
Abstract
Introduction:
Osteoarthritis (OA) of the knee is a growing problem in an aging population. Unicompartmental knee arthroplasties (UKA) have been used for management of isolated OA of the medial tibiofemoral joint. This is the first study on the usage of UKA in Hong Kong.
Methods:
Retrospective analysis of all patients undergoing medial compartment UKA in a tertiary referral center since 2003. Preoperative and postoperative International Knee Society Knee Scores (KSKS) and Knee Societal Functional Assessment (KSFA) scores, range of motion, flexion deformity, and lower limb mechanical alignment were measured. Statistical analysis using paired sample t-tests was performed. Revision operations, rate of revisions, and causes of failure were analyzed. Univariate and multivariate logistic regression analyses of risk factors for revision operation were performed against patient demographics, type of prosthesis, postoperative alignment, and degree of correction.
Results:
There were 94 UKA performed with an average follow-up of 4.3 years (range: 0.5–15.2 years). The KSKS and KSFA scores improved from 54.5 and 54.0 to 85.6 and 64.5 (p < 0.01), respectively. There was no significant improvement in the range of motion (p = 0.87) and fixed flexion deformity (p = 0.14). Mechanical alignment improved from 172.1° to 174.9° varus postoperatively (p < 0.01). Six cases required revision operation with a revision rate of 1.50 per 100 observed component years. Causes of revision included two cases of tibial tray loosening and one case each of progressive OA, mechanical failure, persistent pain, and infection. Logistic regression analysis for risk factors showed no statistical significance.
Conclusions:
UKA offers good functional improvement but further long-term studies are required to evaluate survivorship.
Introduction
Osteoarthritis (OA) of the knee has enormous health-care impact and disease burden with WHO (World Health Organization) estimates a global incidence of 3.8% of the population suffering from OA knee. 1 Studies across Asia have noted a varying prevalence of OA knee ranging from 3% to 38%, highest in Japan and Korea. 1 –3 The lifetime risk of developing OA of the knee was reported to be a staggering 44.7%. 4 It has accounted for 17.5 million years lived with disability. 1
Although there is a higher age-adjusted prevalence of OA knee in the elderly population (>65 years old), a substantial portion of patients present early, before the age of 55. 1,2 This is further reflected by the peak global prevalence of OA knee presenting at 50 years of age. In China, 37% of patients presenting with OA knee are in the range of 50–54 years old. An increasing number of middle-aged patients suffer from pain and disability with difficulty in walking, stair climbing, increased use of nonsteroidal anti-inflammatory drugs, and increased medical consultations. 2,5
In Hong Kong, over 50% of total joint replacements were performed on patients over 70 years old. 6 Management of early OA has typically been by conservative measures with analgesics, physiotherapy, patient education, and lifestyle advice. Young patients with early degeneration were observed for years until significant progression occurs before offering surgical intervention. However, effective surgical intervention in the form of partial knee replacements is available and are used internationally. The most commonly used partial knee replacement is the medial unicompartmental knee arthroplasty (UKA). This replaces the isolated medial tibiofemoral joint, which is often the first to degenerate in varus OA knees (Figure 1). The use of UKA in Hong Kong has not been evaluated in the literature before. This is the first study in Hong Kong to shed light on the trends of UKA usage for management of isolated medial tibiofemoral joint OA over the last 15 years (2003–2017) in a tertiary referral center and university teaching hospital. We evaluated the efficacy, complications, and revision rates of UKA throughout these years.

(a) Intraoperative photograph showing medial compartment OA with eburnation of articular cartilage of the tibiofemoral joint (right) compared to the intact lateral compartment articular cartilage (left). (b) Intraoperative photograph after medial compartment UKA performed. (c) and (d) model of the Oxford unicompartmental knee implant with the metal tibia, femoral components, and a polyethylene liner. OA: osteoarthritis; UKA: unicompartmental knee arthroplasty.
Methods
A retrospective review of all patients undergoing UKA for isolated medial knee OA in Queen Mary Hospital (QMH) and Duchess of Kent’s Children Hospital (DKCH), Hong Kong, from 2003 to 2017, was conducted. Revision operations of UKA and lateral compartment unicondylar arthroplasties were excluded. All records were reviewed by the principal investigator. All UKR were performed by five surgeons (MHC, HCF, PKC, CHY, and KYC) with standard medial arthrotomies from the level of the upper pole of the patella to the tibial tuberosity.
Patient demographics including age, gender, body mass index (BMI), and etiology of OA were recorded. The preoperative functional status of the patients was evaluated using the International Knee Society Knee Score (KSKS) and Knee Societal Functional Assessment (KSFA) Score (see Appendix 1). The preoperative range of motion of the knee, degree of fixed flexion deformity of the knee, and radiographic assessment of the lower limb mechanical alignment with the hip–knee–ankle (HKA) angle were also recorded. This is the angle subtended by a line drawn from the center of the femoral hip ball to the center of the tibial spine eminence and a line from the tibial spine eminence down to the midpoint of the talar surface at the ankle joint as shown in Figure 2. This angle indicates the mechanical axis of the lower limb with larger angles representing greater varus malalignment. Overcorrection or under-correction of the lower limb mechanical alignment may cause increased loading on the lateral tibiofemoral joint or the prosthesis, respectively, ultimately, leading to early failures requiring revision operations. 7

