
Abstract
Background:
Bone marrow lesions (BMLs) are common subchondral defects revealed by magnetic resonance imaging (MRI) in patients with osteoarthritis, often associated with pain and functional limitation. Subchondroplasty (SCP) is a relatively new technique in which bone substitute material (BSM) is injected inside BML areas to provide structural support to the subchondral bone, preventing its collapse and reducing pain.
Purpose/Hypothesis:
The purpose of this study was to characterize changes in pain, functional and radiological outcomes, conversion to knee replacement, and complications after SCP. We hypothesized that ≥70% of patients would achieve a reduction in pain of ≥4 points on a numeric rating scale (NRS) at a 6-month follow-up after SCP.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients with symptomatic knee BMLs who underwent SCP were prospectively evaluated preoperatively and at 1, 6, 12, and 24 months postoperatively. Functional outcomes were measured with the NRS for pain, Knee Society Score (KSS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and International Knee Documentation Committee (IKDC) scores. Radiographs and MRI were performed preoperatively and at 6- and 12-month follow-ups to verify edema healing and changes in bone structure.
Results:
A total of 50 patients were included in the study. The mean follow-up was 26 months (24-30 months). Compared with preoperative values, the mean NRS score decreased at every follow-up point (P < .0001 for all) and the IKDC, WOMAC, and KSS scores improved significantly at 6- and 12-month follow-ups. At 6 months postoperatively, 27 patients (54%) registered a reduction on the NRS of ≥4 points. Postoperative MRI revealed a hypointense zone surrounded by a hyperintense signal at the injection site. Standard radiography showed osteoarthritis grade worsening in 4 (8%) patients. Knee replacement was performed in 11 patients —in 7 patients due to the worsening or persistence of disabling symptoms and in 4 patients due to the progression of osteoarthritis. The leakage of BSM occurred in 6 patients without any clinical consequences during the study period.
Conclusion:
About half of the study patients achieved a reduction in the NRS of 4 points at the 6-month follow-up after SCP.
Registration:
NCT04905394 (ClinicalTrials.gov identifier).
Subchondral bone marrow lesions (BMLs) have been described in the knee, hip, clavicle, foot, and ankle of patients with osteoarthritis (OA). 17,22 They can be classified into 3 categories as follows: (1) reactive, which is caused by an inflammatory process; (2) ischemic, which is due to perfusion reduction; and (3) mechanical, which is imputable to joint malalignment and meniscal or ligamentous injuries. 1,26 They are commonly associated with OA when physiologic subchondral remodeling fails due to increased focal stress or reduced healing capacity of the subchondral bone. 7 Histologically, BMLs demonstrate nonspecific changes, including edema, fibrosis, medullary fat necrosis, trabecular bone microfractures, and poor mineralization. 11 Clinically, such lesions have been related to pain, joint surface deformation, and accelerated OA progression. 13 Radiologically, they are rarely recognized by standard radiographs and commonly characterized on magnetic resonance imaging (MRI) by the presence of an area of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images compared with normal bone marrow in fat-suppressed T2-weighted short-tau inversion recovery (STIR) and proton density sequences. 13,27 The literature demonstrated that patients with BMLs are 9 times more likely to undergo knee replacement within 3 years than those without BMLs; thus, interest is growing in treatment options directed toward the subchondral bone that aim to preserve the joint. 24
Treatment of BMLs has historically focused on conservative management, including off-loading, physical therapy, and anti-inflammatory drugs; however, these treatments are usually burdensome and involve partial or nonweightbearing for a long period. BMLs are also treated by pharmacological therapies such as prostacyclin, bisphosphonates, or intra-articular hyaluronic injections as well as core decompression and osteotomy. For more severe BMLs that are unresponsive to conservative measures, subchondroplasty (SCP) has emerged as a potential treatment to improve pain. 8 The SCP procedure is a minimally invasive, fluoroscopically assisted intervention that fills subchondral bone defects with bone substitute material (BSM), which is an engineered flowable osteoconductive calcium phosphate mineral compound that mimics the properties of cancellous bone and is resorbed and replaced by new bone during the healing process. 25 It is often performed in conjunction with arthroscopy to improve the accuracy of the desired injection site and to correct any associated intra-articular pathologies (ie, degenerative meniscal tears, loose bodies, chondral flaps, and synovitis), if present. 21 The goal of SCP is to improve the structural quality of the affected subchondral bone and promote local bone remodeling, aiming to prevent bone collapse and arthritis progression. 7
The purpose of this study was to characterize changes in pain, functional and radiological outcomes, and conversion to knee replacement, and complications after SCP. We hypothesized that ≥70% of patients would achieve a reduction in pain of ≥4 points on a numeric rating scale (NRS) at a 6-month follow-up. Furthermore, we evaluated the prevalence of patients with a ≥2-point reduction in pain NRS—the established minimal clinically important difference 10 (MCID)—at a 6-month follow-up. The secondary outcomes were functional improvement as well as any osteoarthritic and BML changes at short- and medium-term follow-ups.
