
Abstract
Background:
Outpatient unicompartmental knee arthroplasty (UKA) has been shown to be safe and feasible when compared with inpatient surgery; however, no studies have evaluated the cost-effectiveness and cost-benefit of performing outpatient versus inpatient UKA.
Hypothesis:
Significant cost savings can be achieved by transitioning UKAs from an inpatient to an outpatient procedure in an outpatient surgical facility, with no appreciable difference in complication or readmission rates.
Study Design:
Economic and decision analysis; Level of evidence, 3.
Methods:
A retrospective chart review of 25 consecutive medial UKAs was performed. A total of 10 inpatient UKAs with a mean length of stay of 1.6 days (range, 1-4 days) and 12 outpatient UKAs were included in the final analysis. A simple difference in costs incurred, reimbursements, and percentage difference between inpatient and outpatient surgery in an outpatient surgical facility was calculated. Charges were subdivided into surgical facility fees, inpatient room charges, operating room supply fees, and other fees. Secondary outcome measures included reason for greater than 1 day stay for the inpatient UKAs, complications, readmissions, and the type of regional anesthesia utilized.
Results:
The outpatient UKA charges were a mean $20,500 less per patient than the inpatient average charge of $46,845. The primary cost savings were attributed to the outpatient surgical facility fee, which averaged $3800 per patient, while the inpatient facility charge was 350% more expensive at $13,200 per patient (approximately $9500 savings). On the inpatient side, the average reimbursement was 55% of charges, or $25,550. For outpatient procedures, the average reimbursement was 47%, or $12,370. There was no difference between the inpatient and outpatient groups in terms of complications or readmissions.
Conclusion:
This work demonstrated that significant cost savings of roughly 50% can be achieved with an outpatient UKA protocol done at an outpatient surgical facility. Not only is it feasible and economically attractive to perform outpatient UKA, but it can reduce inpatient bed occupancy and resource allocation for a busy hospital.
Keywords
Unicompartmental knee arthroplasty (UKA) has traditionally been considered an inpatient procedure. Physician and patient concerns regarding uncontrolled pain, perioperative complications, and decreased mobility have resulted in at least a 1-night stay in the hospital. Unlike total knee arthroplasty (TKA), which involves extensive dissection and a typical 2- to 3-day inpatient stay, UKA can be done in a minimally invasive fashion with a smaller incision and substantially reduced pain since it involves only 1 part of the knee. Studies have shown increased patient satisfaction and improved outcomes with an accelerated recovery protocol and decreased length of hospital stay. 4,11
There are a few studies in the literature that have shown UKA performed as an outpatient surgery to be safe and feasible when compared with inpatient surgery, with no increased risk of complications or change in patient outcomes. Beard et al 1 published a pilot study involving 7 patients wherein all patients were discharged home within 24 hours from the time of surgery. No significant complications were noted in their series, but 1 patient failed to progress with knee flexion and required a manipulation under anesthesia. They commented that convalescence at home removes the patient from the threat of hospital-acquired infection, permits a more functional rehabilitation, and the cost for the institution is reduced. 1 Berger et al 2 prospectively followed 111 patients who had primary knee arthroplasty (25 UKA, 86 TKA) completed by noon. Ninety-four percent of patients (96% UKAs) met discharge criteria and were discharged directly to home the day of surgery. Within the first week after surgery, there were 4 readmissions and 1 emergency department visit without readmission—all in patients who underwent TKA. There were no deaths, cardiac events, or pulmonary complications. 2 Another case-controlled study compared outpatient UKA with the standard inpatient UKA. 13 Eighty-five percent of patients in the outpatient UKA study arm were able to be discharged home on the day of surgery. Delayed discharge was present in 2 patients who suffered from a high pain intensity and 1 patient who was fearful of going home. One outpatient UKA patient developed stiffness requiring manipulation under anesthesia at 6 weeks postoperative. 13 Cross and Berger 7 published their results on 105 consecutive patients undergoing UKA. All 105 patients (100%) were able to be discharged home the same day utilizing a rapid recovery protocol. No patients required readmission within the first week after surgery, and only 1 patient required readmission between weeks 1 and 12 for management of postoperative infection. 7
To our knowledge, no studies have been published evaluating the cost-effectiveness and cost-benefit of performing outpatient versus inpatient UKA. One study in the literature evaluated the efficacy of an accelerated recovery protocol after UKA with the goal of discharging patients home the day after surgery. 20 Their protocol achieved a cost savings of 27% and significantly reduced hospital bed occupancy. In addition, patient satisfaction was greater with the accelerated discharge than with the routine discharge time. Ambulatory surgery centers (ASCs) and outpatient surgery departments are focused on ensuring that patients have the best surgical experience possible while providing cost-effective care that can save the government, third-party payors, and patients money. For instance, Medicare pays significantly less for procedures performed in ASCs when compared with rates paid to hospitals for the same procedures. Accordingly, patient co-pays are also significantly lower when care is received in an ASC. However, the long-term growth of ASCs is threatened by the widening disparity in reimbursement that ASCs and hospitals receive for the same procedures.