(a) Measurement of the HKA angle for mechanical alignment as depicted by the angle α in the preoperative standing lower limb radiograph on the left in a patient with medial compartment OA. (b) Postoperative standing lower limb X-ray on the right of the same patient with correction of varus mal-alignment. (c) Radiograph of a typical case of isolated medical compartment knee OA with UKA performed in (d). OA: osteoarthritis; UKA: unicompartmental knee arthroplasty; HKA: hip–knee–ankle.
Clinical outcomes measured included the postoperative KSKS and KSFA values to assess the efficacy of UKA in improving patient function. The postoperative differences in knee range of motion, fixed flexion deformity, and postoperative mechanical alignment were also measured. Statistical analysis for comparison of preoperative and postoperative assessments was made using paired sample t-tests with software SPSS version 25.0 (SPSS Inc., Chicago, Illinois, USA).
Assessing the surgical option of UKA from a health-care economic standpoint, the hospital in-patient length of stay, postoperative complications, revision operations, and time to revision surgery were also evaluated. As the follow-up intervals of each patient were different, the revision rates of UKA were calculated in terms of revisions per 100 observed component years. This calculation is made by dividing the total “observed component years at risk” by the number of revisions. The former is defined by the cumulative time from index operation to revision surgery, death or most recent follow-up, whichever is shortest for each patient. This is the total time the prosthesis is at risk of failure. The causes for revision surgery and modes of failure were also determined. Univariate analysis of possible risk factors associated with higher rate of revision including patient’s age, sex, weight, BMI, type of prosthesis, diagnosis, postoperative alignment, and overcorrection to within 3° of the mechanical axis were performed using χ 2 and independent t-tests. Binary logistic regression was used for multivariate analysis of the same risk factors to determine the significance and odds ratio.
Results
There were a total of 94 UKA performed for medial compartment OA over the past 15 years. Forty-nine of which were female (52%). The age at the time of operation ranged from 49 to 82 years, with a mean age of 66. The detailed demographics are shown in Table 1. Primary OA accounted for the majority of etiological diagnosis (94%) with the remaining five cases due to osteonecrosis of the medial femoral condyle. The mean follow-up time was 4.3 years (range: 0.5–15.2 years, SD: ±3.7). The mean follow-up period was relatively short because of a large proportion of UKA being performed in the past 2 years.
Baseline demographics and univariate and multivariate analyses on risk factors for requiring revision.

SD: standard deviation; HKA: hip–knee–ankle; OA: osteoarthritis; UKA: unicompartmental knee arthroplasty; BMI: body mass index; R 2: 0.36, ±standard deviation.
aHKA angle for mechanical axis and lower limb alignment.
Statistically significant values are bolded.
For the clinical outcomes, the mean preoperative range of motion was 118.6° (range: 85–140°, SD: ±184.7), which showed no significant difference compared to the postoperative range of motion (p = 0.87) as shown in Table 2. There was a slight improvement of fixed flexion deformity of the knee which was not statistically significant (p = 0.14). All clinical assessment scores showed a significant improvement postoperatively. The mean operative KSKS was 54.5 which improved by 31.1 postoperatively (p < 0.01, 95% CI: 25.4–36.8). The KSFA scores, which address the patient’s functional ability, showed a significant improvement by an increment of 10.5 from a mean preoperative score of 54.0 (p = 0.01, 95% CI: 4.4–16.8). There was also an overall improvement in lower limb mechanical alignment with the intention of surgical under-correction of the varus mechanical malalignment to avoid overloading of the lateral compartment of the knee which could hasten the progression of lateral compartment OA. Radiographic assessment of mechanical alignment of the lower limb showed a mean correction from 172.1° varus malalignment preoperatively to 174.9° varus postoperatively (p < 0.01, 95% CI: 1.94–3.71).
Clinical outcomes.

