
Abstract
Background:
The extent to which concomitant osteotomy provides an improvement in clinical outcomes after cartilage repair procedures is unclear.
Purpose:
To review the existing literature to compare clinical outcomes of patients undergoing cartilage repair of the tibiofemoral joint with versus without concomitant osteotomy.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines by searching PubMed, the Cochrane Library, and Embase to identify studies that directly compared outcomes between cartilage repair of the tibiofemoral joint alone (group A) versus cartilage repair with concomitant osteotomy (high tibial osteotomy [HTO] or distal femoral osteotomy [DFO]) (group B). Studies on cartilage repair of the patellofemoral joint were excluded. The search terms used were as follows: osteotomy AND knee AND (“autologous chondrocyte” OR “osteochondral autograft” OR “osteochondral allograft” OR microfracture). Outcomes in groups A and B were compared based on reoperation rate, complication rate, procedure payments, and patient-reported outcomes (Knee injury and Osteoarthritis Outcome Score [KOOS], visual analog scale [VAS] for pain, satisfaction, and WOMAC).
Results:
Included in the review were 5 studies (1 level 2 study, 2 level 3 studies, 2 level 4 studies) with 1747 patients in group A and 520 patients in group B. The mean patient ages were 34.7 and 37.5 years in groups A and B, respectively, and the mean lesion sizes were 4.0 and 4.5 cm2, respectively. The mean follow-up time was 44.6 months. The most common lesion location was the medial femoral condyle (n = 999). Preoperative alignment averaged 1.8° and 5.5° of varus in groups A and B, respectively. One study found significant differences between groups in KOOS, VAS, and satisfaction, favoring group B. The reoperation rates were 47.4% and 17.3% in groups A and B, respectively (P < .0001).
Conclusion:
Patients undergoing cartilage repair of the tibiofemoral joint with concomitant osteotomy might be expected to experience greater improvement in clinical outcomes with a lower reoperation rate compared with those undergoing cartilage repair alone. Surgeons preparing for cartilage procedures of the knee joint should pay particular attention to preoperative malalignment of the lower extremity to optimize outcomes.
Keywords
Focal chondral defects of the knee joint are a common cause of musculoskeletal morbidity, with a prevalence of more than 60% in patients undergoing knee arthroscopy. 13 If nonoperative management fails, patients may undergo a variety of surgical options to treat cartilage lesions. 8 Despite the satisfactory results demonstrated by these procedures, patients may not do well. One study 14 found a failure rate of 18.5% in patients undergoing autologous chondrocyte implantation (ACI) and 17.1% in patients undergoing microfracture during an average follow-up of 7 years.
Various factors influence the cartilage regeneration potential that are patient-specific or specific to the native knee joint. In addition to the isolated cartilage defect, other factors such as meniscal status, ligamentous instability (mainly the anterior cruciate ligament [ACL]), and lower extremity malalignment should be considered. If all possible influential factors are not corrected, patient outcomes may be compromised or treatment with cartilage restoration may fail. 15 Osteotomies, including high tibial osteotomy (HTO) and distal femoral osteotomy (DFO), can reduce contact pressure on the implanted graft, normalize mechanics, and significantly unload the affected compartment of the knee, contributing to improved clinical outcomes and superior graft survivorship. 6 Despite some studies examining the effects of cartilage repair with or without osteotomy, 16,17,26 the extent to which concomitant osteotomy provides an improvement in clinical outcomes after cartilage restoration procedures is unclear.
The purpose of this systematic review was to compare clinical outcomes of patients undergoing cartilage repair of the tibiofemoral joint with versus without concomitant osteotomy. The authors hypothesized that patients undergoing combined cartilage repair and realignment would have superior clinical outcomes versus cartilage repair alone.