Methods
This prospective observational cohort study protocol was approved by the regional ethical committee and was registered at ClinicalTrials.gov (Clinical Trials.gov ID NCT04905394; May 26, 2021). We enrolled consecutive patients with symptomatic knee BMLs resistant to nonoperative treatment who underwent SCP, and we prospectively evaluated them up to 2 years after surgery. They were selected according to the inclusion and exclusion criteria listed in Table 1.
Eligibility Criteria a
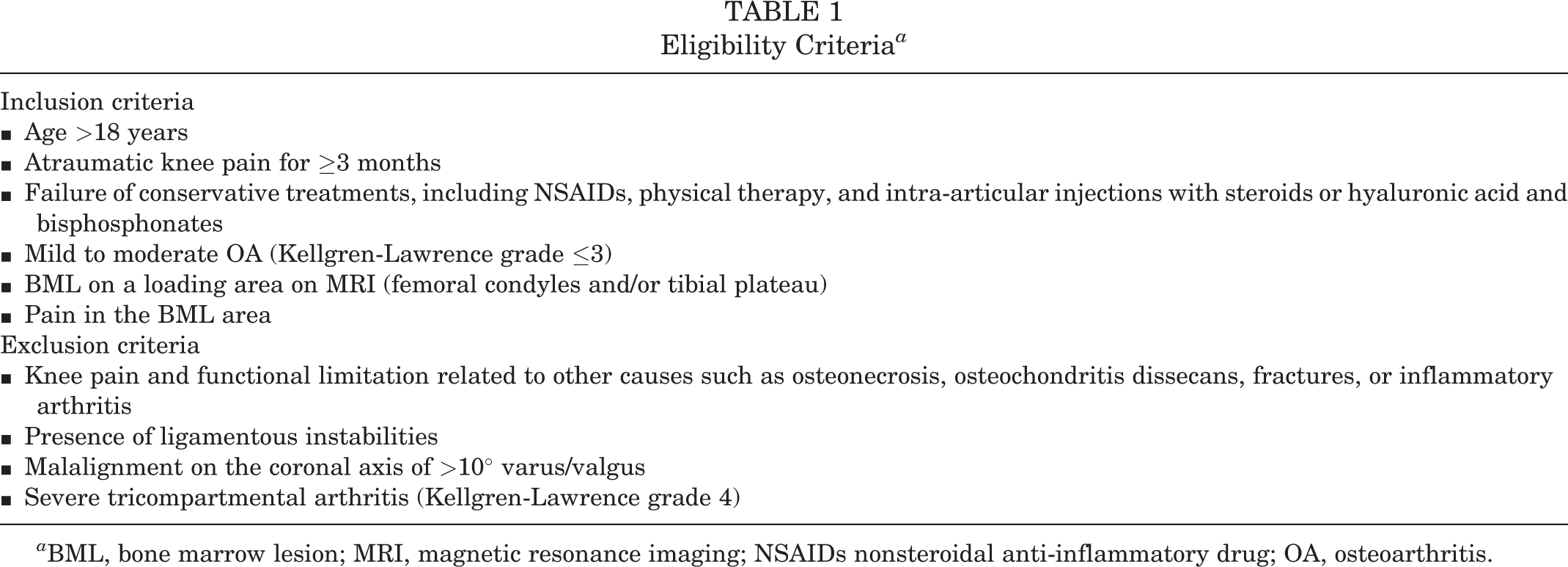
a BML, bone marrow lesion; MRI, magnetic resonance imaging; NSAIDs nonsteroidal anti-inflammatory drug; OA, osteoarthritis.
