
Abstract
Purpose
This study aimed to compile available data in medical literature about subchondral calcium phosphate injection, comparing results obtained with this technique, as well as indications, complications, and other important factors in treatment of bone marrow lesions.
Designs
A literature review using PubMed and Medline database in order to identify works with terms “subchondral calcium phosphate injection,” “ subchondroplasty®,” “bone marrow lesion,” and “knee.” Eight relevant articles were found.
Results
A total of 164 patients with bone marrow lesion mainly on femoral condyle and tibial plateau recovered with significant functional improvement of knee after subchondral calcium phosphate treatment. Although 25% of them still had some type of pain complaint, they also showed improvement. There were few complications reported and return to activities occurred after 3 months on average.
Conclusions
Few studies evaluate the result of using subchondral calcium phosphate injection technique. However, all presented favorable results regarding pain and improvement of knee function. In addition, within 2 years, there was a 70% reduction in conversion to total knee arthroplasty in patients with previous surgical indication who choose calcium phosphate treatment.
Introduction
Changes in subchondral bone are currently recognized as an important factor in the osteoarthritic process.1,2 Bone marrow lesions (BML), or bone edema, are characterized by a histological alteration of the subchondral bone, which may progress with pain, joint surface deformity and accelerated progression of osteoarthritis.3-6 Histological changes are not limited only to edema, but includes also fibrosis, necrosis of bone marrow, microfractures of bone trabeculation, and deficient mineralization, which leads to production of abnormal bone remodeling to form a bone with normal characteristics.7,8
Accelerated progression of osteoarthrosis is common in patients with BML, which may increase chance of total knee arthroplasty (TKA) by up to 9 times within 3 years.9,10 The search for adjuvant therapies capable of altering the evolution of a subchondral lesion becomes important for preservation of the knee joint.
Subchondral calcium phosphate injection consists of application of a synthetic calcium-phosphate-based bone substitute at the BML site. It aims to improve the structural quality of affected subchondral bone and provide a local bone remodeling, seeking to prevent bone collapse and progression of arthritis.11-15
The purpose of the present study is to identify evidence produced by studies related to the subject, synthesizing data obtained in medical literature on indications, treatment, complications, and results of subchondral calcium phosphate injection technique for BML.
Methods
Search Strategy
Electronic database PubMed and Medline were used to search for relevant studies on subject. Primary term used was “subchondral calcium phosphate injection” and “subchondroplasty®” and secondary terms “bone marrow lesion” and “knee.” English studies were searched without time filtering; however, all published works are less than 5 years from date of publication to date.
Study Selection
All studies that approached subchondral calcium phosphate injection as a treatment technique for BML, presenting respective results obtained with technique were evaluated. Studies were checked first for duplicates and then displayed by title, summary, methods, and results. Each study was submitted to a stepwise screening process by each author.
Data Extraction
All the data obtained in studies were compiled in a table, in which similar and different aspects were analyzed and identified: number of patients, indications, contraindications, product used, site of injury, technique used, classification, return to activities, complications and results obtained, among other data evaluated ( Table 1 ).
Characteristics of Selected Studies on Subchondral Calcium Phosphate Injection, Showing the Number of Patients Involved in Each Study, Indications, Contraindications, Product Used, Location of the Lesion, Expansions of Indications, Evaluation Scores Used, Complications, Return to Activities and Weightbearing, and Results Found.
