
Abstract
Background:
Osteoarthritis (OA) progression in the lateral compartment is the most common reason for revision after medial unicompartmental knee arthroplasty (UKA). Altered contact kinematics in the lateral compartment may be related to the pathogenesis of OA.
Purpose:
To quantify the in vivo 6 degrees of freedom (6-DOF) knee kinematics and contact points in the lateral compartment during a single-leg lunge in knees after medial UKA and compare them with the contralateral native knee.
Study Design:
Descriptive laboratory study.
Methods:
Included were 13 patients (3 male, 10 female; mean age, 64.7 ± 6.2 years) who had undergone unilateral medial UKA. All patients underwent computed tomography preoperatively and 6 months postoperatively, and bilateral knee posture was tracked using dual fluoroscopic imaging system during a single-leg deep lunge to evaluate the in vivo 6-DOF kinematics. The closest points between the surface models of the femoral condyle and the tibial plateau were determined to locate the lateral compartment contact positions. The Wilcoxon signed-rank test was used to compare knee kinematics and lateral contact position between the UKA and native knees. Spearman correlation was used to test the associations of bilateral 6-DOF range difference and lateral compartment contact excursion difference with bilateral limb alignment difference and functional scores.
Results:
Compared with native knees, UKA knees had an increased anterior femoral translation of 2.0 ± 0.3 mm during the entire lunge (P < .05). The lateral contact position in UKA knees was located 2.0 ± 0.9 mm posteriorly and with 3.3 ± 4.0 mm less range of contact excursion than native knees (P < .05). Decreased range of lateral compartment contact excursion in the anterior-posterior direction was significantly associated with increased hip-knee-ankle angle in the UKA side (P < .05).
Conclusion:
The current study revealed altered knee 6-DOF kinematics and the reduced contact excursion range during single-leg lunge after unilateral medial UKA.
Clinical Relevance:
The altered contact kinematics and reduced range of contact excursion in UKA knees could lead to excessive cumulative articular surface contact stress, which is implicated in the pathogenesis of OA.
Keywords
Unicompartmental knee arthroplasty (UKA) is a bone- and ligament-sparing alternative to total knee arthroplasty (TKA) in the treatment of patients with single-compartment osteoarthritis (OA). 30 UKA offers several potential advantages over TKA, including less surgical exposure, more preservation of bone stock, retention of cruciate ligaments, faster postoperative recovery, and improved patient satisfaction. 18,25 –27 However, the clinical results of UKA still show a 7% to 13% higher revision rate compared with TKA at 8 to 10 years after surgery, with progression of OA and aseptic loosening having the highest incidence rates. 24,32,39 In addition, progression of OA was a more commonly reported complication in midterm and late failures, 39 and lateral compartment OA progression significantly affects clinical outcomes after medial UKA. 28 However, the pathogenesis of lateral compartment OA progression after medial UKA currently remains unclear.
Previous studies have focused on the limb alignment, in vivo, and in vitro kinematics of the knee after UKA. Severe limb malalignment, especially in the coronal plane (varus/valgus), could increase the risk of early polyethylene liner wear and cartilage degeneration of the nonreplaced compartment, highlighting the importance of proper limb alignment in UKA. 15 However, OA progression in the nonreplaced compartment was still observed in well-aligned UKAs over 10 years, 4,10 implying that other biomechanical factors also contributed to the pathogenesis of OA. Price et al 34 found that patients with mobile-bearing (MB) UKA exhibited more normal in vivo sagittal plane kinematics at long-term follow-up than TKA. In addition, in vitro studies have reported that fixed-bearing (FB) UKA could closely reproduce the native range of knee flexion, tibial axial rotation, and femoral anteroposterior translation. 16,33 However, improved recovery of knee kinematics after UKA compared with TKA has been inconsistent, and UKA is associated with a higher revision rate and continuous OA progression, 24,39 which may be attributed to the lack of articular contact trajectory of the nonreplaced compartment. Finite element analysis has suggested that patient-specific design of medial FB UKA can better protect the cartilage and meniscus in the nonreplaced compartments than traditional design. 19 Zarei et al 43 reported that medial FB UKA had no significant effect on lateral compartment joint space and contact location during chair-rise movement for 6 patients; however, their small sample size limited the level of evidence, and more challenging weightbearing activities (eg, single-leg lunge) should be considered to fully evaluate the knee function. Therefore, the in vivo kinematics and biomechanical changes of nonreplaced compartments after FB UKA during weightbearing activities would provide significant insights into the mechanism of OA progression.
The accurate in vivo tibiofemoral kinematics and articular contact pattern have been quantified to evaluate the biomechanical condition of the knee. 14,23 The in vivo study quantified tibiofemoral cartilage contact position by the closest point between the femoral and tibial models and suggested that an abnormal contact pattern of the knee with anterior cruciate ligament (ACL) deficiency was commonly associated with degeneration of cartilage. 23 Furthermore, the contact kinematics of TKA and FB UKA during vigorous activities have been quantified to predict the in vivo wear performance of the polyethylene liner. 7,8,40 However, no previous study has reported the effect of FB UKA on the tibiofemoral kinematics and contact pattern in the opposite nonreplaced compartment. Therefore, it is essential to investigate whether in vivo 6 degrees of freedom (6-DOF) and contact patterns in the nonreplaced compartment are restored after FB UKA.