Preoperative Evaluation
Every patient underwent clinical assessment 1 week before surgery using the NRS for pain, 9 Knee Society Score (KSS) 6 , Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), 20 and International Knee Documentation Committee (IKDC) 18 scores. Knee radiographs and MRI (T1-weighted, T2-weighted, and STIR sequences) were performed to evaluate the BML size and location and knee OA, graded according to the Kellgren-Lawrence classification, and to exclude malalignment. 12
Surgical Technique
SCP was performed under spinal anesthesia. Patients lay supine on a radiolucent table with a cushion under the ipsilateral hip to better control limb external rotation. According to preoperative planning, the cannula entry point was anteroposteriorly and laterally demarcated with fluoroscopy. The BSM—an engineered calcium phosphate mineral compound—was then prepared until it reached liquid/pasty viscosity (Figure 1A). The fenestrated cannula was then introduced toward the center of the BML in the femoral lesion or the tibial lesion or both (Figure 1B). A delivery syringe filled with the BSM was attached to the back of the cannula and injected into the bone—an average of 2 mL in the femur and 3 mL in the tibia. A trocar was inserted into the cannula to push any remnants into the bone, then after hardening of the BSM, the cannula was removed (Figure 1, C-D). Finally, proper placing of the bone substitute was confirmed using fluoroscopic imaging and the incisions were sutured (Figure 1E). Arthroscopy was performed after the procedure to treat any concomitant pathology (eg, unstable meniscal tears) and eventually remove any intra-articular BSM leakage. Radiography was performed at the end of surgery to assess whether any extra-articular leakage had occurred.

Subchondroplasty procedure. (A) Preparation of bone substitute. (B) Fenestrated cannula. (C-E) Insertion of cannulas and injection of bone substitute under fluoroscopic guidance.
Postoperative Rehabilitation
Patients were allowed to resume weightbearing activities as tolerated with crutches assistance, if needed, for up to 2 weeks. Rehabilitation, including range-of-motion and strengthening exercises, started on day 1 after surgery, while return to full unrestricted activities was allowed 4 to 8 weeks postoperatively.
Postoperative Evaluation
All patients were clinically assessed at 1, 6, 12, and 24 months postoperatively using the same clinical scores as before surgery (NRS for pain, KSS, WOMAC, and IKDC) to evaluate knee pain and function. In addition, radiographs and MRI were performed at 6- to 12-month follow-ups to detect bone remodeling and OA progression.
Statistical Analysis
Statistical analysis (A.M. and A.D.S.) was performed using R Statistical Software (Version 4.0.0; R Foundation for Statistical Computing) and Graph Pad Prism Version 6.0 software (Graph Pad Software).
The sample-size calculation and 6-month evaluation point were determined based on previous studies. 4,5,14,16 With a sample size of 50, a confidence interval of about 10% would be obtained if the prevalence of success—defined as patients with a 4-point reduction in the 6-month NRS score—was 72%, indicating a high precision of the estimates.
The prevalence of success was calculated by dividing the number of patients with a 4-point reduction in the NRS score at the 6-month follow-up by the number of patients not lost to follow-up and was reported with a 95% CI. To be conservative, patients who underwent prosthetic replacement surgery before 6 months—for whom NRS scores at 6 months were unavailable—were considered as not achieving the 4-point reduction. In sensitivity analyses, patients with the NRS scores of <4 at the baseline and 0 at the 6-month follow-up were considered successes. We also calculated the prevalence of patients with a 2-point reduction in the NRS (MCID).
Continuous variables were recorded as the mean ± SD or medians and interquartile range as appropriate. The within-group differences from the baseline to different follow-ups for continuous variables were evaluated with the paired t test or the Wilcoxon matched-pairs signed-rank test according to the characteristics of the data distribution evaluated using the Shapiro-Wilk normality test. Categorical variables were recorded as the number of patients and frequencies. For all analyses, the significance level was set at P < .05.
