postoperative pain (1.9 ± 2.2 [no-TXA] vs 1.5 ± 1.7 [TXA]; P = .89).
Conclusion:
In this study, IV TXA significantly reduced postoperative intra-articular bleeding in patients who underwent arthroscopic osteocapsular release of the elbow for primary degenerative arthritis. However, there were no differences in postoperative range of motion or pain between patients who received TXA and controls.
Keywords
Primary osteoarthritis of the elbow is a common cause of elbow pain and stiffness, particularly in men who engage in repetitive and strenuous activities, such as manual workers, farmers, or athletes. 13,16 Common presentations include loss of terminal extension and/or flexion with pain and irritability at the end ranges of motion. Patients can also exhibit sudden mechanical locking or a catching sensation from incarcerated loose bodies or frayed chondral flaps. 2 Midrange elbow pain is usually not a prominent feature, compared with end-range pain, as the hallmark of this condition is the development of impinging osteophytes arising from the olecranon tip and the corresponding olecranon fossa posteriorly and anteriorly from the coronoid process and anterior humerus. 2,16
With increasing societal demands and expectations for near full and/or pain-free elbow range of motion, any limitations short of this are often poorly tolerated by many patients. 13,22 When nonoperative management, such as analgesia and activity modifications, fails, arthroscopic surgical debridement and osteocapsular release of the elbow have been shown to be very effective and reliable in restoring range of motion, relieving pain, and improving quality of life in patients with mild to moderate disease. 2,13,16,18,22 The goals of surgery are to perform a synovectomy of all inflamed tissue, achieve capsular release, and remove any impinging osteophytes and loose bodies to alleviate the mechanical block to elbow motion. 2,16,21
However, it is equally important that after the osteocapsular release has been performed, all the gains that have been achieved in elbow motion are maintained, and any factors that would cause recurrent stiffness or intra-articular adhesions are minimized. Postoperatively, the development of joint stiffness occurs in 4 distinct phases, beginning with bleeding, followed by soft tissue edema and swelling, then granulation tissue formation, and eventually fibrosis. 6 As the first 2 phases occur immediately postoperatively, every attempt should be made to mitigate this, including early active motion, with or without continuous passive motion (CPM); cryotherapy; drain tubes to reduce hemarthrosis; nonsteroidal anti-inflammatory medications; perioperative corticosteroids; and compression bandages. 6,10,25
Tranexamic acid (TXA), a lysine-based inhibitor of plasminogen, has become increasingly popular in both general and orthopaedic surgeries as an effective agent that decreases bleeding in a variety of settings. 1,4,12 It works by blocking the progression of the fibrinolytic pathway by competitively inhibiting the activation of plasminogen to plasmin, therefore promoting clot formation. 1,12 In hip, knee, and shoulder arthroplasty, it has become well established from multiple randomized controlled trials that TXA reduces intraoperative bleeding, postoperative drain tube outputs, and blood transfusion requirements. 4,5,8,17 In elbow surgery, the evidence is still limited, with only 2 studies reporting on the role of TXA. 19,24 Recently, Zhang et al 24 demonstrated that topical TXA significantly decreases intraoperative blood loss and drain tube output after open arthrolysis for posttraumatic elbow stiffness, whereas Mannan et al 19 reported that perioperative blood loss was significantly less with TXA administration after total elbow arthroplasty. However, to date, no studies have investigated the role of TXA in arthroscopic elbow surgery.
The primary aim of this study was to determine the role of intravenous (IV) TXA in reducing postoperative hemarthrosis after arthroscopic osteocapsular release for primary degenerative arthritis of the elbow. Secondary outcome measures included postoperative pain levels and early range of motion. We hypothesized that TXA would significantly reduce postoperative hemarthrosis and drain tube output, leading to less pain and better early range of motion in patients compared with a control group.