The aims of the current study were to (1) quantify the in vivo 6-DOF kinematics and contact positions in the lateral nonreplaced compartment of UKA and native knees during weightbearing single-leg lunge and (2) analyze the effects of medial FB UKA on the knee 6-DOF and contact kinematics of the lateral nonreplaced compartment. The study hypothesis was that medial FB UKA could alter normal knee kinematics and the contact pattern of the lateral compartment.
Methods
Patient Data
The study was performed according to a protocol approved by our institutional review board, and informed consent was obtained from each patient. Included were 13 patients (3 male, 10 female), who underwent a medial FB UKA (Restoris MCK; Stryker) for medial compartment OA. Component implantation was guided by a single surgeon (Q.W.) using Mako robotic instrumentation (Stryker) during surgery. The exclusion criteria were postoperative knee pain, ACL deficiency, any postoperative complications, and musculoskeletal diseases. ACL integrity was examined through the exposed surgical field before and after UKA implantation and was evaluated by manual anterior drawer, Lachman, and pivot-shift tests during the follow-up period. 20 All patients were asked to finish several scales to evaluate postoperative knee function: Oxford Knee Score (OKS), 9 Knee Society Score (KSS), 17 and Forgotten Joint Score (FJS). 3 The patient characteristics and postoperative knee function data are shown in Table 1.
Patient Characteristics and Postoperative Knee Function Data (N = 13 patients) a
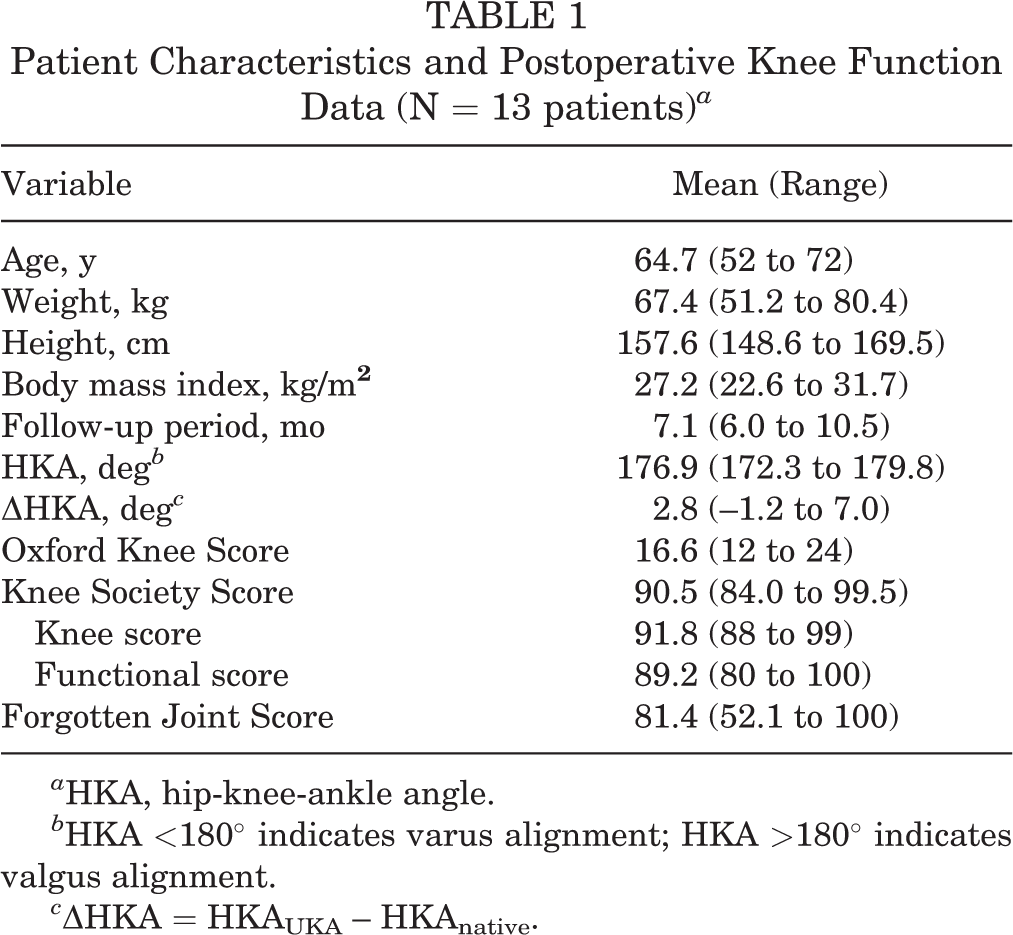
a HKA, hip-knee-ankle angle.
b HKA <180° indicates varus alignment; HKA >180° indicates valgus alignment.
c ΔHKA = HKAUKA – HKAnative.