Results
A total of 50 patients having chronic symptomatic BMLs were enrolled between April 2017 and February 2020. The mean follow-up period was 26 months (24-30 months). The age of patients ranged from 34 to 91 years, with a mean of 64.62 ± 11.39 years at the time of surgery. Also, 34 patients (68%) were women and 16 (32%) were men. The medial compartment was more frequently involved—14 BMLs in the medial femoral condyle, 15 in the medial tibial plateau, and 19 in both the femoral condyle and the tibial plateau (kissing) lesions. In 29 patients, a concomitant arthroscopic surgical procedure (eg, partial meniscectomy) was performed during the same surgery. According to the Kellgren-Lawrence classification, 7 patients had grade 0 knee OA, 16 patients had a grade of 1, 20 patients had a grade of 2, and 7 patients had a grade of 3. A complete description of the demographic characteristics of all the enrolled patients is reported in Table 2.
Patient Characteristics (N = 50 patients) a

a Continuous variables are expressed as mean ± SD and median [interquartile range]; binary variables are expressed as n (%). BMI, body mass index; OA, osteoarthritis; SCP, subchondroplasty.
Two patients were lost to follow-up because they withdrew their consent to participate in the study, leaving 48 patients. Eleven patients (22.9%) underwent prosthetic replacement surgery within the 24-month follow-up; for these patients, the last available scores before knee replacement were collected and analyzed. Patients who underwent a new procedure were excluded from further analysis at 6 months: the 2 patients that were lost to follow-up, and 3 patients underwent prosthetic replacement surgery; thus, the NRS was available for 45 patients 3 patients underwent knee replacement within the 6-month follow-up; another 6 patients underwent KR between 6-month and 12-month follow-up; another 2 patient underwent KR between 12-month and 24-month follow-up. 11 patients of the sample underwent KR during the study period (Figure 2).