Given the current focus on the cost of health care delivery, orthopaedic surgeons are encouraged to find methods of safely reducing the duration of inpatient stay after knee arthroplasty. With the opening of a new, more modern outpatient surgical center at our hospital, the principal investigator (D.R.D.) has been able to perform all UKA surgeries on an outpatient basis during the past year, unlike previous years when they were done as an inpatient surgery. The purpose of this study was to directly compare the costs and savings of performing outpatient UKA in an outpatient surgical facility versus inpatient UKA. We hypothesize that outpatient UKA done in an outpatient surgical facility will demonstrate significant cost savings when compared with inpatient UKA and that outpatient UKA will be shown to be safe and effective with equivalent complication and readmission rates as inpatient UKA.
Methods
Detailed patient account information and cost data are readily available at our institution for a 39-month period. Thus, between July 1, 2012, and September 30, 2015, a total of 25 patients underwent medial UKA surgery by the senior author (D.R.D.). The initial 12 consecutive patients were treated with inpatient surgery. Since the opening of the new outpatient surgical center, the next 13 consecutive patients were treated with outpatient surgery over a 10-month period.
A retrospective chart review of all 25 patients was performed. All patients had undergone medial UKA surgery and were at least 3 months out from surgery at the time of chart review. Cost data were also gathered from our accounting department. Two subjects who had inpatient surgery were excluded from the study. One patient did not have complete cost data available. The other subject was determined to not be representative of the inpatient cohort as the patient developed postoperative atrial fibrillation requiring an extended hospital stay and the resultant charges were nearly double that of the rest of the patients. The first subject who had outpatient surgery was also excluded as this individual had surgery at the main hospital and was charged the more expensive surgical facility fees associated with this setting as opposed to outpatient ambulatory surgical fees like the rest of our outpatient surgery cohort. After excluding the above patients, the final cohort consisted of 10 inpatient and 12 outpatient UKAs.
In all cases, patellar eversion, knee dislocation, and knee hyperflexion were avoided. A fixed-bearing unicompartmental system was utilized in all UKA cases (Unicompartmental High Flex Knee; Zimmer, now Smith & Nephew) (Figure 1). All patients received a regional nerve block in addition to general anesthesia as outlined below. Tourniquet was used for all patients. None of the outpatient UKA patients had a Foley catheter placed.