Computed Tomography–Based 3-Dimensional Modeling of the Knee
The computed tomography (CT) images were acquired to reconstruct 3-dimensional (3D) models and coordinate systems of the knee for preoperative planning and postoperative fluoroscopic study. The hip, knee, and ankle joints in the UKA side were imaged under a 64-slice CT scan (Sensation 64; Siemens) for each patient before surgery. The 3D surface models of the femoral head, femoral condyles, tibial plateau, and ankle were reconstructed based on segmentation of CT images using the region-growing method in Amira 6.7.0 (Thermo Fisher Scientific). Patients underwent CT again 6 months after medial UKA surgery for 3D modeling of knees (both sides) and implanted prostheses using the same protocol.
Before surgery, the anatomic bony landmarks on surface models of the hip center and medial and lateral femoral epicondyles of the UKA knee were used to create a femoral coordinate system, and the ankle center and medial and lateral tibial plateau centers were used to create a tibial coordinate system, according to the method of Grood and Suntay. 13 To ensure the consistency of coordinate definition, we mirrored and aligned the 3D models of the preoperative UKA knee with the coordinate systems of the native knee after using iterative closest points to construct the coordinate systems. 5,37 The meshes of the knee models in the medial compartment were excluded in the alignment procedure to reduce the effect of modeling error caused by CT metal artifact in postoperative UKA knees. A 3D deviation analysis indicated that the root mean square error of the alignment method was 0.28 ± 0.05 mm for the femur and 0.32 ± 0.08 mm for the tibia on the UKA side and 0.44 ± 0.18 mm for the femur and 0.47 ± 0.08 mm for the tibia on the native side. The manufacturer provided 3D computer-aided design (CAD) models of femoral and tibial implants that were used in motion measurement. Thus, the CAD models of implants were aligned to reconstructed implants to determine the position of implants relative to femoral and tibial coordinate systems. The root mean square error of distances between the 3D CAD and reconstructed implant models was 0.27 ± 0.06 mm for the femoral condyle and 0.33 ± 0.07 mm for the tibial baseplate.
In Vivo Fluoroscopic Motion Measurement
The in vivo posture of the knee during static standing and weightbearing single-leg lunge was simultaneously tracked using a dual fluoroscopic imaging system (DFIS) for both UKA and native knees. The single-leg lunge is a representative high flexion and weightbearing activity that is widely used in rehabilitation training and joint function evaluation after knee arthroplasty. 11,12,38 Two mobile fluoroscopes (BV Pulsera; Phillips Medical) were set in approximately orthogonal position in practice, and the relative position between the fluoroscopes was recorded to build a virtual DFIS in MATLAB (MathWorks). The radiation pulse was 30 snapshots per second with 8-millisecond width, and the size of the acquisition image was 280 × 280 mm (1024 × 1024 pixels).
The acquired 2-dimensional (2D) dynamic fluoroscopic images were placed corresponding to the imaging planes, and 3D surface models of bones and implants were also imported to a virtual DFIS environment. The bone and implant model position were independently manipulated until the projection of the 3D surface model to imaging planes matched the contour of the 2D fluoroscopic images. The accurate spatial positions of the bone and implant were acquired based on a 2D-3D matching procedure, with measurement errors of <0.2 mm in translation and 0.4° in rotation. 22,36
The hip-knee-ankle angle (HKA) in the UKA and native knees was measured as the angle between the femoral mechanical axis (line through center of the hip and center of the knee) and tibial mechanical axis (line through center of the ankle and center of the knee), and femoral and tibial mechanical axes were defined by DFIS at static standing posture. Lower limb symmetry was evaluated by calculating the difference in HKA between the UKA and native sides (ΔHKA). The tibiofemoral 6-DOF kinematics (femoral transepicondyle axis center relative to the tibia and tibial rotation relative to the femur) during the single-leg lunge were calculated for both UKA and native knees. The tibial flexion angle was defined as the angle between the y-axes of the femoral coordinate system and the tibial coordinate system, and 6-DOF kinematics were analyzed with a tibial flexion angle of 0° to 100°.
Lateral Compartment Articular Contact Tracking
The measured 6-DOF kinematics and shapes of the femoral condyle and tibial plateau models were used to determine the articular contact position in the lateral nonreplaced compartment after medial FB UKA. The contact positions were tracked by identifying the point with minimum distance between surfaces of the femoral condyle and tibial plateau in the lateral compartment corresponding to the tibiofemoral kinematics. The tibial coordinate systems of UKA and native knees were referred to quantify the contact positions, which were transformed with respect to the anterior-posterior (AP) and medial-lateral (ML) axes of the tibia. The lateral compartment contact positions in the UKA and native knees were normalized according to the length of the transepicondylar axis.
The knee flexion cycle was divided into early flexion (0°-30°), midflexion (30°-60°), and deep flexion (60°-100°), and the movement of the lateral compartment contact position was quantified to analyze the contact excursion pattern. The difference in lateral compartment contact excursion between the UKA and native knees (ΔExcursion) was calculated for the AP and ML directions and was recorded as a percentage of the native knee (Δ%AP excursion and Δ%ML excursion, respectively).