Methods
Patients
This was a retrospective cohort study of a consecutive series of patients who underwent arthroscopic debridement and contracture release of the elbow for symptomatic degenerative arthritis between January 2015 and July 2018. The study was prompted by a change in practice that began in July 2016, which resulted in the routine administration of IV TXA during elbow arthroscopy, in an effort to reduce intra-articular bleeding, swelling, and postoperative drain tube output. Before this point, IV TXA was not routinely administered during elbow arthroscopy, and this provided the control group for comparison. There was no difference in surgical technique between the 2 groups. Ethics committee approval was obtained before commencement of this study, and informed consent was obtained from each patient.
During the study period, a total of 150 patients underwent elbow arthroscopy by the senior author (E.T.E.). Patients were included if they were aged >18 years and had undergone an arthroscopic debridement of impinging osteophytes and contracture release of the elbow for degenerative osteoarthritis with a symptomatic flexion contracture of at least 10° and/or loss of flexion of least 120°. Patients were excluded if their elbow arthroscopy was performed for other reasons such as posttraumatic stiffness, isolated removal of loose bodies, plica debridement, arthroscopic fracture management, arthroscopic lateral ligament repair, and debridement of lateral epicondylitis or if there was a concomitant removal of hardware or any other open procedure. Furthermore, patients with known abnormal coagulation or bleeding profiles or a history of deep vein thrombosis/venous thromboembolism, stroke, or heart disease were excluded from receiving IV TXA.
Eighty-three patients fulfilled the inclusion criteria and were included in the study, with 43 patients in the no-TXA group and 40 patients in the TXA group. The characteristics for the 2 groups are displayed in Table 1. There was no significant difference between the 2 groups with respect to age, sex, or hand dominance.
Patient Characteristics a

a Data are presented as mean ± SD or No. (%). TXA, tranexamic acid.
b Statistical analysis concomintant ulna nerve surgery between the 2 groups was not performed as it was not relevant to the aims of the study. Hence no P value is provided.
Surgical Technique
On induction, all patients received 8 mg of IV dexamethasone for swelling, which was continued postoperatively with 2 further doses 8 hours apart. All patients had either a general anesthetic or IV sedation with a long-acting regional brachial plexus block. Patients were placed in the lateral decubitus position, supported by a beanbag. A nonsterile tourniquet was placed high in the arm, and the arm was supported over a Western Elbow Positioner (Smith & Nephew) and stabilized to the holder using Microfoam tape (3M). Bony and soft tissue landmarks were identified and marked, and 20 mL of normal saline was injected into the elbow joint via the soft spot portal to insufflate the joint. An Esmark bandage was then applied, and the tourniquet was inflated to 250 mm Hg.
For patients with preoperatively determined ulnar nerve symptoms, a neurolysis with or without anterior subcutaneous transposition was performed before the arthroscopy. The nerve was then protected throughout the rest of the procedure. It is the senior author’s preference to approach the posterior compartment first. A complete synovectomy was performed, and the triceps was elevated from the distal humerus to allow increased excursion in elbow flexion. After removal of any loose bodies, if the olecranon tip was noted to be prominent, causing impingement with elbow extension, it was osteotomized using an 8-mm Lambotte osteotome via the direct posterior portal. Corresponding osteophytes in the olecranon fossa were removed using a high-speed bur. The elbow was extended to ensure that there was no potential for further bony impingement. The posterolateral compartment (radiocapitellar joint) was then addressed, and any bony or soft tissue debris was cleared from the joint and the surrounding capsule.
The anterior compartment was addressed last, with the arthroscope placed through a proximal anteromedial portal, and a working proximal anterolateral portal was established under direct vision. The anterior capsule was elevated from the humerus using a radiofrequency device, and where necessary, osteophytes were removed using a high-speed bur from the anterior humerus and the coronoid tip. The elbow was maximally flexed to ensure that there was no ongoing impingement. If full extension was still limited, an anterior capsulectomy was performed from lateral to medial using an arthroscopic Duckbill biter, exposing the overlying brachialis muscle. The elbow was then manipulated in both flexion and extension to obtain maximal range of motion.
