
Abstract
Background:
Lateral epicondylitis of the elbow is a common degenerative disorder in middle-aged patients. Surgery is reserved for patients who do not respond to nonoperative treatment.
Purpose:
To evaluate hand-grip strength and return to heavy manual activities in patients engaged in work requiring heavy lifting after arthroscopic release of refractory lateral epicondylitis.
Study Design:
Case series; Level of evidence, 4.
Methods:
The study included consecutive patients who underwent arthroscopic release of the extensor carpi radialis brevis tendon to treat recalcitrant lateral epicondylitis of the elbow, with a minimum 48-month follow-up. Functional outcome measures included assessment of hand-grip strength, visual analog scale for pain, and Mayo elbow performance score. The recorded measurements were compared at postoperative 1 and 6 months and the final assessment. Pre- and postoperative data were compared using the paired t test, and the various postoperative assessments were compared using 1-way analysis of variance.
Results:
A total of 22 patients (mean ± SD; age, 34.6 ± 5.9 years) with a mean follow-up of 60.5 ± 4.7 months were included in our study. There were highly significant improvements between preoperative and 1-month postoperative results regarding hand-grip strength (17.5 ± 4.1 kg to 34.4 ± 6.8 kg), visual analog scale score for pain (7.86 ± 1.2 to 1.8 ± 1.09), and Mayo score (57.1 ± 7.9 to 89.3 ± 4.9; P < .00001 for all). Significant improvements were found on all 3 functional measures between 1 and 6 months postoperatively (P ≤ .05 was statistically significant), and there were nonsignificant improvements on all measures from 6-month to final follow-up. The patients regained 96.4% of their hand strength as compared with the unaffected side and returned to their previous activities without reporting serious complications.
Conclusion:
Minimally invasive arthroscopic release of recalcitrant lateral epicondylitis of the elbow provided a satisfactory functional result, as shown by regaining of hand-grip strength in patients engaged in heavy manual occupations without significant morbidities.
The incidence of lateral epicondylitis of the elbow (also known as tennis elbow) ranges from 1% to 3% in the entire population and 7% in heavy manual workers; it often occurs in individuals aged 30 to 60 years, with equal distribution between the sexes. 8,17 The condition affects people with different activity levels and occupations and imposes a remarkable socioeconomic burden, assuming 11.7% of work-related injury claims. 20
The chief complaint of lateral epicondylitis is lateral elbow pain exacerbated by repeated wrist dorsiflexion and forearm pronation-supination. Additionally, there is a weakness of the forearm muscles with diminished hand-grip strength hindering patients’ daily activities. 5,6 The pathophysiology of this disorder is degeneration of the extensor carpi radialis brevis (ECRB) tendon because of repeated wrist extensions and forearm rotations. 11 Additionally, other associated intra-articular pathologies may be present, such as synovitis, hypertrophy of the annular ligament, and chondral lesions. 1 If these lesions are missed during surgical intervention, persistent pain and patient dissatisfaction after surgery can result. 15,16
Over 80% of patients respond well to nonoperative measures such as activity modification, physical therapy, nonsteroidal anti-inflammatory drugs, a brace, extracorporeal shock wave therapy, and local injection of corticosteroids or platelet-rich plasma. 18 These measures should be tried for at least 6 months before considering operative intervention. 3,10
Surgery is reserved for recalcitrant cases and failed nonoperative management. The aim of surgery is to excise the degenerated part of the tendon to promote neovascularization and subsequent healing. There are 2 principal methods of surgical intervention: either the open or arthroscopic approach. 21 With the evolution of modern arthroscopic techniques and equipment, arthroscopic release of recalcitrant tennis elbow has gained popularity in the past decade. Good evaluation of other concomitant intra-articular pathologies, faster rehabilitation, and lower morbidities are the major benefits of this technique. 2
To our knowledge, there are no prospective midterm follow-up studies to investigate the outcome of hand-grip strength and return to heavy manual labor after arthroscopic release of resistant lateral epicondylitis of the elbow. The purpose of our study was to assess the recovery of hand-grip strength and return to heavy manual activities at midterm follow-up after arthroscopic release of recalcitrant lateral epicondylitis, including an assessment of the time required for functional improvement. We hypothesized that there would be satisfactory midterm functional outcomes, enabling a return to the previous level of activity involving heavy work.