Statistical Analysis
Means and standard deviations of in vivo 6-DOF and articular contact position in the lateral compartment were reported relative to the knee flexion angle from 0° to 100°. All measurements were tested using the Kolmogorov-Smirnov test for normality. The Wilcoxon signed-rank test was used to compare the 6-DOF kinematics and lateral contact position between the UKA and native knees. Spearman correlation was calculated to test for the associations of bilateral 6-DOF range differences ([Value UKA – Value Native]/Value Native), lateral compartment Δ%AP excursion, and lateral compartment Δ%ML excursion with ΔHKA, OKS, KSS, and FJS. The level of significance was set as .05, and all statistical analyses were conducted using MATLAB (MathWorks).
Results
Knee Kinematics During the Single-Leg Lunge
The UKA knees showed a similar pattern of 6-DOF kinematics to native knees (Figure 1). Both UKA and native knees exhibited internal tibial rotation during the lunge. During knee flexion from 0° to 100°, the tibias of the UKA and native knees rotated from external rotation positions of –2.1° ± 4.9° and –5.8° ± 6.5° to internal rotation positions of 5.5° ± 5.8° and 2.6° ± 6.6°, respectively. The UKA knees demonstrated an average increased internal rotation of 2.2° ± 0.5° compared with the native knees (P > .08) (Figure 1A). Both UKA and native knees had similar tibial varus angles during the lunge (Figure 1B). There were no significant differences in the range of tibial rotation between the UKA and native knees (Table 2).

Mean values with standard deviations (shaded areas) of the 6 degrees of freedom (6-DOF) kinematics in unicompartmental knee arthroplasty (UKA) and native knees during the single-leg lunge. The 6-DOF kinematics were normalized relative to the knee flexion angle during the lunge. (A and B) Tibial internal rotation (IR)/external rotation (ER) and tibial varus/valgus alignment. (C and E) Femoral anterior-posterior, proximal-distal, and medial-lateral translations. The rotations represent the tibial rotations relative to the femur, and the translations represent the femoral motions relative to the tibia. The red line on the horizontal axis indicates significant differences between UKA and native knees (P < .05).
The 6-DOF Kinematics of the UKA and Native Knees During the Single-Leg Lunge a

a 6-DOF, 6 degrees of freedom; AP, anterior-posterior; ER, external rotation; IR, internal rotation; ML, medial-lateral; PD; proximal-distal; UKA, unicompartmental knee arthroplasty.
A significant difference in femoral AP translation was observed between the UKA and native sides during the lunge. During knee flexion from 0° to 100°, the femurs of the UKA knee moved posteriorly from 0.4 ± 3.5 to –11.9 ± 3.5 mm, and the femurs of the native knee moved posteriorly from –0.5 ± 4.0 to –14.1 ± 3.5 mm. The knee joint center of the UKA knees was located more anteriorly in the AP direction compared with the native knees during knee flexion of 6° to 100° (P < .05) (Figure 1C), and 2.0 ± 0.3-mm increased anterior femoral translation, on average, was observed in the UKA knees compared with the native knees during the entire lunge (P < .05). The differences between UKA and native sides in the proximal-distal and ML directions were not statistically significant (Figure 1, D and E). There were no significant differences in the range of femoral translation during the lunge between UKA and native knees (P > .1) (Table 2)
Lateral Compartment Contact Position After Medial UKA
The lateral compartment contact position of medial UKA knees was more posterior than that of native knees (Figures 2 and 3). The articular contact position in the lateral compartment of UKA knees sharply moved posteriorly in early flexion (0°-30°) from 2.1 ± 3.0 to –3.7 ± 2.6 mm, then moved to –4.8 ± 2.4 mm at 60° of flexion, and finally moved to –7.0 ± 3.5 mm at flexion of 100°. The contact position of the lateral condyle in the native knees continuously moved posteriorly from 6.7 ± 3.0 mm at full knee extension of 0° to –2.0 ± 2.5 mm at 30° of flexion, –3.4 ± 1.8 mm at 60° of flexion, and –5.3 ± 3.5 mm at 100° of flexion (Figure 2A). The contact position of the lateral condyle in UKA knees was located 2.0 ± 0.9 mm posteriorly, on average, compared with native knees during a flexion angle of 0° to 92° (P < .05). Furthermore, the lateral contact excursion of the UKA knees in early flexion was 5.8 ± 2.7 mm, which was significantly less than that of native knees (8.7 ± 2.6 mm) (P < .01). There were no statistically significant differences in lateral contact excursion at midflexion (30°-60°) or deep flexion (60°-100°). Overall, the AP lateral contact excursion range in the UKA side was 3.3 ± 4.0 mm smaller than in native knees in the entire flexion cycle (P < .05) (Table 3).