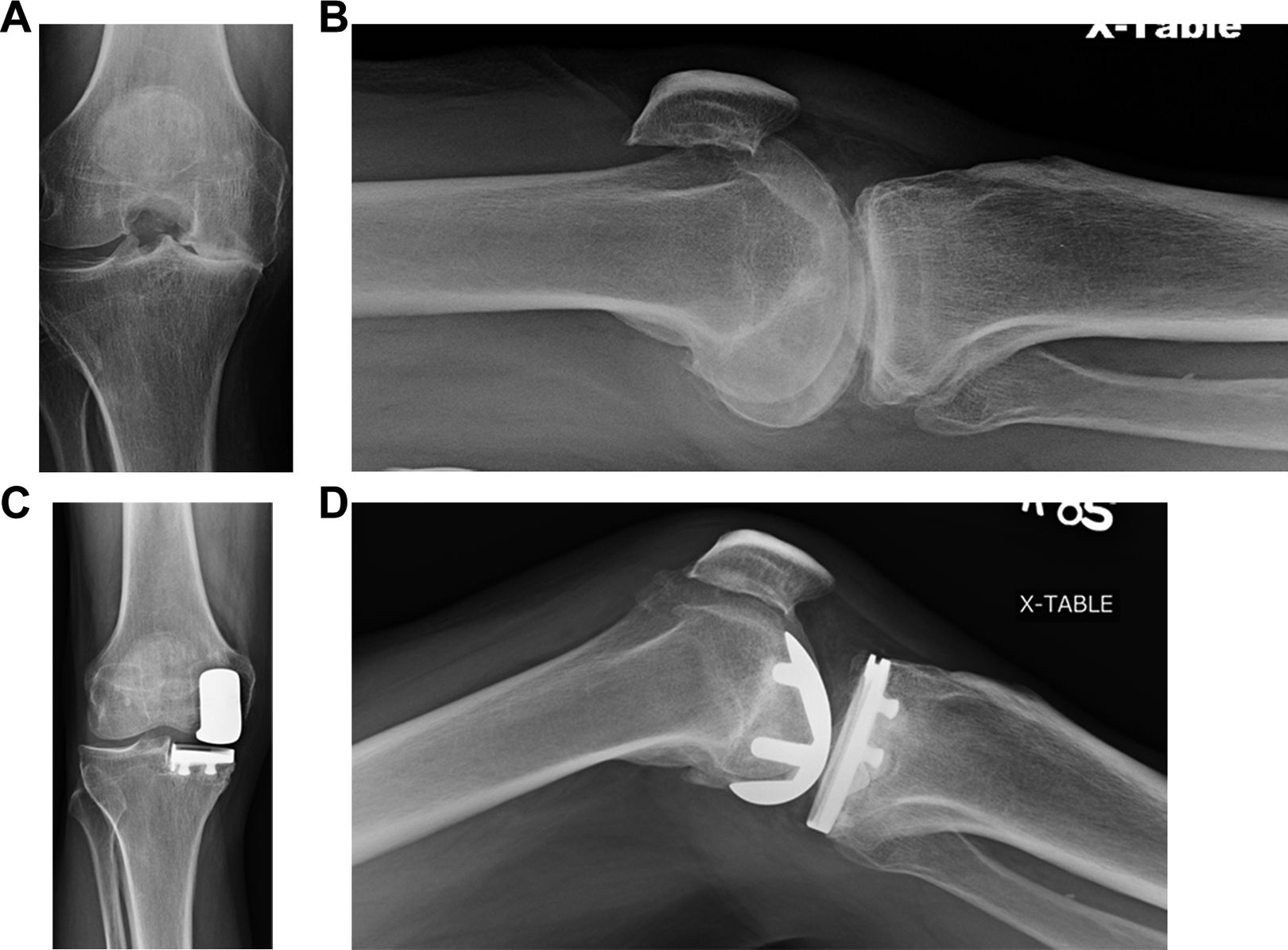
Anteroposterior and lateral radiographs demonstrating medial compartment knee osteoarthritis (A and B) before and (C and D) after medial unicompartmental knee arthroplasty.
A simple difference in costs incurred, reimbursements, and percentage difference between inpatient and outpatient surgery was calculated. Furthermore, the charges were subdivided into surgical facility fees, inpatient room charges, operating room (OR) supply fees, pharmacy fees, therapy fees, and laboratory fees. The surgeon’s professional fee was not included in the overall charges. Secondary outcome measures included the reason for a stay greater than 1 day for inpatient UKAs, complications, readmissions, and the type of regional anesthesia used for the outpatient UKA surgeries.