Methods
This systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using a PRISMA checklist. Two independent reviewers (J.D., S.M.F.) searched PubMed, Embase, and the Cochrane Library from inception up to May 9, 2022. The electronic search strategy used was as follows: osteotomy AND knee AND (“autologous chondrocyte” OR “osteochondral autograft” OR “osteochondral allograft” OR microfracture). A total of 586 studies were reviewed by title and/or abstract to determine study eligibility based on inclusion criteria. Furthermore, reference lists for studies that met inclusion criteria were reviewed to see if any further studies were identified that met inclusion criteria. In cases of disagreement, a third reviewer (M.J.K.) made the final decision.
Inclusion criteria included clinical studies that directly compared outcomes between cartilage repair of the tibiofemoral joint alone versus cartilage repair of the tibiofemoral joint with concomitant osteotomy (HTO or DFO). Studies were excluded if they were nonhuman studies, studies unrelated to the knee, noncomparative studies, and studies that evaluated cartilage repair/osteotomy of the patellofemoral joint.
Data extraction from each study was performed independently and then reviewed by a second author (M.J.K.). There was no need for funding or a third party to obtain any of the collected data. Risk of bias was assessed according to the ROBINS-I (Risk of Bias in Nonrandomized Studies of Interventions) risk of bias tool, 23 which incorporates an assessment of bias due to confounding, selection of participants, deviations from intended interventions, completeness of outcome data, selection of outcomes reported, and other sources of bias. The level of intraobserver agreement between reviewers was determined by calculating the Cohen kappa (κ), in which a value <0.20 indicates poor agreement; 0.21 to 0.40, fair agreement; 0.41 to 0.60, moderate agreement; 0.61 to 0.80, good agreement; 0.81 to 1.00, very good agreement. 18
Reporting Outcomes
Outcomes assessed included patient-reported outcomes (PROs), reoperation rate, complication rate, and procedure payments. PROs included the Knee injury and Osteoarthritis Outcome Score (KOOS), 22 the visual analog scale (VAS) for pain, satisfaction, and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). 21 Satisfaction was measured by 1 study 10 by a 4-item score (not satisfied, partially satisfied, satisfied, or very satisfied).
Study Methodology Assessment
The Modified Coleman Methodology Score (MCMS) 9 was used to evaluate study methodology quality. The MCMS has a scaled potential score ranging from 0 to 100. Scores ranging from 85 to 100 are excellent; 70 to 84, good; 55 to 69, fair; and <55, poor. The primary outcomes assessed by the MCMS are study size and type, follow-up time, attrition rates, number of interventions per group, and proper description of study methodology.
Statistical Analysis
A weighted average was calculated for numerical characteristics (age, follow-up, sex, body mass index [BMI], and lesion size).
Results
Five studies 1,4,7,10,19 met the inclusion criteria and were included in the systematic review (Figure 1). A total of 2267 patients were included across the studies: 1747 patients underwent cartilage repair alone (group A) and 520 patients underwent cartilage repair with concomitant osteotomy (group B). The mean patient ages in groups A and B averaged 34.7 and 37.5 years, respectively, and the mean lesion sizes were 4.0 and 4.5 cm2, respectively. The mean follow-up time was 44.6 months. The average BMI was 27.0, and 53.2% of patients were men (Table 1). A total of 358 patients underwent HTO and 3 patients underwent DFO (Table 2). The 2 most common cartilage procedures were ACI (n = 883, 39.0%) and osteochondral allograft transplantation (n = 765, 33.7%). The preoperative alignment, which was reported in only 2 studies, averaged 1.8° and 5.5° of varus in groups A and B, respectively. The most common lesion location was the medial femoral condyle (n = 999, 44.1%).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.
Characteristics of the Included Studies a

a Group A = cartilage repair alone. Group B = cartilage repair with osteotomy. LOE, level of evidence; NR, not reported.
b Reported as weighted means.