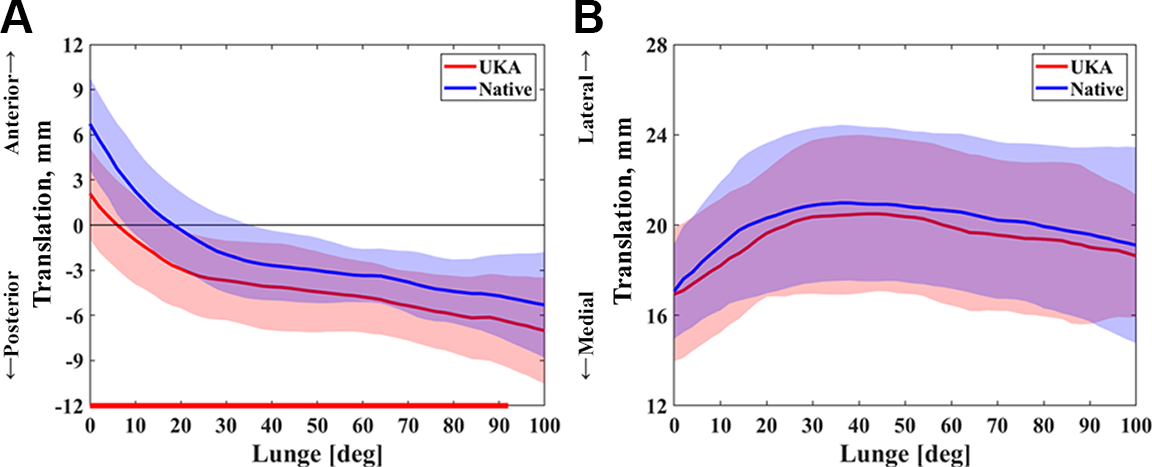
Mean values with standard deviations (shaded areas) of the lateral compartment contact positions in unicompartmental knee arthroplasty (UKA) and native knees during the single-leg lunge. The lateral contact positions were normalized relative to the knee flexion angle during the lunge. Contact position in the (A) anterior-posterior and (B) medial-lateral directions. The red line on the horizontal axis indicates significant differences between UKA and native knees (P < .05).
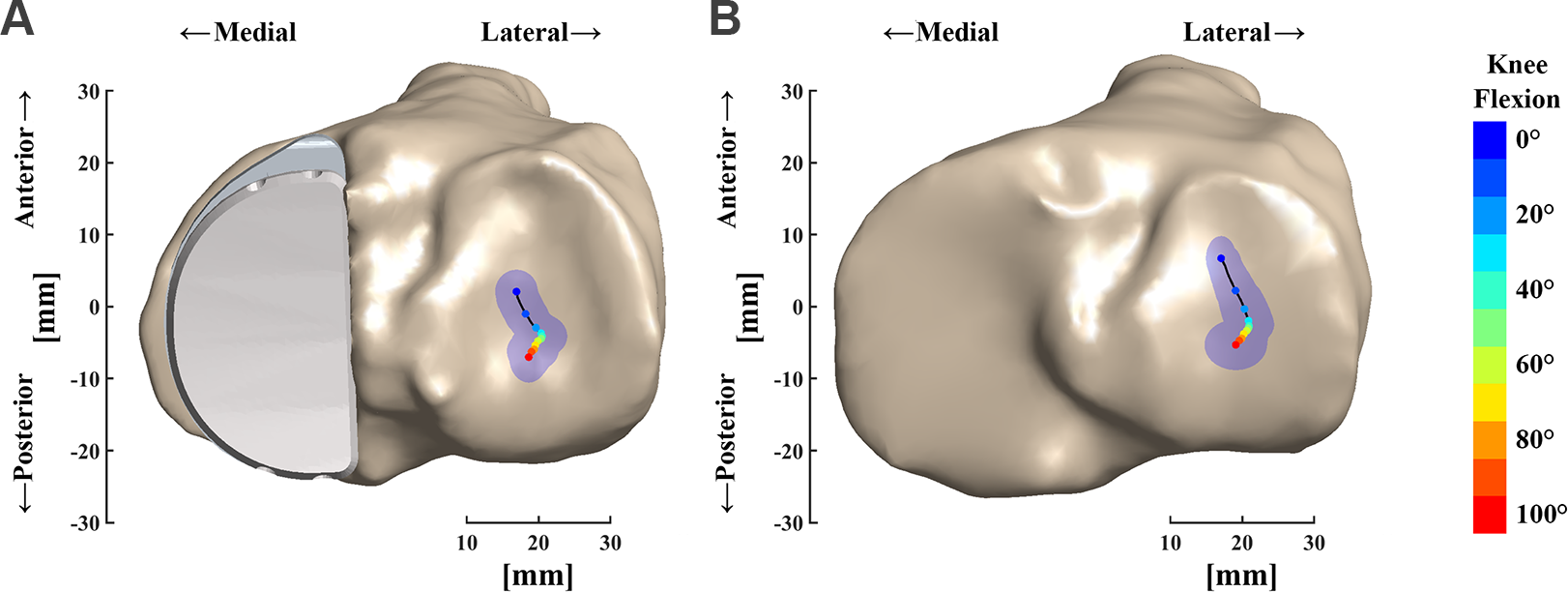
Lateral articular contact excursion of (A) unicompartmental knee arthroplasty knees and (B) native knees during the single-leg lunge. The points with different colors represent contact positions at different knee flexion angles. The blue-shaded area indicates overlapped ellipses within 1 SD of contact position in the anterior-posterior and medial-lateral directions.