Results
Our study included 10 inpatient and 12 outpatient UKA patients. The inpatient cohort consisted of 8 males and 2 females, with a mean age of 64.5 ± 9.8 years. The outpatient cohort consisted of 7 males and 5 females, with a mean age of 67.2 ± 9.2 years. The outpatient cohort had a slightly higher mean body mass index (BMI) (28.7 vs 25.8 kg/m2), and both groups had similar American Society of Anesthesiologists (ASA) classifications based on their medical comorbidities, with the majority of patients being classified as ASA 2. Similar surgical times, as measured by tourniquet time, were noted between the 2 groups. Degree of medial compartment deformity as measured by the Kellgren-Lawrence knee osteoarthritis scale and knee alignment as measured by deviation from mechanical axis were recorded (Table 1). 5,10,14
Patient Characteristics and Surgical Factors a

a ASA, American Society of Anesthesiologists; BMI, body mass index; K-L, Kellgren-Lawrence.
b As measured on standing, flexion radiographs. All degrees are varus angulation as all patients had medial compartment osteoarthritis. One patient in both the inpatient and outpatient cohorts was excluded due to poor imaging, with no standing flexion view available for review.
For the 10 inpatient UKAs (Table 2), the average charge to a patient’s insurance carrier was $46,845. On average, 55% of charges were reimbursed through insurance, for an average total reimbursement of $25,551. The charge for OR supplies made up the largest percentage of overall charges at 52%. These include items such as gowns, drapes, saw blades, cement, and the actual charge for the UKA implant components. The charge for surgical facility fees made up the second largest percentage at 28%. This includes separate fees for OR time (per minute), recovery time, and anesthesia time. Another 6% of charges were accounted for by pharmacy, 4% were the actual cost of the hospital room, and 2% for inpatient physical and occupational therapy services.
Inpatient UKA Costs a
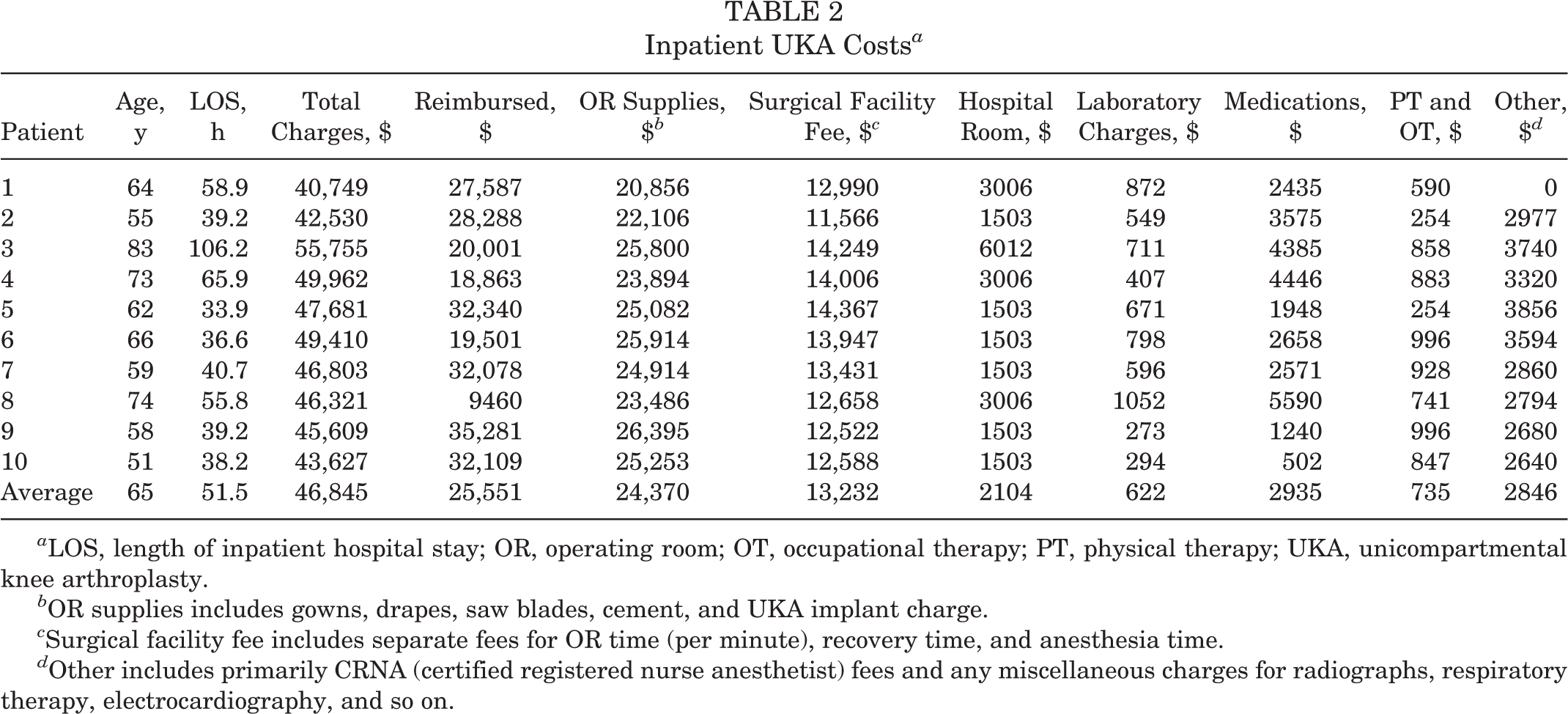
a LOS, length of inpatient hospital stay; OR, operating room; OT, occupational therapy; PT, physical therapy; UKA, unicompartmental knee arthroplasty.
b OR supplies includes gowns, drapes, saw blades, cement, and UKA implant charge.
c Surgical facility fee includes separate fees for OR time (per minute), recovery time, and anesthesia time.