Administration of TXA
For patients who were administered TXA, 1.0 g of TXA was administered intravenously at the completion of the arthroscopic procedure while the wounds were being closed. The tourniquet remained inflated during this time.
Perioperative Management and Rehabilitation
A single 10F (3.33-mm diameter) Redivac drain tube was inserted into the posterolateral portal of the elbow and clamped with no suction. The arthroscopic portals were closed using 3-0 nylon sutures in an interrupted fashion. Standard dressings were applied, the elbow was placed into a bulky bandage, and the tourniquet was then deflated. The clamp on the drain tube was only opened when the patient was transferred to the recovery room. No patients in this series required postoperative flexion or extension splinting. All patients were admitted to the hospital overnight, and cryotherapy was applied to the elbow (DonJoy IceMan; DJO Global).
On postoperative day 1, the bandages were removed, and a compressive sleeve was placed over the elbow. The patient then underwent graduated passive motion of the elbow in a CPM machine for 2 hours. After CPM, the drain tube was removed, and the volume of blood in the bottle was routinely recorded. In all patients, the drain tube was in place between 18 and 24 hours postoperatively and was removed if the output had ceased or was <10 mL/h.
Patients were discharged with a compression sleeve, and they were encouraged to regularly place ice over the elbow and maintain passive and active-assisted range of motion of the elbow, as tolerated. Regular nonsteroidal anti-inflammatory drugs were also encouraged for the first 3 weeks postoperatively. Patients were followed up between days 10 and 14, when the sutures were removed and formal physical therapy commenced. Postoperative rehabilitation comprised gentle progressive stretching exercises, both passive and active-assisted. Patients were routinely followed up at week 8, when progress and range of motion of the elbow were assessed. In most cases, patients were then discharged into the care of their local physical therapist for ongoing rehabilitation.
Evaluation and Outcomes
Patient records were retrospectively analyzed with respect to the recorded drain tube output before drain removal. We also recorded the pre- and postoperative range of motion as assessed via handheld goniometer and the pain level on postoperative day 1 as measured on a visual analog scale (VAS; 0 [no pain] to 10 [worst pain]). In all patients, videos of their elbow arthroscopy were kept in a database. This allowed for detailed assessment and grading of the extent of elbow debridement: (1) olecranon tip, (2) olecranon fossa, (3) anterior humerus, (4) coronoid tip, (5) radial head/capitellum, and (6) anterior capsulectomy.
The primary outcome measure in this study was the amount of drain tube output. Secondary outcome measures included pain levels, whether the extent of debridement influenced drain tube output, and improvements in early range of motion of the elbow.
Statistical Methods
Data were described using means, standard deviations, and ranges. The difference in outcomes between patients who were administered TXA and those who were not was analyzed using 1-way analysis of variance or Mann-Whitney U test; the Fisher exact test was used for categorical data. All statistical analyses were performed using SPSS Version 20.0 (IBM Corp). Differences with a P value <.05 were deemed statistically significant.
A post hoc analysis was performed to confirm appropriate sample sizes to detect a difference of >50%, with an α = .05 and power of 0.8.
Results
Drain Tube Output and Pain
In patients who were administered TXA at the time of elbow arthroscopy, the mean volume of drain tube output was 43.4 ± 52.4 mL (range, 0-190 mL). This was significantly less than that of patients who were not administered TXA, in which the mean drain tube output was 88.8 ± 80.5 mL (range, 0-350 mL) (P = .0016). This represented a 51% reduction in output (Table 2 and Figure 1). Regarding day 1 postoperative pain levels, there was no difference in VAS scores between the no-TXA and TXA groups (Table 2).
Comparison of Postoperative Drain Tube Output and Pain Between the Study Groups a

a Data are presented as mean ± SD (range). Bolded P value indicates a statistically significant difference between groups (P < .05). TXA, tranexamic acid; VAS, visual analog scale.