Range of Lateral Compartment Contact Excursion in the AP and ML Directions for UKA and Native Knees a
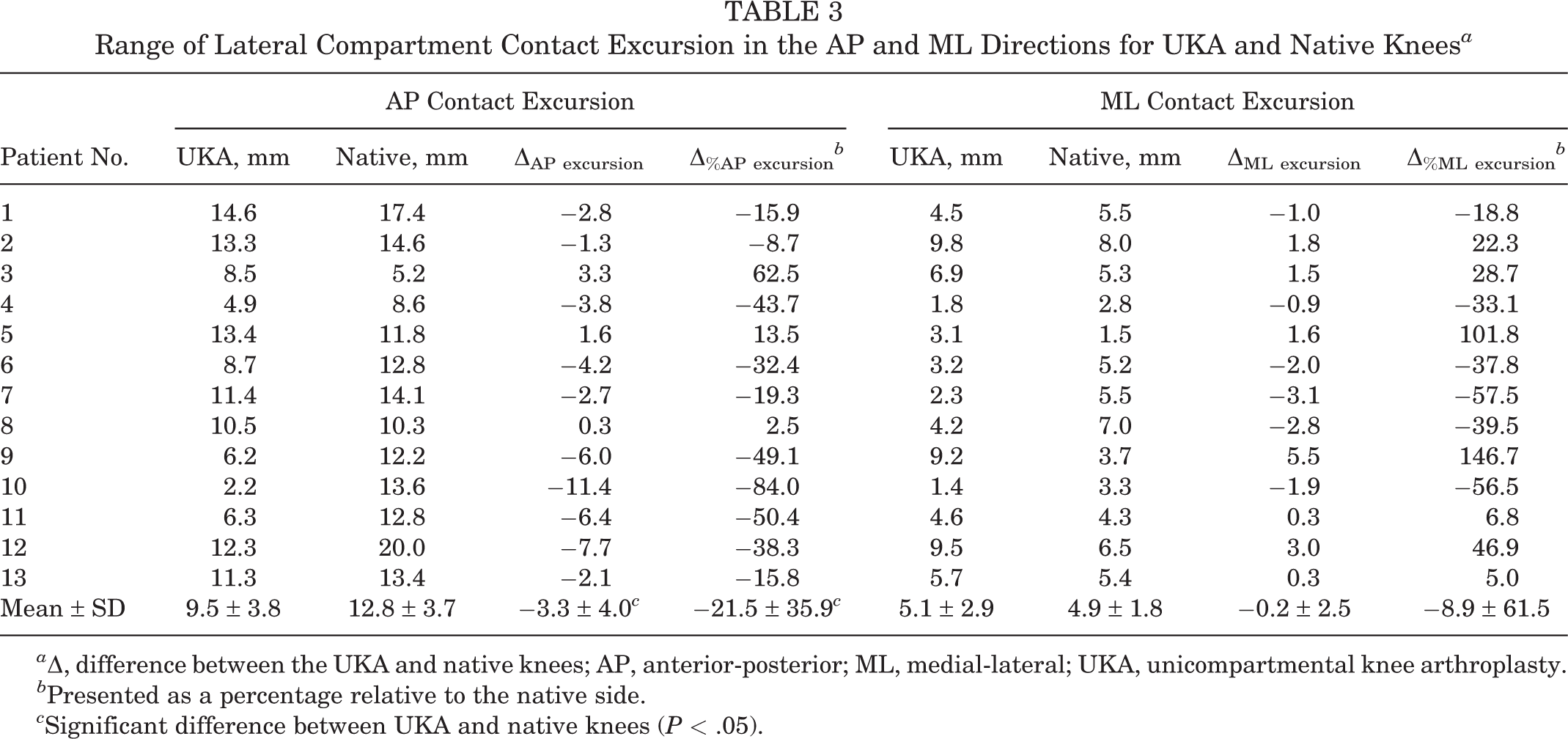
a Δ, difference between the UKA and native knees; AP, anterior-posterior; ML, medial-lateral; UKA, unicompartmental knee arthroplasty.
b Presented as a percentage relative to the native side.
c Significant difference between UKA and native knees (P < .05).
The articular contact position of the lateral compartment in the ML direction showed a similar pattern in both UKA and native knees. The contact position of the lateral condyle moved laterally in early flexion, while it moved medially in midflexion and deep flexion (Figures 2 and 3B). The differences in the lateral condyle contact position and range of contact excursion in the ML direction were not statistically significant between the UKA and native sides (Table 3).