Methods
Our institutional review board approved this prospective series study, and informed consent was obtained from all participants. The study was conducted between November 2015 and April 2021 at Zagazig University Hospitals. Twenty-two consecutive patients (17 men and 5 women) with recalcitrant chronic lateral epicondylitis were eligible for our study. The mean ± SD patient age was 34.6 ± 5.9 years (range, 24-46 years). All patients had undergone nonoperative treatment in the form of rest, physical therapy, nonsteroidal anti-inflammatory drugs, and 1 or 2 corticosteroid injections for at least 6 months before surgery, after which they were treated with arthroscopic release of the ECRB tendon. Patients were excluded if they had rheumatoid arthritis, hyperuricemia, previous injury or surgery of the ipsilateral elbow, radial tunnel syndrome, follow-up <48 months, and age <18 years. The demographic data of the study patients are summarized in Table 1.
Demographic Characteristics of the Study Patients (N = 22)

Preoperative Assessment
Clinical assessment of the patients through a detailed history, examination, and provocative tests was performed first before operative intervention. All patients tested positive for the Cozen test (lateral elbow pain with resisted wrist dorsiflexion) with no limitation of elbow motion. Posterior elbow pain and snapping in the terminal degrees of elbow extension are suggestive of posterior radiocapitellar plica. All patients were clinically free of such lesions. Additionally, a posterolateral rotatory drawer test was performed to check for lateral elbow instability, and no patients tested positive. Radial tunnel syndrome was noted clinically by identification at the site of pain and the point of tenderness (5 to 6 cm distal to the lateral epicondyle). Anteroposterior and lateral plain radiographs of the elbow were acquired to exclude osteochondral lesions and old fractures. Magnetic resonance imaging was performed to confirm the diagnosis of ECRB tendon degeneration, exclusion of chondral lesions, and associated intra-articular pathology (Figure 1).

Magnetic resonance imaging T2 sequence. Coronal view shows increased signal intensity at the extensor carpi radialis brevis origin (white arrow) denoting tendon degeneration.
The preoperative hand-grip strength, visual analog scale (VAS) pain score, 9 and Mayo elbow performance score 7 were recorded for functional evaluation. Hand-grip strength (kg) was measured by a handheld dynamometer (Renhotec) (Figure 2), and the strength of the affected side was compared with that of the contralateral side.

Handheld dynamometer used to measure the hand-grip strength.
Surgical Technique
All surgery was performed by the same surgeon (F.S.F.), with the patient under general anesthesia and a well-padded arm tourniquet inflated to 250 mm Hg. The patient was placed lying down in a lateral position with the arm hanging over a holder and the elbow at 90° (Figure 3).
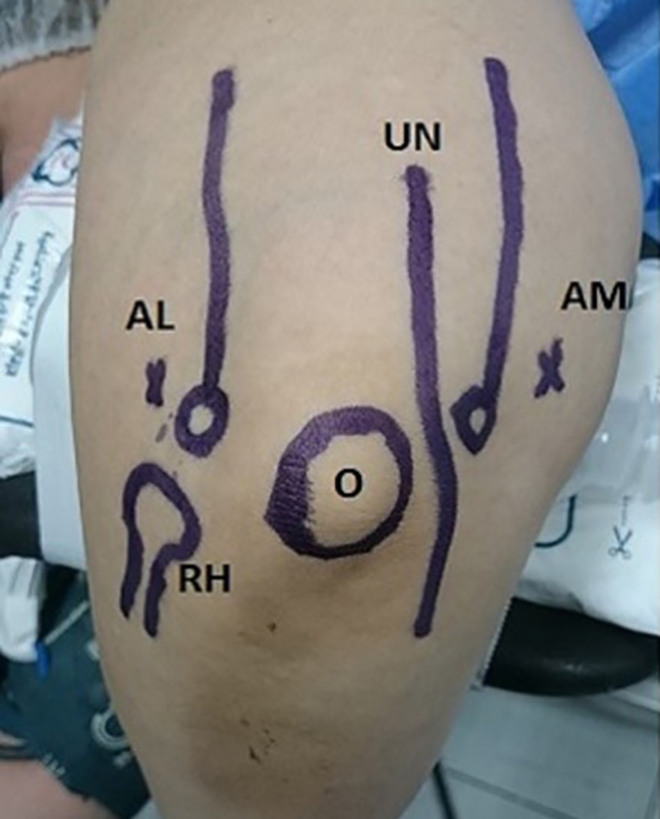
Patient position and skin marking of anatomic landmarks of the elbow. AL, anterolateral portal; AM, anteromedial portal; O, olecranon; RH, radial head; UN, ulnar nerve.