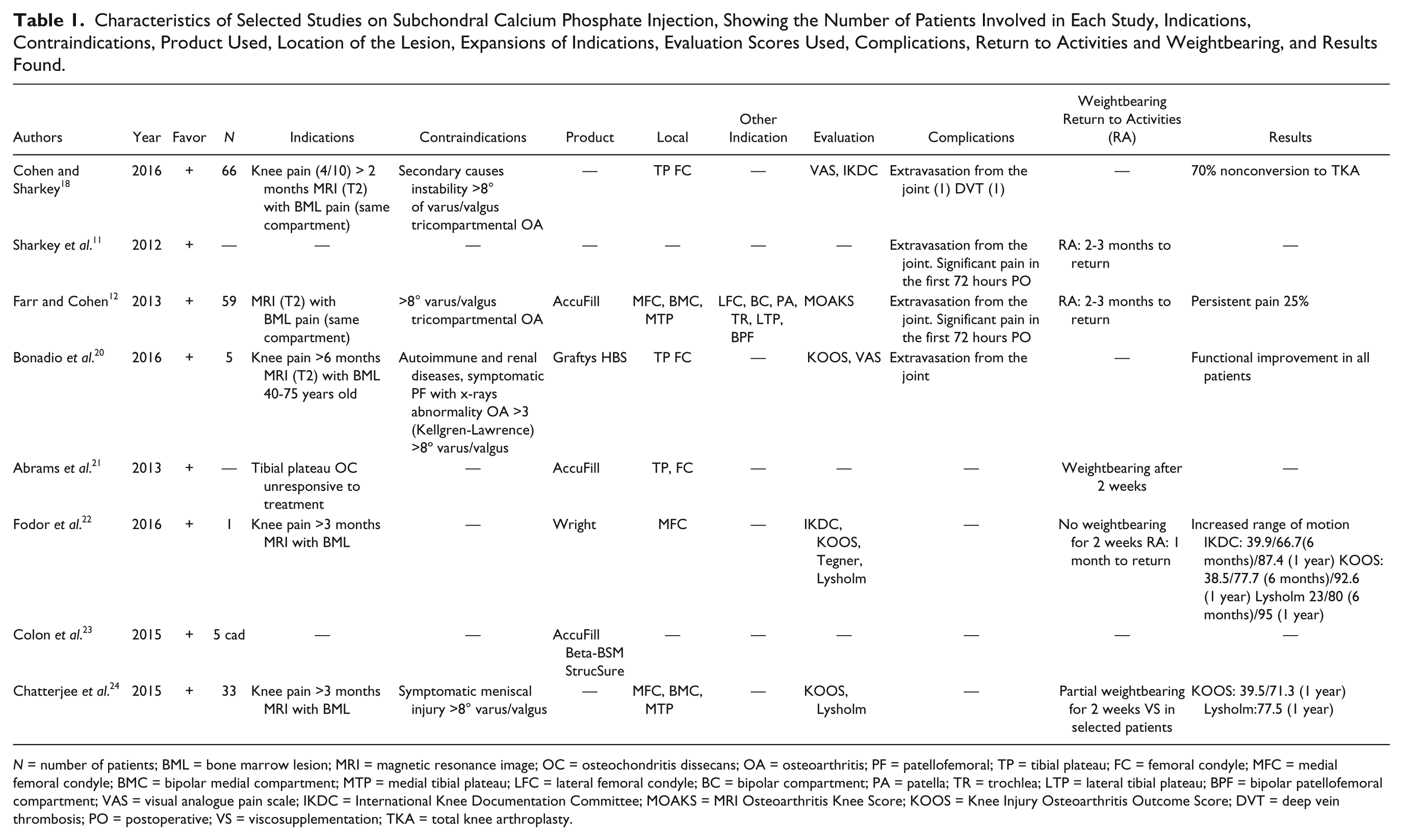
N = number of patients; BML = bone marrow lesion; MRI = magnetic resonance image; OC = osteochondritis dissecans; OA = osteoarthritis; PF = patellofemoral; TP = tibial plateau; FC = femoral condyle; MFC = medial femoral condyle; BMC = bipolar medial compartment; MTP = medial tibial plateau; LFC = lateral femoral condyle; BC = bipolar compartment; PA = patella; TR = trochlea; LTP = lateral tibial plateau; BPF = bipolar patellofemoral compartment; VAS = visual analogue pain scale; IKDC = International Knee Documentation Committee; MOAKS = MRI Osteoarthritis Knee Score; KOOS = Knee Injury Osteoarthritis Outcome Score; DVT = deep vein thrombosis; PO = postoperative; VS = viscosupplementation; TKA = total knee arthroplasty.
Results
Initial research resulted in 10 articles found, of which, after analysis of title and abstract, we selected and included 8 studies, extracting data for compilation in a table. Results of evaluated data were subdivided into topics:
Number of patients
Number of patients evaluated in studies varied from 5 to 66. Most of the studies present a small series. A total of 164 patients were evaluated in the 8 studies analyzed.
2. Indications
Indications for subchondral calcium phosphate injection in BML were: moderate to severe pain for more than 2 to 6 months; presence of BML associated with pain in the same compartment of the lesion; stable osteochondritis dissecans injuries in tibial plateau with nonresponse during conservative treatment. Age to indicate the surgical treatment ranged from 40 to 75 years.