Correlation Between Knee Kinematics and HKA: Functional Scores
There were no significant associations between altered range of knee 6-DOF and ΔHKA, OKS, KSS and FJS (Table 4). The Δ%AP excursion was significantly associated with increased ΔHKA (r = –0.5879; P = .04) (Table 4 and Figure 4). There were no significant associations between Δ%ML excursion and ΔHKA, OKS, KSS, and FJS (Table 4).
Spearman Correlation (r) Between Bilateral 6-DOF Range Difference, Difference in Lateral Compartment Contact Excursion, and ΔHKA, OKS, KSS, and FJS a

a Δ, difference between the unicompartmental knee arthroplasty and native knees; 6-DOF, 6 degrees of freedom; AP, anterior-posterior; ER, external rotation; FJS, Forgotten Joint Score; HKA, hip-knee-ankle angle; IR, internal rotation; KSS, Knee Society Score; ML, medial-lateral; OKS, Oxford Knee Score; PD, proximal-distal.
b Range difference = (Value UKA – Value Native)/Value Native.
c Statistically significant (P < .05).
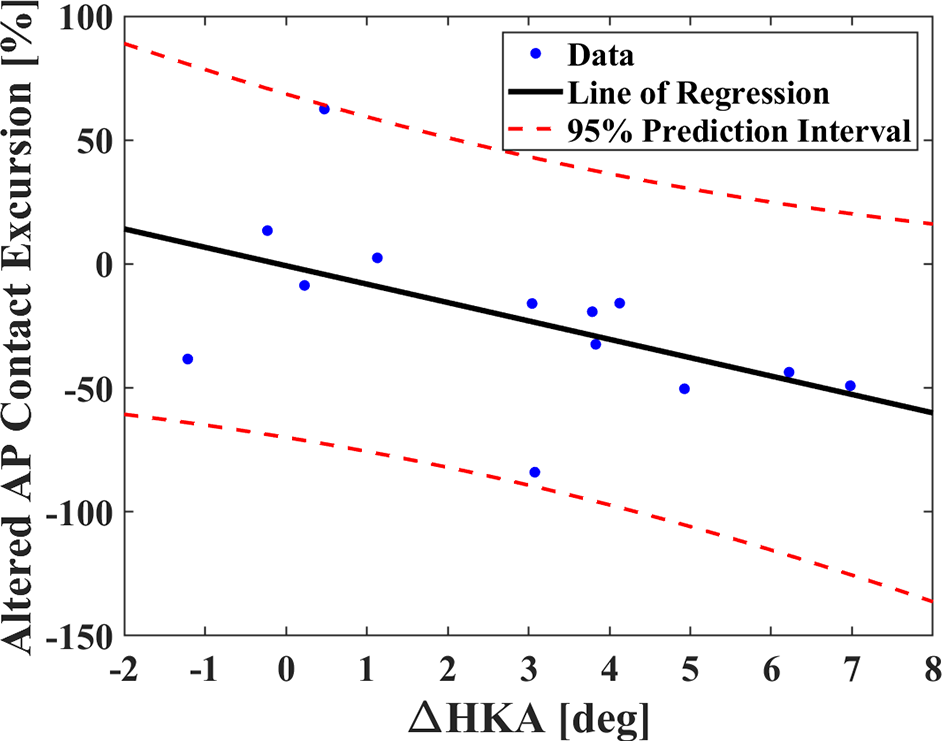
Association between Δ%AP excursion and ΔHKA. A positive ΔHKA indicates knee valgus, and a negative ΔHKA indicates knee varus. Δ, difference between the unicompartmental knee arthroplasty and native knees; AP, anterior-posterior; HKA, hip-knee-ankle angle.
Discussion
In the current study, we found increased anterior femoral translation in the UKA knee compared with the native knee during the weightbearing single-leg lunge (P < .05), while other 6-DOF kinematics were similar. The lateral compartment contact position of UKA knees was significantly more posterior (P < .05) with a smaller range of contact excursion (P < .01) in the AP direction than those in the native side. In addition, lateral compartment Δ%AP excursion was significantly associated with increased ΔHKA (P < .05). These results supported our hypothesis that the lateral compartment contact kinematics would be altered after medial FB UKA.
Previous studies have reported that UKA can better restore normal knee kinematics than traditional TKA. 16,21,33,34 One study reported that UKA knees exhibited similar in vivo femoral external rotation and condyle AP motion during squatting to normal knees. 21 The in vitro knee simulator studies have also indicated that kinematics during knee flexion were restored after FB UKA. 16,33 However, the contrary finding was reported: postoperative femoral axial rotation and transepicondyle axis movement during squatting were close to preoperative OA knees rather than normal knees. 29 In the current study, similar tendencies of in vivo 6-DOF with different magnitudes between UKA and native knees were observed. We found an average 2.2° ± 0.5° increased tibial internal rotation and 2.0 ± 0.3-mm increased femoral AP location in the UKA side during the entire flexion cycle of the lunge compared with native knees, while there were no significant differences in the range of 6-DOF kinematics. Tibial internal rotation increases during gait for knees with different OA severities, 31 which was not completely corrected after medial FB UKA. In addition, the more anterior femoral location may decrease the weightbearing range of knee flexion and increase the risk of posterior bone impingement. 2 The increased femoral AP location and tibial internal rotation were not associated with patient-reported knee function scores and clinical outcomes in the short-term follow-up period (Table 4). The long-term effect of FB UKA on knee kinematics should be followed up continuously. In general, the 6-DOF results during lunge indicated that normal knee kinematics were altered after medial FB UKA in the short-term follow-up period.