Cartilage Lesion Characteristics a

a Group A = cartilage repair alone. Group B = cartilage repair with osteotomy. ACI, autologous chondrocyte implantation; BMS, bone marrow stimulation; D, debridement; DFO, distal femoral osteotomy; HTO, high tibial osteotomy; M, multiple therapies; MFC, medial femoral condyle; NR, not reported; O, other; OCA, osteochondral allograft transplantation.
b Reported as weighted means.
Patient-Reported Outcomes
Two studies 4,10 reported results of the KOOS. In 1 study, 10 patients in group B had a significantly higher postoperative KOOS (81.75 ± 14.22) compared with patients in group A (74.40 ± 16.57) at the final follow-up (P = .02). In the other study, 4 no significant differences were found between groups at the final follow-up (P > .05). WOMAC scores were reported in 1 study, 4 with no significant differences between the 2 groups at the final follow-up (P > .05). VAS pain scores were reported in 1 study, 10 with significantly lower scores for patients in group B (2.02 ± 1.98) compared with group A (3.20 ± 2.18) at the final follow-up (P = .003). Satisfaction was reported in 1 study, 10 and results indicated a significantly higher level of satisfaction in group B compared with group A at the final follow-up (P = .015).
Reoperation Rate
Three studies 4,7,19 assessed reoperation rate at the final follow-up (Table 3). In 1 study, 4 revision surgery was indicated in patients with persistent pain related to the implant site in combination with sign of ACI graft failure or ACI graft complication on magnetic resonance imaging (MRI). In another study, 19 revision was performed in cases of graft failure with partial knee arthroplasty, total knee arthroplasty, or revision cartilage repair. All 3 studies found significant differences between groups, favoring group B. One study 7 found no significant differences between groups A and B with regard to rate of conversion to arthroplasty (P = .68).
Reoperation Rates a
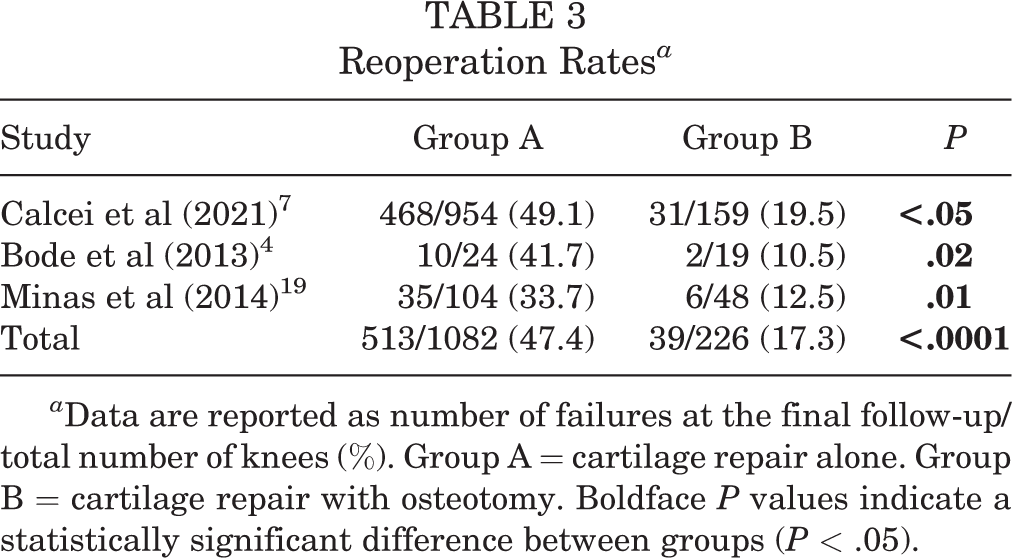
a Data are reported as number of failures at the final follow-up/total number of knees (%). Group A = cartilage repair alone. Group B = cartilage repair with osteotomy. Boldface P values indicate a statistically significant difference between groups (P < .05).
Complication Rate
One study 7 reported complication rates and found no significant differences between ACI alone (3.0%) versus ACI with concomitant osteotomy (4.5%) (P = .52) and OCA alone (2.5%) versus OCA with concomitant osteotomy (3.3%) at the final follow-up (P = .69).