The joint was injected with 30 mL of saline to distend the joint capsule through the soft spot between the olecranon, capitellum, and radial head. The arthroscope was introduced into the anterior compartment of the elbow through the anteromedial portal (2 cm proximal and 1 cm anterior to the medial epicondyle), and the joint was inspected for ECRB tendon degeneration, plica, synovitis, and hypertrophy of the radiocapitellar capsular complex (Figure 4). The assistant applied axial loading of the forearm with maximum supination (pivot-shift test) while the position of the radial head on the capitellum was observed under direct arthroscopic visualization to assess elbow instability. Inspection of the posterior compartment through the soft spot portal is mandatory if there is clinical suspicion about the posterior plica. The working anterolateral portal was made outside-in under arthroscopic monitoring.

Arthroscopic view showing hypertrophy of the radiocapitellar capsular complex with degeneration of the capsule and extensor carpi radialis brevis tendon. C, capitellum; RCC, radiocapitellar capsular complex; RH, radial head.
Through the anterolateral portal, a 3.5-mm motorized shaver (Stryker) was used for debridement of the degenerated capsule and ECRB tendon until the muscle fibers of the extensor carpi radialis longus appeared (Figure 5). Debulking of the radiocapitellar capsule and annular ligament was necessary if there was impingement with elbow flexion. Resection was not done beyond the equator of the head radius to avoid injury of the ulnar part of the lateral collateral ligament (Figure 6).

(A) The degenerated extensor carpi radialis brevis tendon before resection. (B) Debridement of the degenerated tendon and capsule using a 3.5-mm motorized shaver. C, capitellum; D, degenerated tendon.

After completion of the procedure, the extensor carpi radialis brevis tendon is completely released but not beyond the radial head equator with debulking of the radiocapitellar capsular complex. ECRL, extensor carpi radialis longus; RH, radial head.
Postoperative Care and Follow-up
The arm was immobilized in a sling for 48 hours after surgery, and stitches were removed after 2 weeks. Passive motion of the wrist and elbow as much as the patient could tolerate was allowed immediately. Light hand activities were allowed during the first 4 weeks after surgery. Resistive exercises and gradual return to heavy manual work were allowed after 6 weeks. Functional scores (VAS for pain and Mayo score) and hand-grip power were estimated at postoperative 1 and 6 months and at the end of follow-up.
Statistical Analysis
The numerical values are presented as means and standard deviation, with calculation of 95% CIs for means. The Kolmogorov-Smirnov test was used to assess the normality of the studied group. The paired t test was used to estimate the difference between pre- and postoperative means after 1 month. One-way analysis of variance and the post hoc Tukey test were utilized to detect the differences between the postoperative 1- and 6-month scores and the final means. In all tests, P <.05 was indicative of statistical significance. The sample size that gave 90% statistical power for an α error of .05 and an effect size difference of 0.8 was calculated by the G*Power software calculator (Version 3.1). SPSS (Version 16.0; IBM) was used for statistical analysis.
Results
Our study included 22 patients with chronic tennis elbow with a mean age of 34.6 years. The mean follow-up time was 60.5 ± 4.7 months with no missed patient. No major complications were reported in this study. Only 1 patient had mild postoperative tourniquet neuropraxia, which resolved within 3 weeks of surgery. No cases of elbow instability or recurrence were reported. Hypertrophy of the radiocapitellar capsular complex and annular ligament was the main concomitant intra-articular finding, which was discovered in 17 patients: 14 with type II (partial radial head coverage) and 3 with type III (partial coverage with impingement). No other associated lesions were noticed. The mean duration of symptoms before surgery was 10.8 ± 2.6 months (range, 6-15 months).
All functional outcomes improved from preoperative values and over time, as shown in Figure 7 and Table 2. As compared with presurgery, there was a highly significant improvement in mean hand-grip strength at 1 month postoperatively (P < .00001) and continued significant improvement between 1 and 6 months (P < .00001). There was nonsignificant improvement between 6 months postoperatively and final assessment (P = .8). At the end of the study, the mean strength of the affected hand vs the contralateral hand was 43.3 ± 6.2 kg vs 44.9 ± 6.2 kg, respectively, indicating that the patients had regained 96.4% of their normal hand power.