3. Contraindications
Contraindications for subchondral calcium phosphate injection in BML were: secondary causes for pain diagnosed; loss of limb function; knee instability; angular deformities in varus or valgus greater than 8°; tricompartmental osteoarthrosis; autoimmune diseases; dialytic renal insufficiency; and anterior pain with patellofemoral alteration identified by imaging examination.
4. Substitute bone paste
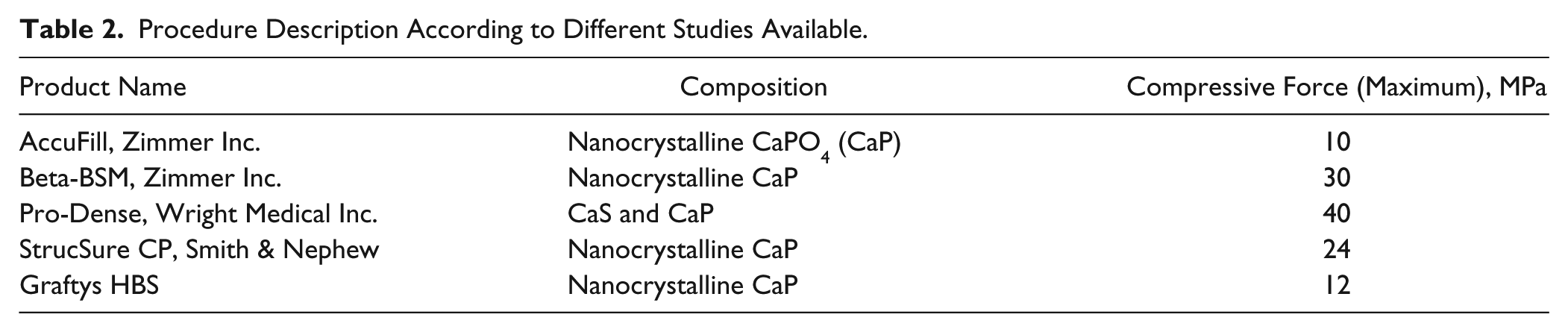
All bone substitutes used in paste are made from calcium phosphate. In evaluated studies following brands were used: AccuFill (Zimmer Inc., USA), Graftys HBS (Graftys, France), Wright Pro Dense (Wright, USA), Beta-BSM (Zimmer Inc., USA), and StrucSure (Smith & Nephew, UK). Composition and maximum compression force of each of them are presented in Table 2 .
5. Location of lesion
Bone substitution was applied to lesions identified mainly in medial tibial plateau and medial femoral condyle. Other regions treated, however, were lateral tibial plateau, lateral femoral condyle, femoral trochlea, patella, and combined in presence of mirror lesions: femoral condyle and tibial plateau, patella, and femoral trochlea.
6. Technique
Initially, evaluation should be performed with magnetic resonance imaging (MRI), in order to define location, size, and depth of lesion.
Procedure Description According to Different Studies Available.
In the surgical center, under anesthetic effect (general or spinal anesthesia), a 7G cannula, with its own syringe for sulfate mixing (varies according to each manufacturer), is introduced 5 to 10 mm below fluoroscopy-guided joint surface in the central region of lesion. Calcium phosphate (CaP) slurry is injected to fill injured area, which may range from 5 to 16 mL. Intraoperative image control is important to ensure that there is no extravasation of substrate to the joint or soft tissue.
To treat a tibial lesion, a navigational guide can be used by placing it on anterior portion of knee so that access portals of guide are on subchondral bone (5 to 10 mm below articular surface). Guide should mark tibial plateau and posterior border of tibia. Tibial tubercle can be used as a stabilizer for the navigation frame. Once the guide is in place, trajectory that has been predetermined by the 3 planes in the MRI can be used to accurately place a fenestrated cannula in the BML. Placement of cannula is confirmed in orthogonal fluoroscopic views. The inner trocar from the cannula can be removed and the syringe with synthetic bone substitute is injected into the cannula. By applying constant digital pressure, bone substitute is injected into area of subchondral defects. The cannula can be rotated to direct the fenestrations toward or away from the articular surface ( Fig. 1 ). Bone substrate is continued to be injected until a dark flush is visible on fluoroscope which mimics BML identified on MRI. Arthroscopic evaluation is used to confirm proper injection of CaP without extravasation in joint space.