Procedure Payments
One study 7 reported total day of surgery payments and found no significant differences between ACI alone versus ACI with concomitant osteotomy (P = .22) and OCA alone versus OCA with concomitant osteotomy (P = .13).
Modified Coleman Methodology Score
Table 4 shows the MCMS scores from the 5 included studies. One study 19 received an excellent score. Three studies 1,4,10 received a good score. One study 7 received a fair score.
Modified Coleman Methodology Score a
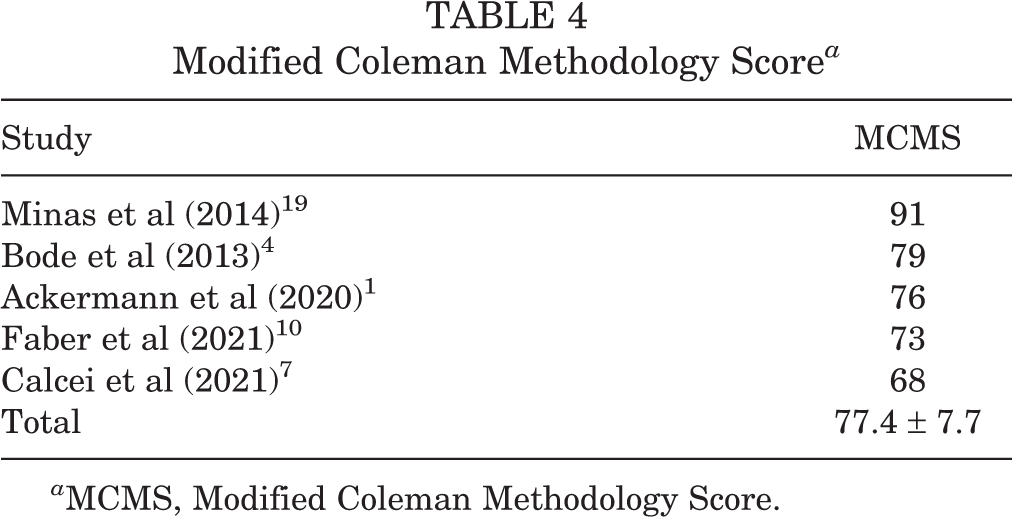
a MCMS, Modified Coleman Methodology Score.
Methodologic Quality Assessment
The results of the methodologic quality assessment of the 5 nonrandomized studies using the ROBINS-I risk of bias tool are presented in Figure 2. All 5 studies 1,4,7,10,19 showed a moderate risk of bias due to confounding, as there were no prognostic variables that predicted baseline intervention and no patients that switched between interventions during the study period. No studies excluded eligible patients or used variable follow-up times based on intervention (low risk of bias), no studies deviated from the intended intervention (low risk of bias), and all studies clearly classified treatment type (low risk of bias). While all 5 studies 1,4,7,10,19 described using nonblinded methods for outcome assessment, none described differences in postoperative rehabilitation or outcome measurement protocols between groups (moderate risk of bias). No studies showed bias due to missing data (low risk of bias). All 5 studies 1,4,7,10,19 demonstrated serious risk of bias in measurement of outcomes as neither physicians nor patients were blinded to treatment type. Finally, no studies showed bias due to selective reporting (low risk of bias). The κ value was 0.83, reflecting very good agreement between reviewers.