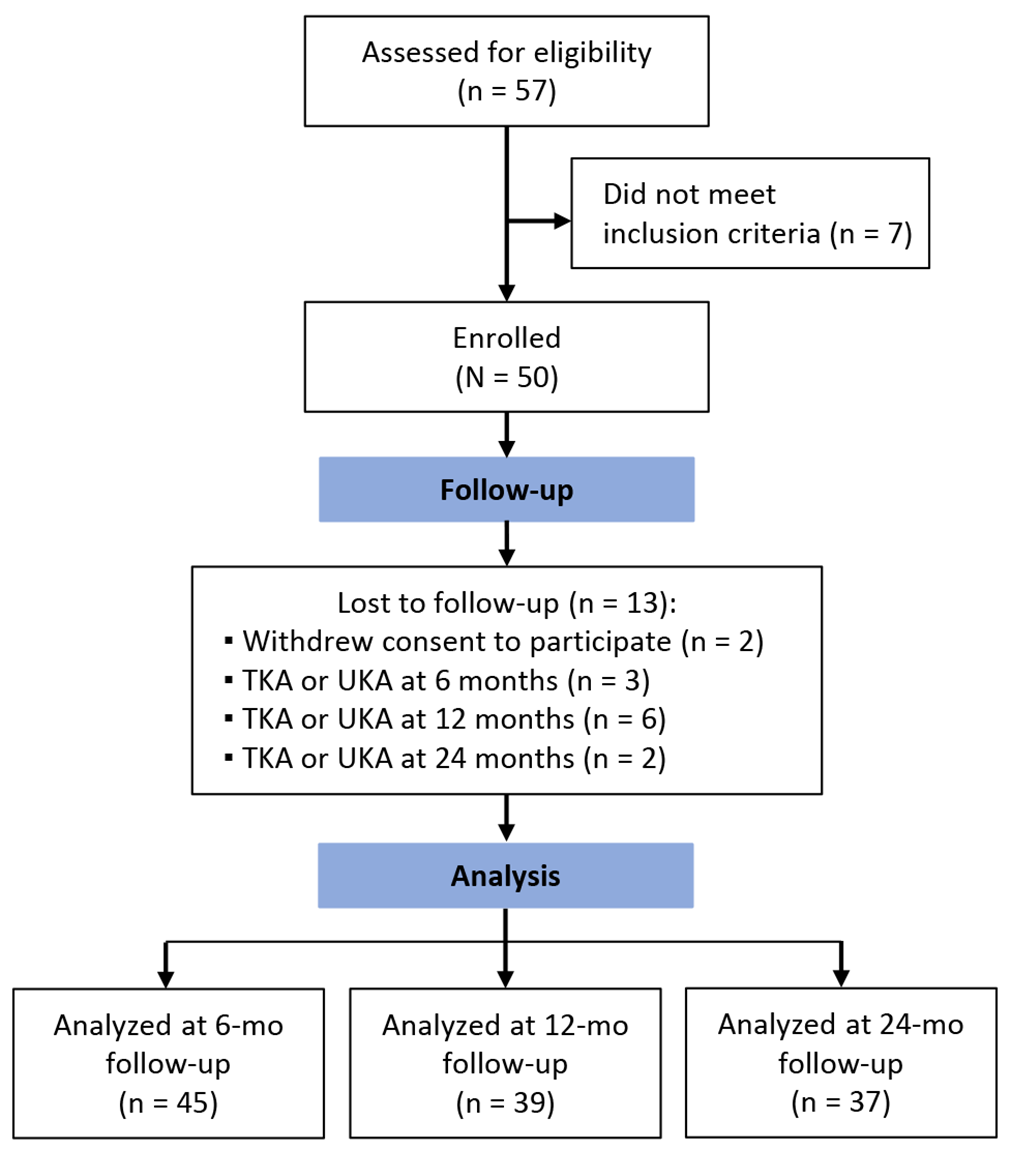
Flow diagram of the study. TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
At the 6-month follow-up, 27 patients experienced a 4-point reduction in the NRS pain score. The prevalence of success was 56.3% (27/48 [95% CI, 41.2%-70.5%]). Considering that 3 patients had an NRS score of 0 at the 6-month follow-up but had a baseline NRS value <4, the prevalence of success was 62.5% (30/48 [95% CI, 47.3%-76%]). Also, 38 patients (38/48 [79.2%] [95% CI, 65%-89.5%]) achieved a 2-point reduction in the NRS score at 6 months.
The mean preoperative NRS, WOMAC, and IKDC scores were 6.34 ± 2.09, 44.78 ± 16.72, and 30.88 ± 13.74, respectively. At the 6-month follow-up, the NRS and WOMAC scores improved to 2.39 ± 2.34 and 16.64 ± 14.98, respectively (P < .0001), whereas the IKDC score increased to 61.56 ± 20.63 (P < .0001). At the 12-month follow-up, the scores significantly improved to 1.13 ± 1.15, 10.33 ± 9.24, and 68.48 ± 15.53, respectively (P < .0001). These results were also confirmed at the 24-month follow-up, with an improvement in all the scores to 1.41 ± 1.61, 7.05 ± 8.09, and 70.49 ± 14.13, respectively (P < .0001). Additionally, the KSS (objective, satisfaction, and function sections) score significantly improved at the end of the follow up. Results showed that pain noticeably decreased and functional outcomes significantly improved after the procedure (Table 3 and Figure 3).
Clinical and Functional Outcomes According to the Follow-up Period a