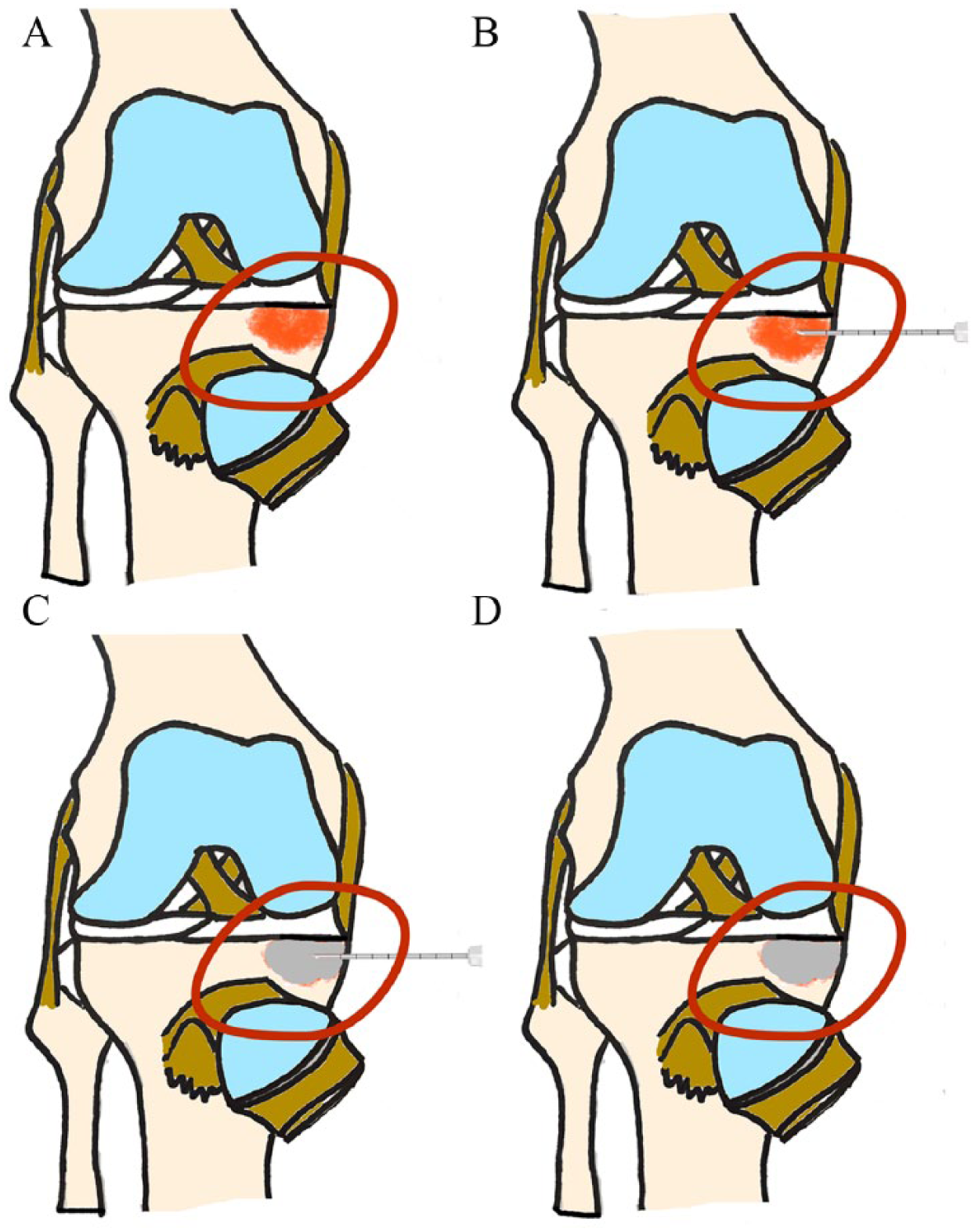
(
To treat a femoral lesion, a navigation guide can be used again and placed on femoral condyle to define articular surface of condyle and confirm location of the injection. Similar to the tibial lesion, fluoroscopy is used to confirm proper location of placement and injection of CaP. Based on location of lesion, cannula fenestrations can be directed to articular surface, if necessary. As with tibial lesion, surgeon needs to confirm that there is no extravasation of phosphate in joint, placing material exactly on lesion and confirming placement with arthroscopy. As CaP is hydrophilic, any material can be washed from joint with arthroscope and shaver.
Incision is sutured and dressing simple. Postoperative immobilization was not performed, and total load was released as tolerated 1 day after surgery ( Table 3 ).
7. Evaluation questionnaires
Composition and Biomechanical Characteristics of All Different Calcium Phosphate.