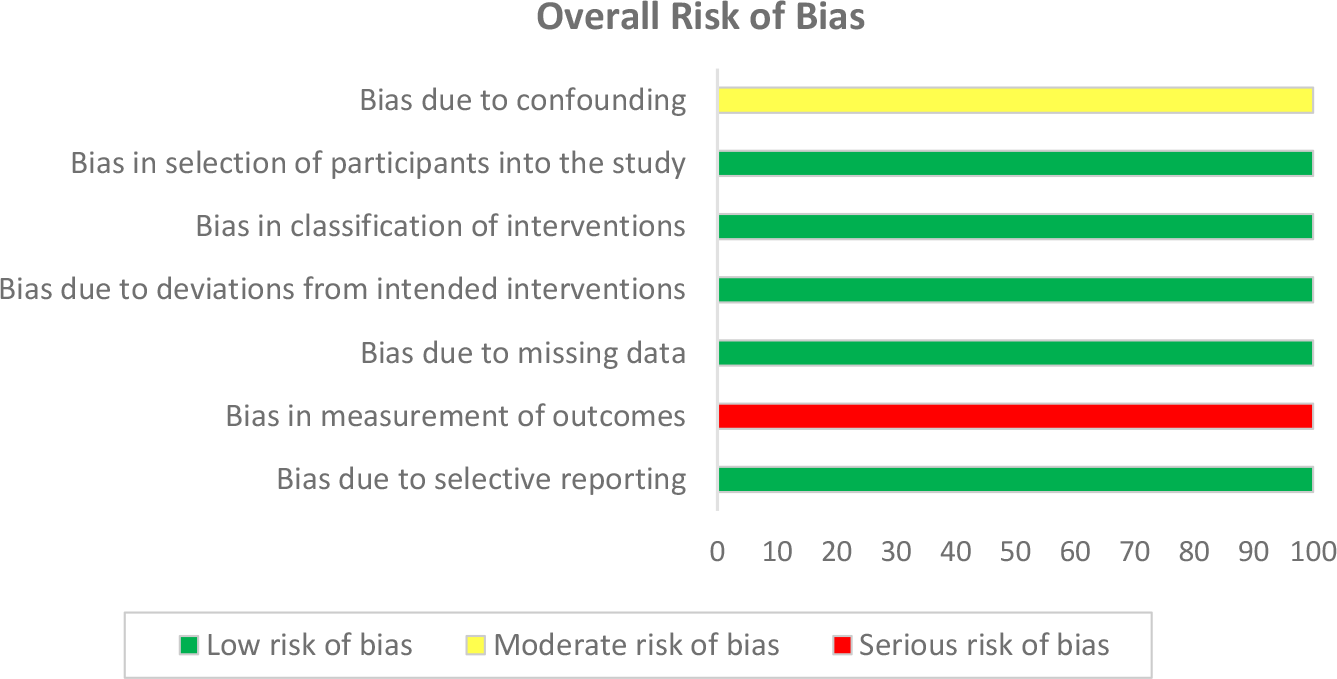
Risk of bias represented as a percentage across all included studies.
Discussion
Based on the results of our systematic review, we found a significantly lower reoperation rate for patients undergoing cartilage repair with concomitant osteotomy compared with cartilage repair alone. In addition to lower reoperation rates, we also found superior PROs among patients undergoing cartilage repair with concomitant osteotomy in the domains of both function and pain at the short-term follow-up. Furthermore, no significant differences were found between groups with regard to complication rates and procedure payments.
A previous systematic review from 2013 25 compared clinical outcomes of patients undergoing isolated patellofemoral ACI versus those undergoing ACI combined with patellofemoral realignment. The study included 366 patients and found significant improvements in multiple clinical outcomes favoring the combined treatment group, with no significant difference between groups in the rate of postoperative complications. Moreover, another systematic review published in 2020 20 concluded that when osteotomies were performed in conjunction with cartilage procedures, return to work occurred more quickly, as did an increased rate of healing at the chondral lesion site. Finally, a literature review conducted in 2017 24 concluded that cartilage-restoration procedures performed in conjunction with HTO can lead to improved cartilage regeneration. These findings parallel the results of the current systematic review.