d Other includes primarily CRNA (certified registered nurse anesthetist) fees and any miscellaneous charges for radiographs, respiratory therapy, electrocardiography, and so on.
For the 12 outpatient UKAs done in an outpatient surgical facility (Table 3), the average charge to a patient’s insurance carrier was $26,272. On average, 47% of charges were reimbursed through insurance, for an average total reimbursement of $12,368. The charge for OR supplies made up the largest percentage of overall charges at 74%, while the charge for surgical facility fees made up only 14% of the total cost. The surgical facility fee for outpatient procedures is a fixed charge that incorporates anesthesia, OR time, and recovery fees based on the type of surgery the patient is having (Surgical Facility Fee, Table 3). Furthermore, for outpatient UKA, there were no hospital room, laboratory, or therapy charges.
Outpatient UKA Costs a

a OR, operating room; OT, occupational therapy; PT, physical therapy; UKA, unicompartmental knee arthroplasty.
b OR supplies includes gowns, drapes, saw blades, cement, and UKA implant charge.
c Surgical facility fee is a fixed charge that includes OR time (per minute), recovery time, and anesthesia time.
d Other includes primarily CRNA (certified registered nurse anesthetist) fees and any miscellaneous charges for radiographs, respiratory therapy, electrocardiography, and so on.
Patients receiving inpatient UKAs stayed an average of 1.6 days (range, 1-4 days) in the hospital. The reason that any patient stayed longer than 1 day (4 patients total) was due to inadequate pain control or difficulty with mobilization. All patients had an ASA score of 2, except 1 patient who had an ASA score of 3. Three mild postoperative complications were noted. One patient developed a superficial infection that was successfully treated with oral antibiotics, another patient had a traumatic mild wound dehiscence treated with local wound care, and a third patient had a postoperative urinary tract infection.
All outpatient UKA patients were successfully discharged home on the day of surgery. Ten patients had an ASA score of 2 and 2 patients had an ASA score of 3. For regional anesthesia, 8 patients had single-shot femoral nerve blocks and 4 patients had continuous femoral nerve blocks via an indwelling pain catheter, with which they were discharged home, and single-shot sciatic nerve blocks. No complications were encountered in the outpatient UKA group. There were no patients readmitted in either the inpatient or outpatient groups.