Excessive cumulative articular surface contact stress resulting from altered contact kinematics might lead to OA progression of cartilage. 1,6 The complex interaction among in vivo kinematics, joint mechanics (including contact mechanics and joint laxity), and cartilage mechanobiology (including cell metabolism and response to mechanical stimuli) can result in the initiation and progression of knee OA, 1 which stresses the relevance of in vivo contact kinematics during functional activities. Zarei et al 43 found that lateral compartment joint space and the contact location of 6 patients during the chair-rise movement were not altered after medial FB UKA; however, no detailed data of contact position were reported, and small sample size reduced the evidence level.
To the best of our knowledge, this study is the first to precisely evaluate the effects of medial UKA on the in vivo lateral compartment contact kinematics during weightbearing activities. In the AP direction, the lateral articular contact of UKA knees was located in a 2.0 ± 0.9-mm more posterior position, with a 3.3 ± 4.0-mm smaller range of contact excursion during the entire flexion cycle of the lunge than native knees. There were no significant differences of lateral compartment contact kinematics in the ML direction between bilateral knees (Figure 2). In addition, the individual variability in the range of AP contact excursion of the lateral condyle between UKA and native knees was high during the lunge for patients who underwent unilateral UKA (Table 3). Seven of 13 patients had more than 30% differences in the range of AP contact between bilateral sides, and decreased range of AP contact in UKA knees was observed in most patients (n = 10/13). The contact results indicated that biomechanical contact of the knee was not preserved after medial FB UKA, which may be a risk factor of OA progression in long-term follow-up. 24,39
Lower limb alignment overcorrection after FB UKA may contribute to the abnormal lateral compartment contact positions after medial FB UKA. Previous studies have suggested that mild varus limb alignment provides better clinical outcomes and survival rate in FB UKA compared with neutral or close-to-neutral alignment, 35,41 while valgus limb alignment has been associated with OA progression for patients undergoing revision. 35 Wen et al 42 investigated the effect of implantation parameters on the lateral compartment after MB UKA and reported that slightly varus (undercorrection) lower limb alignment reduced lateral contact stress of the femoral and tibial cartilage and might prevent lateral compartment OA progression. However, few studies have justified the in vivo effect of limb alignment on lateral compartment biomechanics. We found a 2.8° ± 2.5° increased HKA and a 3.3 ± 4.0 mm decreased range of lateral compartment AP contact excursion in the UKA side versus the native side (Tables 1 and 3), as well as a negative association between lateral compartment Δ%AP excursion and ΔHKA (r = –0.5879; P = .04) (Table 4). The linear regression line indicated that overcorrected limb alignment (ie, increased knee valgus) was associated with a significantly reduced lateral compartment Δ%AP excursion, and the FB UKA knee demonstrated similar lateral compartment Δ%AP excursion when FB UKA-restored limb alignment was the same as the native side (Figure 4). Overall, we hypothesized that the native unaffected limb might be a reliable reference for FB UKA surgical planning, and the effect of lower limb symmetry on lateral compartment contact biomechanics should be evaluated after surgery.
Limitations
There are several limitations of the current study to be noted. First, all patients in the study were given one type of FB UKA implant using robotic instrumentation, ensuring accurate component positioning. Therefore, the present results might not apply to other UKA designs or in UKAs with component malpositions. However, the current study is the first to quantify the effect of UKA on in vivo lateral compartment contact position during a weightbearing lunge, and other types of UKA should be investigated in the future, such as MB UKA. Second, the follow-up period was 6 to 10 months. Also, no magnetic resonance imaging data were available to illuminate the effect of abnormal lateral contact kinematics on biomechanical changes of cartilage and the meniscus for OA progression. We will continue to evaluate these patients to track the OA progression in the lateral compartment. Finally, we investigated lunge only. Although the lunge is considered challenging enough for patients to get good measurement of weightbearing knee flexion function, more functional activities should be studied in the future, for example, level and ramp walking, sit-to-stand, set-up, and step-down.
Conclusion
The study findings of altered contact kinematics and especially of reduced contact excursion range in UKA knees, which is associated with increased HKA compared with the native side, may lead to an excessive accumulation of contact stress. The present study provided new insights into the kinematic behavior of the lateral compartment after a medial UKA.
Footnotes
Final revision submitted October 13, 2022; accepted October 26, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: The current study was sponsored by the National Natural Science Foundation of China (grant No. 31972924), the Science and Technology Commission of Shanghai Municipality (grant No. 22S31906000), and the Pudong Science Technology and Economy Commission (grant No. 210H1147900). T.-Y.T. has received research support from MicroPort Co Ltd. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Shanghai Sixth People’s Hospital (reference No. 2017-084).