Comparison of postoperative drain tube output between the no-TXA and TXA groups and in patients who did and did not have an anterior capsulectomy. Error bars indicate SDs. *Statistically significant difference between the no-TXA and TXA groups (P < .05). TXA, tranexamic acid.
To determine whether performing an anterior capsulectomy was associated with increased intra-articular bleeding and hence greater drain tube output, we compared the volumes in both groups, with or without anterior capsulectomy. In the no-TXA group, there was no significant difference between capsulectomy and no capsulectomy (106.0 ± 75.3 mL [range, 5-240 mL] vs 83.6 ± 82.4 mL [range, 0-350 mL]; P = .245). Similarly, in the TXA group, there was also no significant difference between capsulectomy and no capsulectomy (46.3 ± 39.9 mL [range, 0-110 mL] vs 42.7 ± 55.6 mL [range, 0-190 mL]; P = .575) (Figure 1).
Extent of Elbow Debridement
In the no-TXA group, the mean number of sites of debridement was 3.1 ± 1.0, with 5 patients (11.6%) who had only 1 site of debridement, 5 patients (11.6%) with 2 sites, 15 patients (34.9%) with 3 sites, 17 patients (39.5%) with 4 sites, and 1 patient (2.3%) with 5 sites. The TXA group had a mean 3.0 ± 1.3 sites of debridement, with 7 patients (17.5%) who had only 1 site of debridement, 7 patients (17.5%) with 2 sites, 10 patients (25%) with 3 sites, 12 patients (30%) with 4 sites, and 4 patients (10%) with 5 sites. We found no significant difference between the no-TXA and TXA groups with respect to the extent of debridement performed (P = .69). Furthermore, within each group, there was no relationship between the volume of drain tube output and the number of sites of debridement (Table 3).
Comparison of Drain Tube Output by Number of Anatomic Sites Debrided a

a Data are presented as mean ± SD. TXA, tranexamic acid.
Range of Elbow Motion
In the no-TXA group, the mean preoperative arc of motion was 100.5° ± 22.6° (range, 60°-140°). There were 21 patients (48.8%) with a mild contracture (arc, >100°), 20 patients (46.5%) with a moderate contracture (arc, 61°-100°), and 2 patients (4.7%) with a severe contracture (arc, ≤60°). At the 8-week follow-up, the mean arc of motion had significantly improved to 129.7° ± 12.4° (range, 80°-145°) (P < .00001) (Table 4). All except for 1 patient had an arc of motion >100°. In the TXA group, the mean preoperative arc of motion was 108° ± 21.5° (range, 45°-145°); 23 patients (57.5%) had a mild contracture, 16 patients (40%) had a moderate contracture, and 1 patient (2.5%) had a severe contracture. At the 8-week follow-up, the mean arc of motion had significantly improved to 131.7° ± 9.2° (range, 100°-140°) (P < .00001), and all patients had an arc of motion >100°. There was no significant difference between the no-TXA and TXA groups with respect to preoperative or postoperative range of motion (Table 4).