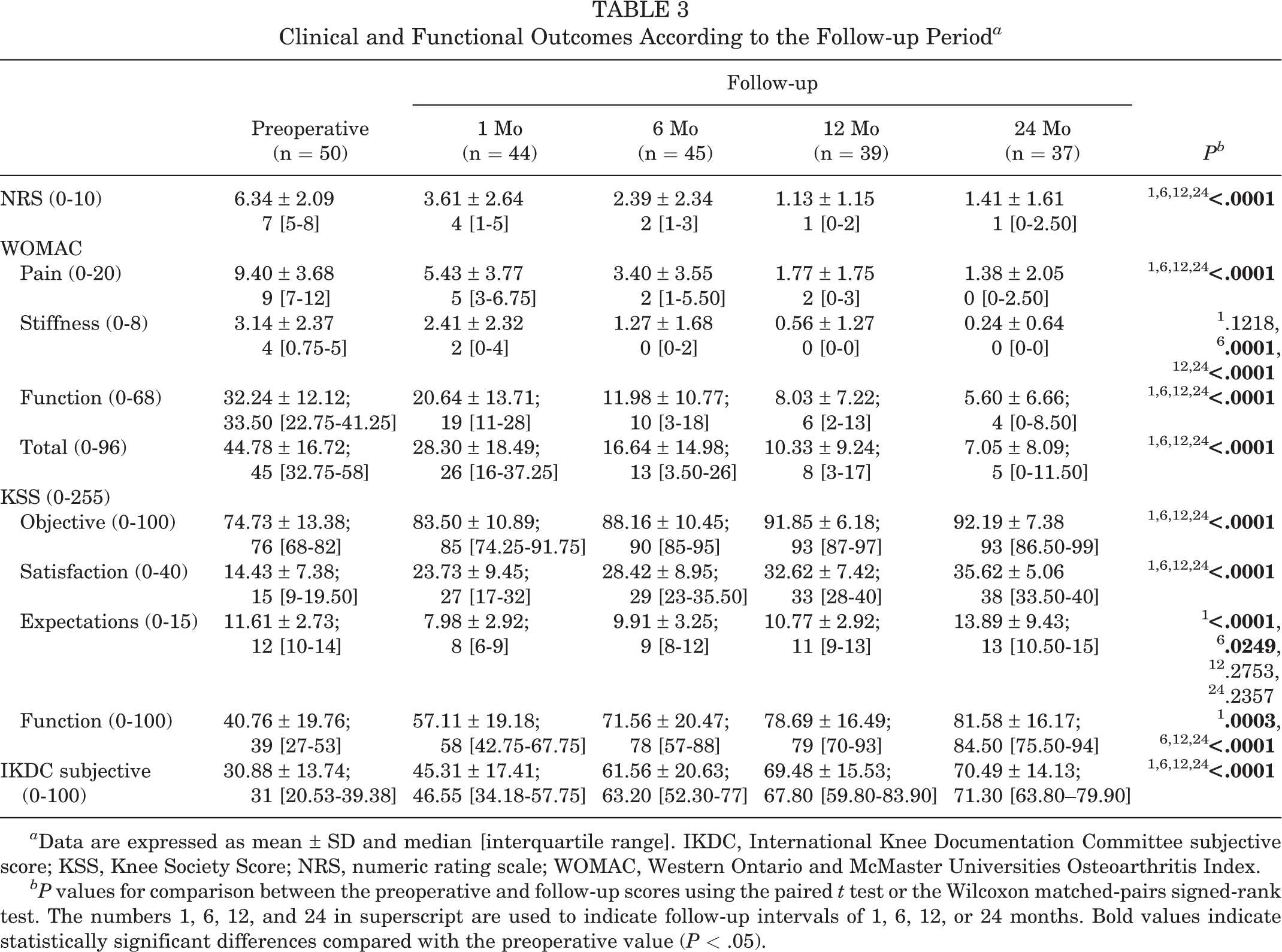
a Data are expressed as mean ± SD and median [interquartile range]. IKDC, International Knee Documentation Committee subjective score; KSS, Knee Society Score; NRS, numeric rating scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
bP values for comparison between the preoperative and follow-up scores using the paired t test or the Wilcoxon matched-pairs signed-rank test. The numbers 1, 6, 12, and 24 in superscript are used to indicate follow-up intervals of 1, 6, 12, or 24 months. Bold values indicate statistically significant differences compared with the preoperative value (P < .05).

Clinical and functional outcomes at 1-, 6-, 12-, and 24-month follow ups. Error bars show the SEM. IKDC, International Knee Documentation Committee subjective score; KSS, Knee Society Score; NRS, numeric rating scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index. Statistically significant differences compared with the preoperative value are presented as follows: *P < .05; *** P < .001; **** P < .0001.
Postoperative knee radiographs were available for 20 patients. They showed bone substitute integration in 20 patients. According to the Kellgren-Lawrence classification, knee OA did not progress in 16 patients, but it progressed in 4 patients and led to knee replacement—in 2 patients from grade 1 to grade 4; in 1 patient from grade 2 to grade 3; and 1 patient from grade 3 to grade 4. Postoperative MRIs were available for 20 patients. They showed a hypointense zone surrounded by a hyperintense signal at the injection site in T2 sequences. Leakage of injected material occurred extra-articularly in 1 patient and intra-articularly in 5 patients, which was immediately treated with arthroscopic debridement and irrigation.