Discussion
To our knowledge, this is the first study evaluating the cost-effectiveness and cost-benefit of performing outpatient UKA in an outpatient surgical facility versus inpatient UKA. Other studies mentioned previously have looked at the cost savings of an accelerated discharge protocol for UKA but not a truly outpatient UKA surgery in which the patient is discharged home the same day. Lovald et al 16 evaluated the costs associated with outpatient TKA versus inpatient TKA utilizing a Medicare patient database. They noted that the costs that can be attributed to knee osteoarthritis over a 2-year postoperative period were reduced by $1967 per patient in the 1- to 2-day stay group and by $8527 per patient in the outpatient group compared with the standard length of stay (3-4 days) group. 16 A recent systematic review evaluating some of the more common orthopaedic procedures showed an average cost savings of 17.6% to 57.6% for outpatient procedures relative to similar procedures performed in a hospital. 6
The outpatient charges in our study were found to be an average of $20,573 less per patient than the inpatient average charge of $46,845 (Table 4). The primary cost savings were attributed to the outpatient surgical facility fee, which averaged $3800 per patient, while the inpatient facility charge was 350% more expensive at $13,200 per patient (approximately $9500 savings). However, even the highest cost category (OR supplies) was an average 25% higher for an inpatient as opposed to an outpatient UKA. Furthermore, hospital price variability for inpatient surgery is much larger than that of outpatient surgery or ASCs. Our data demonstrated a maximum patient-to-patient difference in charges of approximately $15,000 for UKA performed in an inpatient hospital setting as compared with a maximum patient-to-patient difference of only $6200 for UKA performed at an outpatient surgical facility.
Average Inpatient Versus Outpatient Surgery Center UKA Cost Comparison a

a OR, operating room; OT, occupational therapy; PT, physical therapy; UKA, unicompartmental knee arthroplasty.
b OR supplies includes gowns, drapes, saw blades, cement, and UKA implant charge.
c Surgical facility fee incorporates anesthesia, OR time, and recovery room fees. This is a fixed charge for outpatient surgical facilities.
d Other includes primarily CRNA (certified registered nurse anesthetist) fees and any miscellaneous charges for radiographs, respiratory therapy, electrocardiography, and so on.
This striking difference in cost is a growing trend in the United States health care system. A study published in Health Affairs analyzed data from the National Survey of Ambulatory Surgery and discovered that procedures performed in ASCs are more efficient, taking 25% less time than those performed in hospitals. 19 This efficiency and corresponding cost-effectiveness is due largely to the ASC’s focus on a limited number of procedures, their owner/operator culture, and specialized nursing and support staff. Because ASCs specialize in providing outpatient surgery, they are able to deliver patient-care services efficiently and conveniently. For example, ORs are turned over quickly and are not interrupted by emergency cases. This enables physicians to commence their procedures in a timely manner and use their time more productively. Consequently, ASCs tend to be more convenient and cost-effective than hospital inpatient or outpatient departments while still providing excellent care. Furthermore, facility fees can vary greatly even within the same city based on service offerings and market power, which in turn can affect the negotiated rates and reimbursements with insurance companies. The rates can vary by as much as 500% to 600% for the same procedure at different facilities. The lower cost of care in ASCs relative to hospital outpatient departments saves employers and consumers tens of billions of dollars a year. For the commercially insured population in the United States, an estimated $37.8 billion is saved annually by using ASCs. 21 However, many patients are unaware of the lower costs that ASCs offer.
Correspondingly, there was also a difference in the percent of charges reimbursed by insurance carriers in our study. On the inpatient side, a total of 4 carriers were represented with an average reimbursement of 55% of charges (range, 20%-77%), or $25,550. For outpatients, a total of 4 carriers were also represented with an average reimbursement of 47% (range, 30%-83%), or $12,370. Thus, there is a roughly 50% cost savings when evaluating the actual reimbursement and dollars paid for the procedure by moving from an inpatient to an outpatient setting. With the movement of more procedures to an outpatient setting across all specialties, health plans will reduce their overall costs and are encouraging their customers to be more active and thus reduce their out-of-pocket expenses by identifying physicians who perform these surgical procedures on an outpatient basis. However, as mentioned previously, the long-term growth of ASCs is threatened by the widening disparity in reimbursement that ASCs and hospitals receive for the same procedures.