Comparison of Preoperative and 8-Week Postoperative Elbow Range of Motion Between the Study Groups a
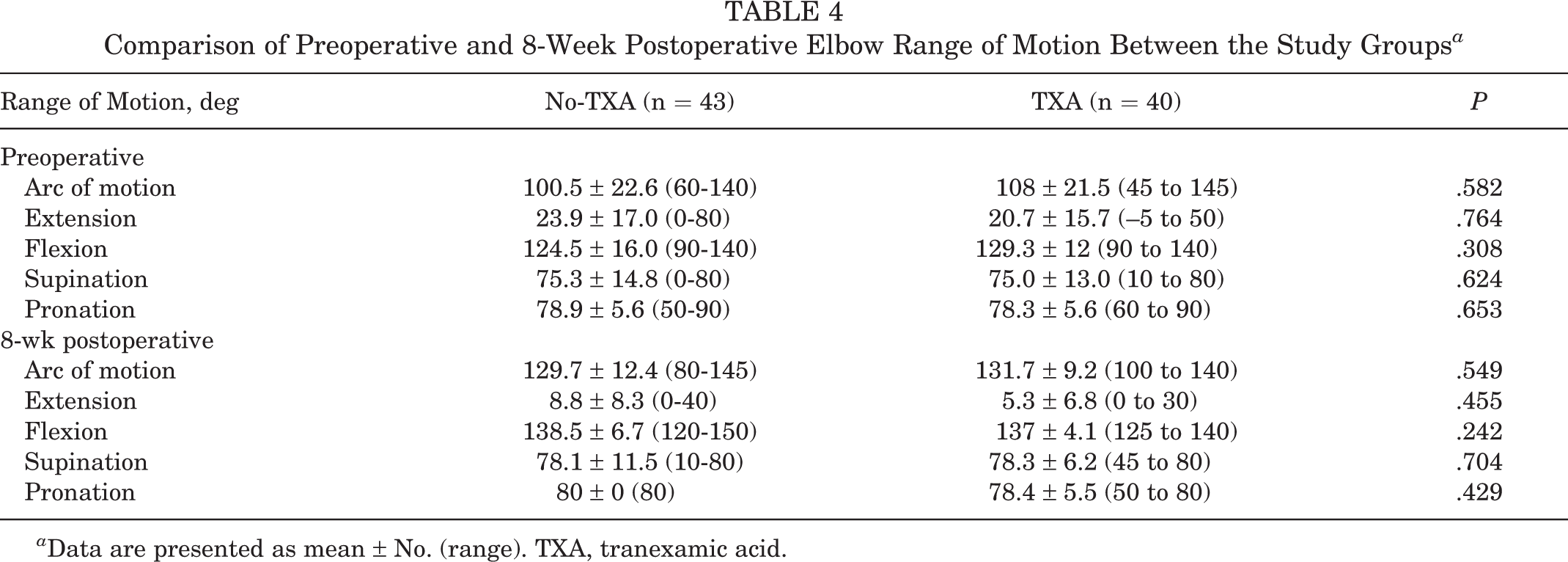
a Data are presented as mean ± No. (range). TXA, tranexamic acid.
Discussion
This study is the first to demonstrate the role of TXA in reducing postoperative bleeding after arthroscopic osteocapsular release of the elbow for primary osteoarthritis. Our results showed that IV TXA, when administered before the release of the tourniquet, resulted in a 51% reduction in drain tube output in patients when compared with a control group (88.8 ± 80.5 mL vs 43.4 ± 52.4 mL; P = .0016). These findings add to the growing body of literature that has demonstrated the effectiveness of TXA in reducing bleeding after various surgeries, particularly those in which success depends on minimizing hemarthrosis and soft tissue swelling, allowing for early active motion to reduce joint stiffness and postoperative pain. 7,11,20 These results have also been demonstrated in the knee after anterior cruciate ligament reconstruction and total knee arthroplasty. 11,23
To our knowledge, only 1 other study has been performed with respect to TXA for contracture releases of the elbow. In that study, Zhang et al 24 used 1.0 g of topical TXA during open arthrolysis of the elbow for posttraumatic stiffness and reported significantly less intraoperative blood loss and also postoperative drain tube output compared with that of the control group. In contrast, we used 1.0 g of IV TXA, which was administered at the end of the arthroscopic procedure, at the time of wound closure, and before release of the tourniquet. The efficacy and safety of IV versus topical TXA are still debated; however, most studies have shown that both routes are equally effective in reducing the level of bleeding. 5,7,14 Jules-Elysee et al 14 compared topical and IV TXA for total knee arthroplasty and demonstrated that IV TXA resulted in higher wound concentrations, suggesting that the wound was the major site of action despite the mode of administration; lower systemic TXA levels were observed in the topical group; but both were within therapeutic range. In terms of safety, there is now emerging evidence that IV TXA is not associated with increased complications in patients with a history of thrombotic events and does not increase the risk of perioperative seizures. 5,15
As aforementioned, minimization of bleeding postoperatively is of utmost importance to reduce subsequent elbow swelling and edema, which, in turn, can have a mechanical effect on elbow motion but also can lead to granulation tissue formation both within the joint and in the soft tissues, resulting in fibrosis and stiffness. 6,9,25 This is the basis of the large majority of adjunctive measures that are employed after both elbow trauma and surgery, such as the use of anti-inflammatory drugs, cryotherapy, compression bandages, and early range of motion, all with the goal of reducing granulation tissue formation and hence minimizing recurrent elbow stiffness. 2,6,9,25 Based on our results, the addition of IV TXA is a simple and effective adjunct to the postoperative management regime. However, in our study, we were not able to show that TXA was effective in either reducing day 1 postoperative pain levels or significantly improving early range of motion of the elbow, with patients in our series achieving an early postoperative arc of motion of 130° ± 12° (no-TXA) compared with 132° ± 9° (TXA) (P = .549). These results are not dissimilar to those of Zhang et al, 24 who also showed no difference in both early and late (1 year) range of motion of the elbow, with and without TXA.