Seven patients required hyaluronic or steroid injections during the follow-up. Total knee replacement was performed in 6 patients, whereas unicompartmental knee replacement was performed in 5 patients because of failure of pain reduction and OA progression. Further analysis of pain reduction at 6 months was performed in the subgroup of patients whose treatment failed and underwent knee replacement after >6 months. Among these 8 patients, only 3 (37.5%) achieved a 4-point reduction.
Discussion
The main finding of this study was that SCP reduced pain, as indicated by a minimum 4-point decrease in the NRS in 54% of patients at the 6-month follow-up. This result did not satisfy the study hypothesis, in which the 4-point NRS decrease was expected to be observed in 70% of the patients. Nevertheless, data demonstrated a statistically significant reduction in NRS pain values. In our series, 76% of patients achieved the MCID for the pain NRS of 2 points, 10 showing that they benefitted from the procedure. This is in accordance with available evidence reporting a mean improvement of pain on a visual analog scale of 4.3 to 7.2 points. 2,4,5,7,14 –16,19 At 2 years after surgery, 26 patients (52%) showed target pain reduction, indicating a continuity of the obtained results.
Data analysis showed an unexpected discrepancy between the considerable reduction in the NRS score and the relatively few patients who achieved a reduction of ≥4 points on the NRS. A possible explanation is that at the end of the follow-up period, some patients showed a marked pain reduction (≥4 points) and others had very poor results (<4 points). This finding could indicate a potential selection bias in patients’ selection, such as OA grade, age at the time of surgery, and the effect of concomitant arthroscopic procedures. Moreover, among the 23 patients who did not achieve a minimum 4-point pain reduction at the 6-month follow-up, it was possible to find some clinical benefits in 11 patients (47.8%). Three patients reached 0 points in the NRS at the 6-month follow-up, but they had a baseline NRS value <4 points. In addition, 4 patients achieved the target reduction of the NRS at the 12-month follow-up instead of the 6-month follow-up. Five patients showed a functional improvement in the KSS score despite an insufficient pain reduction.
Two patients (who reached 4 points NRS reduction) underwent KR within the 6-month follow-up due to progression of OA and functional limitation. Another 4 patients underwent KR within the 6-month follow-up due to the persistence of pain after the procedure, and functional limitation affected the quality of life despite achieving the goal of pain reduction. These results highlight the limit of the NRS score in describing the clinical symptoms of this disease. Nonetheless, at the same time, further analysis of the group undergoing prosthetic replacement revealed a higher mean NRS at the 6-month follow-up than the group that completed the follow-up with no need for subsequent surgeries (3.88 ± 2.53 vs 2.05 ± 2.20). Moreover, comparing the difference between the mean NRS value at the baseline and 6 months in the 2 groups, a lower improvement was found in patients who required a knee replacement (2.94 vs 4.33, respectively).
At the 6-month follow-up, the mean IKDC score showed an increase of 30.68 points compared with the preoperative value, confirming that patients could perform more intense physical activity. This result is in contrast with results reported by Cohen and Sharkey, 5 who found an increase of only 17.2 points during the same follow-up period, and results reported by Farr and Cohen, 7 who found an improvement of 22.4 points at a 6-month follow-up. In the present study, WOMAC scores were reduced from 44.78 ± 16.72 preoperatively to 10.33 ± 9.24 at 1 year after surgery, which is similar to the findings of Chua et al 4 (WOMAC score reduction from 47.8 preoperatively to 14.3 at 1 year postoperatively), demonstrating a lower perceived difficulty by patients in carrying out daily activities. Furthermore, the results of these 2 scores also improved at the 12- and 24-month follow-ups. The postoperative improvement in physical abilities as perceived by patients was therefore rapid and long-lasting.
The mean objective KSS significantly improved postoperatively (P < .001), although it was already high preoperatively because of the strict inclusion criteria that reserved the SCP procedure for the patients without joint instability and severe varus/valgus deviations. The slightly positive variation recorded by the subjective KSS, which investigates knee pain during some activities such as walking and climbing stairs, could suggest that a longer time is needed to reach a full improvement after this procedure. The KSS expectation, which is the most subjective part of the score, revealed a slight statistically significant difference at the 6-month follow-up compared with the baseline (P = .0249), 12-month (P = .2753), and 24-month follow-ups (P = .2357), but it is also influenced by other external factors. The KSS functional score supported the positive influence of SCP on knee functional outcomes.