Final Results for Functional Scores and Hand-Grip Strength a
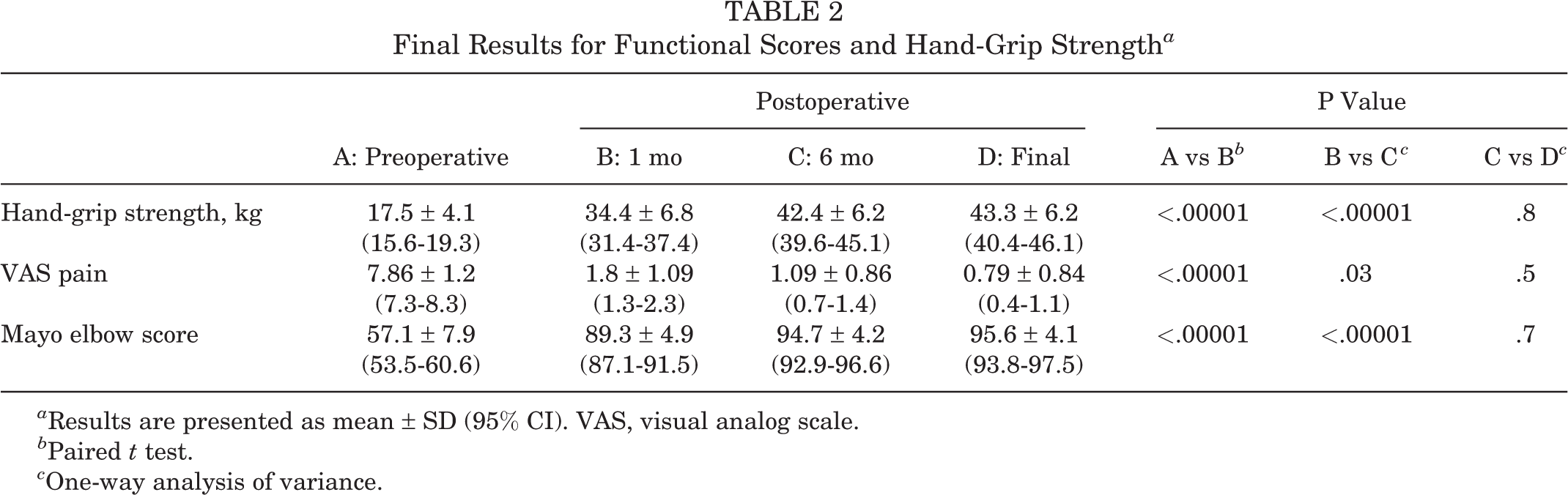
a Results are presented as mean ± SD (95% CI). VAS, visual analog scale.
b Paired t test.
c One-way analysis of variance.
There was highly significant improvement in the 1-month postoperative VAS score from that recorded preoperatively (P < .00001) (Table 2). The improvement continued from 1 to 6 months postoperatively (P = .03), but the improvement was not significantly different between the 6-month and final VAS score (P = .5).
Improvement in the Mayo elbow performance score from presurgery to postoperative 1 month was highly significant, as was the improvement between 1 and 6 months (P < .00001 for both); however, the improvement between 6 months and the final score was not significant (P = .7) (Figure 7, Table 2).
The mean time to return to preoperative activities was 16.7 ± 3.1 weeks. All patients returned to their preoperative levels of activity and occupations without a functional deficit, and all were satisfied with the ultimate outcomes.

Histogram for the results of hand-grip strength, VAS pain, and Mayo elbow performance score. VAS, visual analog scale.
Discussion
Our main finding is the highly significant improvement of the functional elbow scores (VAS and Mayo score; P < .00001) and restoration of the normal hand-grip power (96%) at the end of the study. All patients regained their preoperative manual activities, and they were satisfied with the results. The study hypothesis was confirmed.
Kraushaar and Nirschl 11 described lateral epicondylitis as tendinosis rather than inflammation. They found an area of degeneration and the loss of a normal collagen pattern within the ECRB tendon. The healing process is incomplete with formation of angiofibroblastic tissues replacing the collagen fibers owing to repeated microtrauma. The diagnosis is mainly clinical, and management varies from simple nonoperative measures in most patients to surgical intervention in refractory cases. 3 The rationale of surgery is removal of the degenerated tissue to enhance the vascularity, bring more growth factors, and induce new collagen synthesis. 18
The main issues with open surgery are iatrogenic posterolateral instability, missing any intra-articular lesions, cosmetics, and longer rehabilitation. 1,14 In addition to being a minimally invasive technique that provides earlier rehabilitation and a lower rate of complications, arthroscopic release of resistant chronic tennis elbow has the advantage of detecting concomitant intra-articular pathologies that may prevent good postoperative functional outcomes and patient satisfaction if left untreated. 4,22
Babaqi et al 1 found that an impinging radiocapitellar capsular synovial fold with hypertrophy in the annular ligament was associated with chronic lateral epicondylitis in all cases of their study. This lesion was treated with an arthroscopic partial resection. We discovered this pathological finding in 17 (77.2%) patients intraoperatively.