There was no difference between the inpatient and outpatient groups in terms of complications or readmissions; however, this was only a secondary measure of the study, and due to the small sample size, strong conclusions cannot be drawn. Fortunately, well-done studies discussed in the introduction have demonstrated the safety and feasibility of outpatient UKA. Other studies have also discussed their patient eligibility requirements for outpatient procedures, including total hip arthroplasty, reconstruction of the anterior cruciate ligament, and TKA. In order for patients to undergo outpatient surgery, they had to provide consent; have stable cardiovascular, respiratory, and renal systems; have a caregiver at home after surgery; and live within close proximity to the outpatient center. 3,15 With an appropriate anesthetic and pain control protocol, patients are able to reliably be discharged home on the day of surgery. 8,9 However, not all patients are appropriate outpatient surgical candidates, and those with significant medical comorbidities may require inpatient hospitalization postoperatively. One patient who underwent inpatient UKA was excluded from the cost comparison secondary to an extended hospital stay due to atrial fibrillation.
Our study has several limitations, many of which are in line with other retrospective reviews. Patients were identified with a chart and radiology database search, with all clinical and surgical information gathered from the notes. Because of this limitation, we were unable to identify any differences between surgeries in terms of complexity other than the recorded tourniquet times and analysis of the degree of deformity on preoperative radiographs. We also had small sample sizes in both cohorts, which causes a greater range and variability in all costs. Unfortunately, the hospital billing department does not maintain cost/expense/reimbursement data for greater than a 39-month postoperative period; thus, we were unable to include a large cohort of inpatient UKA patients. Furthermore, the ASA classification system is used to evaluate the degree of a patient’s “physical state” or overall health prior to selecting the anesthetic or before performing surgery. It is used to describe a patient’s preoperative physical status for communication between colleagues; however, the grading system is not intended for use as a measure to predict operative risk. Perhaps a different medical risk stratification score, such as the Outpatient Arthroplasty Risk Assessment Score (OARA score), is more appropriate in determining which patients are safe to undergo outpatient joint replacement surgery. The OARA tool is a 60-question document that risk stratifies patients as either “low risk/appropriate” or “high risk/not appropriate” for outpatient joint arthroplasty. 18 As noted previously, not all patients are appropriate outpatient surgical candidates, and those with significant medical comorbidities may require inpatient hospitalization postoperatively. There can also be significant differences in reimbursement rates depending on the insurance status of the patient. While private payers vary in their reimbursement rates and policies, most are tied in some form to the Medicare system. There were a total of 4 different payers (both private and Medicare) identified in each patient cohort, and reimbursement rates averaged 54.5% (range, 20%-77%) for inpatient UKA versus 47.1% (range, 30%-83%) for outpatient UKA. Finally, evaluating consecutive patients for inpatient UKA versus outpatient UKA also introduces some bias into the study. Patients are not randomized, and thus, with the outpatient UKA protocol there may have been more stringent surgical inclusion criteria (ie, some patients not offered a UKA based on certain medical comorbidities or other factors). In addition, there may have been a more detailed preoperative discussion regarding expectations for discharge home after surgery.
Outpatient and ASCs can offer distinct advantages to patients when compared with hospital inpatient surgeries. They are not only less expensive (sometimes only 25% of the overall cost of an inpatient procedure) but can be easier for patients to navigate and result in overall improved patient satisfaction. Over the past 20 years, the average duration of hospital stay for a TKA has decreased from 9 to 4 days. 12 Several institutions are also experimenting with, and gradually adopting, outpatient TKA as their standard of care. UKA involves less surgical dissection and pain than a standard TKA, with the potential for an accelerated rehabilitation program. Therefore, not only is it feasible to perform outpatient UKA, but it can provide substantial cost savings and a reduction in bed occupancy and resource allocation for a busy hospital.
Conclusion
It is important to understand that while what the patient demands from us (their physicians) is changing, our responsibility for their safety and care has not. The current demographics, time pressure, patient mobility, consumerism, and cost pressures are trends that will continue to change. 17 This work demonstrated that significant cost savings of roughly 50% can be achieved with an outpatient UKA protocol in an outpatient facility.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was waived by the University of Virginia (IRB-HSR # 18459).
Acknowledgment
The authors would like to thank Eric Vess, University of Virginia medical student, for his help with data collection.