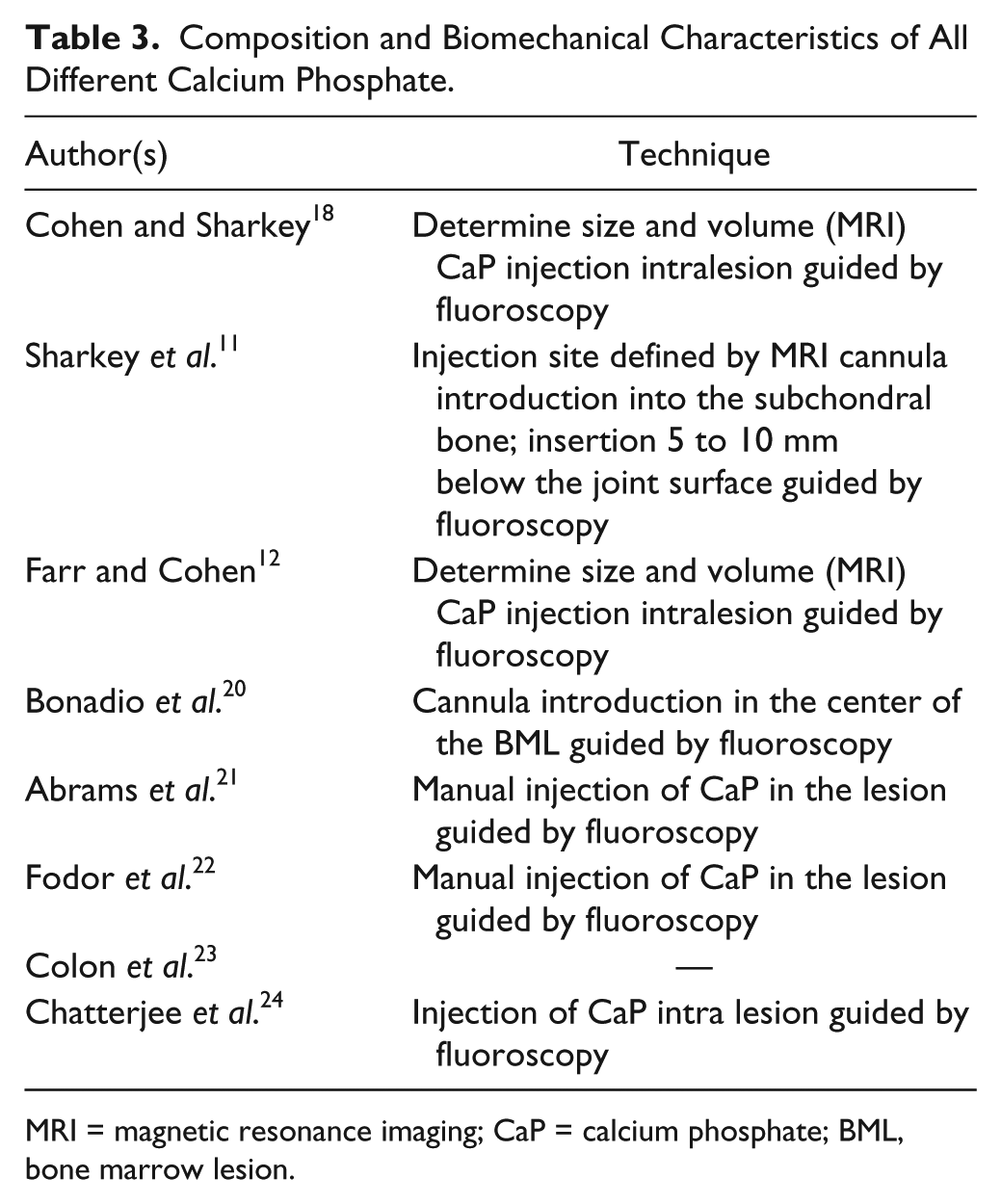
MRI = magnetic resonance imaging; CaP = calcium phosphate; BML, bone marrow lesion.
Visual analog scale (VAS) was used to assess subjective pain pre- and postoperation.16-21 To evaluate knee function, IKDC (International Knee Documentation Committee), KOOS (Knee Injury and Osteoarthritis Outcome Score), Tegner and Lysholm scores were used.18,20-24 The MOAKS score (MRI Osteoarthritis Knee Score) was used to evaluate the MRI lesion. 20
8. Complications
Subchondral calcium phosphate injection seems to be a very safe procedure with very few complications described. The most common complaint was disproportionate knee pain that improved completely within 72 hours after procedure. In the studies evaluated, extravasation of product into joint (2 patients) and deep vein thrombosis of affected limb (one patient) were also mentioned. No case of infection was reported after procedure.