Restoration of hand-grip strength is a crucial factor for returning to heavy manual activities. Our study showed that 96.4% of normal hand-grip power was recovered, with 43.3 ± 6.3 kg reported at the end of the study. In a retrospective study by Soeur et al, 18 the recorded muscle strength deficit was 4.3% at the end of the follow-up period. Oki et al 14 stated that 98.5% of hand-grip power relative to that of the other side was recovered 12 months after surgery. Their results are comparable with our results. In a retrospective study, Yoon et al 22 cited a final hand-grip strength of 33.5 ± 6.9 kg in 37 patients, which is inferior to our value because our patients were regularly engaged in heavy manual activities and so had greater muscle strength. Additionally, we had only 5 (22.7%) female patients in our study vs 15 (40.5%) of 37 patients in their series.
Regarding the resolution of pain, the VAS score in our study improved from 7.86 ± 1.2 preoperatively to 0.79 ± 0.84 at the end of the study. Yoon et al 22 treated 45 patients with arthroscopic ECRB release, and the VAS score improved (6.9 ± 1.0 to 0.9 ± 0.9) as it did in our study. When compared with the results of Oki et al, 14 who cited a mean VAS score >2 with activities, our result was superior. This may be explained by the predominance of women in their study (18/23 patients), the higher mean age (49 years), the longer duration of preoperative symptoms (32 months; range, 6-338), and the presence of concomitant intra-articular lesions in all of their patients. Solheim et al 19 stated that there was a significant correlation between poor surgical outcomes and female sex. Yoon et al recorded the preoperative Mayo elbow performance score (63.5 ± 13.3) and reported that it significantly improved to 92.3 ± 10.6 at the end of follow-up, which is comparable with our final mean (95.6 ± 4.1).
The estimated mean time of return to work in our series was 16.7 weeks, which is longer than that estimated by Oki et al 14 and Kwon et al 12 (8.6 and 8.7 weeks, respectively). In contrast to our patients who were engaged in heavy manual occupations, most of their patients had light manual activities (16/23 patients in the first study [69.5%]; 20/29 in the second [68.9%]), which may explain the longer recovery time in our study.
We also investigated the time sequence of functional improvements in our study. The hand-grip strength and functional scores were significantly improved at 1 month after surgery, with maximum improvement achieved at 6 months. Although there was a continued increase in the estimated values until the end of the study, these increments were neither clinically nor statistically different from the value recorded at 6 months. The sequence of functional recovery was estimated by Oki et al, 14 who concluded that the maximum functional recovery occurred at 6 months after surgery, which is consistent with our observations. Our patients were cautioned against an early return to heavy lifting for at least 6 months after surgery.
Moradi et al 13 included 34 studies in their meta-analysis to compare functional outcomes and complication rates between the open and arthroscopic release of chronic tennis elbow. Fifteen open, 13 arthroscopic, and 6 combined studies were eligible. They declared that the arthroscopic approach had superior functional results with a lower complication rate than open surgery. We did not report any major morbidities or recurrence. Only 1 patient had temporary tourniquet neuropraxia, which resolved spontaneously within 3 weeks of surgery.
Our study had several limitations. First, the number of enrolled patients was small but enough according to our power analysis, with just 19 elbows needed to give 90% statistical power. Second, there was no control group to enable comparison of this technique with other methods of treatment. Additionally, a longer follow-up is needed to detect late recurrence, and the healing process was not investigated in this study. Finally, arthroscopic release is a technically demanding surgery and should be performed by well-qualified surgeons; thus, this may not apply to the general orthopaedic surgeon treating lateral epicondylitis.
Conclusion
Arthroscopic release of chronic refractory tennis elbow has a satisfactory midterm functional outcome. Hand-grip strength was restored, and patients were able to resume their previous heavy manual work without limitations. Further studies will be needed to investigate the nature of the healing process.
Footnotes
Acknowledgment
The authors thank Bashnouna George Youssef for his contribution in recording and preparing the data for this study.
Final revision submitted October 18, 2021; accepted November 30, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Zagazig University (No. 432/22-10-2015).