Among the factors associated with cartilage repair success after concomitant osteotomy, the most important seems to be improvement of the mechanical environment. To maintain overall joint homeostasis, hyaline articular cartilage requires mechanical stimulation for the activation of regulatory pathways to preserve extracellular matrix quality and chondrocyte function. 1 However, mechanical stress that exceeds the tolerance of the articular surface can accelerate the progression of joint degeneration, whereas decreasing mechanical forces on degenerated joint surfaces can stimulate the formation of a new biologic articular surface. 6 This is further highlighted in animal studies, where moderate exercise has been shown to produce an anabolic response in chondrocytes such that cartilage shows increased thickness and proteoglycan content, and decreased proteoglycan degradation. 28 Conversely, excessive, nonphysiologic loading, such as malalignment of the knee joint, can lead to chondrocyte degradation and has been associated with not only progression of knee osteoarthritis (OA) but also the initial development of knee OA. 1,5
Several biomechanical studies have reported that varus malalignment of the lower extremity is associated with increased forces across the medial compartment of the knee, with a deviation as little as 3° resulting in significantly increased peak stresses. 1,2,12 Thus, patients evaluated with chondral lesions of the tibiofemoral joint should undergo further evaluation of lower extremity alignment, with correction indicated when malalignment may place increased stress on the cartilage repair site. Similarly, other studies have demonstrated that meniscal repair or transplantation fails at a higher rate in the presence of ACL instability or lower extremity malalignment 11,27 and that HTO can improve outcomes in these patients. 3 These studies further demonstrate the need to assess the knee joint as a whole by considering cartilage status, ligament stability, meniscal status, and lower extremity alignment.
Limitations
The limitations of this study should be noted. Only 5 studies were included, and 4 were considered low levels of evidence (level 3 or 4), with potential bias in outcome measurement due to a lack of randomization in these studies. There was heterogeneity in the type of cartilage- restoration procedures performed, the definition of graft failure between studies, and the reported PROs between studies. Groups A and B differed with regard to preoperative lower extremity alignment, and therefore, it is difficult to state a threshold malalignment that benefits from concomitant osteotomy when cartilage repair is performed. Another variable that needs to be considered is degree correction. In practice, a patient may undergo concomitant HTO regardless of whether he or she truly has malalignment. For example, the mechanical axis could be corrected to that of the contralateral limb, to the center of the knee, or to the 62% point across the tibial width to “unload” the compartment, as is done in arthritis. Some surgeons will stage the cartilage repair/osteotomy procedures to do the osteotomy first (eg, while waiting for an OCA graft) or, if not truly malaligned, to do the osteotomy later only if the patient gets insufficient improvement from the chondral resurfacing. There is both surgeon and patient selection bias with respect to who gets an osteotomy with the preponderance of HTOs in men. Also, some patients may not be good candidates for osteotomy because of disease, such as chondromalacia and relative meniscal insufficiency, in the other compartments. Furthermore, most of the cartilage restoration procedures used in the included studies were either ACI or OCA, and thus these results cannot be applied to other cartilage procedures. Finally, only 3 distal femoral osteotomies were included in group B, and therefore, our results do not necessarily reflect the results of cartilage repair with DFO.
Conclusion
Patients undergoing cartilage repair of the tibiofemoral joint with concomitant osteotomy might be expected to experience greater improvement in clinical outcomes with a lower reoperation rate compared with cartilage repair alone. Surgeons preparing for cartilage procedures of the knee joint should pay particular attention to preoperative malalignment of the lower extremity in order to optimize outcomes. Further randomized controlled studies are needed before a definitive clinical decision can be made regarding performing an osteotomy with a cartilage procedure.
Footnotes
Final revision submitted September 30, 2022; accepted November 10, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.K.M. has received consulting fees and speaking fees from Arthrex. A.J.S. has received research support from Isto Biologics, consulting fees from DePuy/Medical Device Business Services, and has stock/stock options in Biomet, ConMed, Johnson & Johnson, Pfizer, Smith & Nephew, and Stryker. P.C.M. has received research support from Arthrex and Smith & Nephew and consulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.