9. Postoperative management
Some authors release total load as tolerated day after surgery, but, on average, there was a load restriction, as tolerated, with use of crutches, for a maximum of 2 weeks.
Physical therapy is started within 2 weeks of surgery and persists for 4 to 8 weeks after surgery. Significant reduction of pain and return to full activity occurs after 2 to 3 months of surgery.
10. Results
The studies evaluated showed significant functional improvement of knee, although Farr and Cohen 12 found that 25% of them still remained with some kind of pain complaint.
There was a 70% reduction in need for total knee arthroplasty (TKA) in patients assessed after 2 years of subchondral calcium phosphate injection. In the study with the largest number of patients, 66, use of this technique was proposed in patients who sought service with indication for TKA, with improvements in pain scores (VAS) and knee function (IKDC). 18
Discussion
Subchondral calcium phosphate injection technique for treatment of BML was used in 8 studies evaluated in literature. In all cases, this technique proved to be favorable to treat BML, with satisfactory results.
Since it is a simple procedure, filling of bone defect with calcium phosphate seems to be an alternative in an attempt to avoid evolution of bony edema to a more severe degenerative process of knee. Coupled with few complications described, interest in knowing if this modality actually assists in treatment of lesion stimulates that new studies be done, with better methodology and a larger sample of patients evaluated.
Calcium phosphate–based bone substitute is a graft option in bone defects.13-15 In this function, biphasic calcium phosphate ceramics show good results as osteoinducer and osteoconductor. Such properties may contribute to balance in bone mineralization that was lost in areas of BML, modifying evolution of pathology.16,17 Biphasic calcium phosphate ceramics have degradation more similar to autologous bone, unlike hydroxyapatite, which has a longer time. 20
Most of the studies described evaluate patients who underwent follow-up procedure ranging from 6 to 24 months. It is noticed that type of patients and indication is still quite varied, and that follow-up time is still short. However, it is interesting to note that in all studies, after at least 6 months, there was clinical and functional improvement, and appearance of lesion on imaging examination (MRI).18,20-24
Studies show that the presence of BML in some patients with osteoarthritis is associated with pain, disease progression, joint deformity and consequently evolution to degenerative stages that allow indication of substitution surgery, such as total or partial knee arthroplasty.3,5,10 However, cases when a patient is young, an alternative treatment option may be beneficial. Bone substitutes can be a solution to improve symptoms and even reduce edema, avoiding or postponing evolution of arthrosis and consequently delaying joint replacement, which was demonstrated by Cohen et al. In their studies, there was a 70% reduction in patient’s desire to undergo TKA after 2 years of subchondral calcium phosphate injection treatment. All patients had initial indication for joint replacement. Even so, it was chosen to fill the lesion with calcium phosphate. This very relevant data is promising, but it requires broader assessments, with a larger number of patients, and standardization for indication.12,18-23
Calcium phosphates commercially available to perform subchondral calcium phosphate injection have different properties, such as maximum compressive strength supported varying from 0.000025 MPa to 55 MPa; preparation time of product, varying from 3 to 10 minutes; and time to use (working time) of calcium phosphate preparation varying from 2 to 15 minutes, implying directly on final result. 23
Different characteristics of available products also hamper standardization of results, and consequently, comparison between them. In addition, scales of evaluation of results varied widely between authors, associated with a lack of control group, which, although all showed improvement of knee function and pain, makes it impossible to quantify this improvement and compare this issue between studies.
Limitations
One of the most important limiting factors founded in all different studies presented is the lack of standardization to evaluate results obtained. In addition, no study compared technique with another surgical treatment, like knee arthroscopy, or with longer follow-up of 2 years ago. Finally, number of patients evaluated still needs to be broader for more significant results.
Conclusion
Although there are many commercially available calcium phosphate products for the treatment of subchondral BMLs, there are relatively few studies. While there are reports of decreased pain, improved function and a delay in TKA, there remains a need for high level of evidence studies with appropriate controls (including active controls) to understand the optimal formulations, techniques, and indications.
Footnotes
Authors’ Note
This study was done at the Centro de Traumatologia do Esporte, Universidade Federal de São Paulo, São Paulo, Brazil.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.