Distinction must be made between the pathoetiology of primary osteoarthritis versus posttraumatic stiffness of the elbow, although the treatment options are frequently the same. The origin of posttraumatic elbow stiffness is most often multifactorial and may result from arthrosis from articular injury or incongruity, heterotopic ossification, fracture nonunion, and contracture of the soft tissues and joint capsule. 2,3,6 On the other hand, primary osteoarthritis is characterized by loose bodies and impinging osteophytes between the olecranon tip and fossa and/or the coronoid process and the anterior humerus, with relatively well-preserved and congruent articular cartilage. 2,16 Hence, in this group of patients, the main principle of surgery is to debride the prominent osteophytes to relieve the mechanical block to motion. Therefore, this invariably results in exposed bone surfaces, which have the propensity to bleed. As such, reducing the hemarthrosis via the administration of TXA and also the use of a drain tube is likely to be of benefit in reducing arthrofibrosis. In our study, we tried to determine whether a larger number of sites of debridement influenced the degree of intra-articular bleeding. The mean number of sites that were debrided was 3.1 ± 1.0 in the no-TXA group compared with 3.0 ± 1.3 in the TXA group (P = .69). We found that there was no significant correlation between the number of sites debrided and the extent of bleeding in either group. Furthermore, performing an anterior capsulectomy also did not result in increased bleeding in both groups.
The strength of this study is that a consecutive series of patients underwent surgery by a single surgeon using a standardized technique of arthroscopic osteocapsular release with routine postoperative protocols. In addition, this series represents a well-defined cohort of patients who have primary degenerative arthritis of the elbow, hence allowing for more uniform interpretation of the results. However, the limitations are that it is a retrospective case-control study with relatively small numbers. Although our study was sufficiently powered to detect a difference in the primary outcome measure, that is, drain tube output, it is likely, given the multiple modalities already used postoperatively to minimize bleeding and elbow joint swelling, that a substantially larger numbers of patients would be required to detect any significant changes in secondary outcome measures, such as pain levels and elbow range of motion. In addition, we do recognize that in this study there may have been variations in the measurement of drain tube output, with respect to timing postsurgery and in terms of accuracy, which may influence the overall results.
Conclusion
In this study, we demonstrated that 1.0 g of IV TXA significantly reduced postoperative intra-articular bleeding, as measured via drain tube output, in patients undergoing arthroscopic osteocapsular release of the elbow for primary arthritis. However, between the 2 groups, we did not detect any difference in day 1 postoperative pain levels or early elbow range of motion. Based on the results of this study, further research in this area is needed, and a prospective randomized controlled trial should be performed, with variations in dosage, timing, and length of administration of TXA and also longer follow-up with respect to clinical outcome measures.
Footnotes
Final revision submitted October 17, 2021; accepted January 10, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Avenue Hospital, Ramsay Health (reference No. 225).