No conclusions could be drawn from the few postoperative images collected. Regarding the partial result, postoperative radiographs showed OA progression in only 4 patients, but the short-term follow-up of the present study might not have allowed the detection of possible effects of this procedure on the natural history of OA. Postoperative MRI showed a hypointense zone surrounded by a hyperintense signal at the injection site in T2 sequences and a hypointense zone in T1 sequences, without any significant impact on the patient outcome. These findings could suggest an ongoing remodeling process in the treated areas. Histology would be necessary to confirm the actual changes in the bony tissue; however, it was not performed for ethical reasons. 29 patients underwent concurrent arthroscopic procedures, such as partial meniscectomy or free body removal. However, separately analyzing the group of patients who received a concomitant arthroscopic procedure (e.g. meniscectomy) and the patients who underwent only SCP followed by diagnostic arthroscopy, we found comparable results both in terms of pain (reduction to FU at 6 months of 3.25 points in the first group and 5 points in the second, but a reduction of 5.05 in the first and 5.43 in the second at 12-month FU which is confirmed at 24-month FU) both in terms of failures (6 in the first group and 5 in the second group).
Some complications have been reported after SCP, such as intra-articular and extra-articular leakage during injection and conversion to knee replacement, which might be due to inadequate indications such as diffuse OA. 16 In our study, intra-articular leakage occurred in 5 patients and extra-articular leakage in 1 patient who was immediately treated with debridement and irrigation during the procedure, with no sequelae in the immediate postoperative period or during the follow-up. Some patients reported pain 3 to 5 days after the procedure, which was controlled by analgesic therapy. Seven patients required further conservative treatment such as intra-articular injections with corticosteroids or hyaluronic acid due to the persistence of symptoms. SCP failed in 11 patients who required knee replacement within the follow-up period (6 patients, total knee replacement; 5 patients, unicompartmental knee replacement). The failure rate observed in this study was 22.9%, which is in agreement with other studies 5,14 –16 in the literature whose failure rates ranged between 12.5% and 30%. Early failures during the first 6 months of the follow-up (8 patients) occurred in patients with relatively high-grade OA. Also, a 4-point NRS reduction was achieved in only 37.5% of this population at the 6-month follow-up, confirming that the SCP procedure is not effective in patients with advanced OA, as reported by Chatterjee et al, 3 and that when a failure occurs, it happens early.
It is also important to consider that SCP does not represent a contraindication to the implantation of a prosthesis, and in our case series, no additional technical difficulties were found in performing prosthetic replacement after SCP, according to previous studies that reported that SCP did not affect the execution of subsequent prosthetic surgery. 28
At the 2-year follow-up, 37 of 50 (74%) patients in this sample avoided the implantation of an arthroplasty either temporarily or permanently, suggesting that this treatment can be an option to postpone knee replacement in OA when conservative treatments fail.
Limitations
There are some limitations in this study. First, the lack of minimal pain score as an inclusion criterion prevented some patients from reaching the primary goal of the study, despite an excellent outcome. Second, the lack of a control group did not allow the evaluation of the effectiveness of SCP as a treatment for BMLs compared with placebo or other therapeutic strategies already performed in clinical practice (eg, bisphosphonates). Third, concomitant knee arthroscopy may have influenced the final results, possibly because of the placebo effect 23 or the concomitant procedure’s effect on pain, such as partial meniscectomy or loose body removal. Finally, the lack of full radiological data and the short-term follow-up gave only partial information about BML evolution after the procedure. Since a histological analysis of biopsy samples was not available in this study, it was impossible to correlate the new signals on MRI and the real bone remodeling process.
Conclusion
After the SCP procedure, about half of the patients in the study sample reached 4 points of NRS reduction at the 6-month follow-up, a percentage lower than that predicted by the hypothesis and insufficient to draw conclusions on the efficacy of this procedure. However, about 80% of patients achieved the MCID at the 6-month follow-up and less than 1/4 of the sample underwent prosthetic replacement.
Footnotes
Final revision submitted January 11, 2023; accepted January 25, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.R. has received consulting fees from DePuy, IBSA Group, Medacta, Microport, and Olympus and nonconsulting fees from B. Braun, LIMA, and Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico–Milano Area 2 (ref No. 610/2019).