FFD: fixed flexion deformity; HKA: hip–knee–ankle; KSFA: Knee Societal Functional Assessment; KSKS: International Knee Societal Knee Score.
Statistically significant values are bolded.
The average in-patient length of stay for those undergoing UKA was 6.3 days (range: 2–23 days, SD: ±19.4). However, 16 patients (17%) were able to be discharged the same day after surgery, achieving a total in-patient stay of only 2 days. A length of stay of 2 days accounted for 31% of the patients operated within the last 2 years. Fifty-three percent of patients were discharged by the third day after operation. There were no immediate postoperative complications in our experience.
Separate analyses for comparison of UKA cases before and after 2016 were also performed. There were 41 UKA cases performed before 2016 with an average follow-up of 7.3 years (range: 0.5–15.2, SD: 3.72) compared to 53 UKA cases performed after 2016 with an average follow-up of 1.9 years (range: 0.6–2.2, SD: 0.51). Baseline characteristics including age, gender, BMI, preoperative flexion range, preoperative HKA alignment, and KSKS and KSFA scores were not significantly different as shown in Table 3. Functional outcomes were not significantly different (p > 0.05). There was a slight improvement in functional scores in the short-term follow-up group with an improvement of the KSKS by 35.0 compared to 27.4 in the long-term group although not statistically significant (p = 0.22). There was also a significant improvement in length of stay from 8.6 days down to 4.5 days in operations performed more recently, which was statistically significant (p < 0.01). This may be attributable to better postoperative care and rehabilitation. We have been adopting fast track arthroplasty and enhanced recovery after surgery rehabilitation protocol for all joint replacement patients since 2016, which has invariably improved hospital length of stay. There was otherwise no change in discharge policy for the study duration. From the cases performed before 2016, there were a total of five cases requiring revision operation compared to only one case from cases performed more recently (p = 0.04).
Comparison between long-term and short-term groups.

FFD: fixed flexion deformity; HKA: hip–knee–ankle; KSFA: Knee Societal Functional Assessment; KSKS: International Knee Societal Knee Score; BMI: body mass index.
Statistically significant values are bolded.
Thus, a total of six patients required revision operation after their initial surgery. The overall implant survivorship in our cohort was 91.4%. The meantime to revision operation was 1.85 years after the initial index operation. In our cohort of UKA performed in Hong Kong, the revision rate was 1.50 per 100 observed component years. There was a total of 400 observed component years from index operation to revision or latest follow-up in 94 UKA operations since 2003. The causes of revision included two cases of tibial tray loosening, and one case each of progressive lateral compartment OA, mechanical failure due to undersized femoral component, persistent postoperative pain, and delayed peri-prosthetic joint infection. Functional outcomes were worse in cases requiring revision operation, KSKS scores dropped from 50.8 to 47.8 postoperatively while KSFA scores also declined by 10 from a preoperative score of 31.3. Univariate analysis of risk factors showed no statistical significance in differences for age, gender, BMI, postoperative alignment, laterality, and diagnosis (p > 0.05). However, four of the six revision operations required occurred with the DePuy Preservation implant, which is no longer used (p = 0.01). Logistic regression analysis for the same risk factors showed no statistical significance (p > 0.05) as shown in Table 1.
Discussion
There is a rising incidence of OA with the aging population worldwide. 1 –4 Moreover, a distributional shift has been noted with an increasing incidence of OA diagnosed at a younger age. 1,2 Diagnosis of OA knee was shown to peak at 55 years of age in 2013 compared to 70 years of age in the 1990s. 8 Medial tibiofemoral compartment involvement is seen in 87% of knee OA, including cases with mild OA and those with varus malalignment of the lower limbs. 9,10 Treatment should include a holistic and multidisciplinary approach with patient education, exercise training, weight reduction, and appropriate pharmacological management. 11 Where conservative management has failed, surgical intervention can be offered to relieve pain and improve patient function.
UKA has been widely used to treat isolated compartmental knee OA. UKA was first introduced in the 1960s but has gained popularity over the last decade with better understanding, improving instrumentation and patient selection. 7 The number of UKA performed has increased in North America, New Zealand, Australia, and Norway according to their respective national joint registries. 12 –16 In the United States, the overall number of UKA performed rose from 1658 in 2012 to 4701 in 2016. Australia and Norway have also showed a rise in UKA as a percentage of knee arthroplasties performed. The largest increase was seen in Norway with a UKA utilization rise from 9.4% to 13.3% of all knee arthroplasties from 2010 to 2016. 12 The United Kingdom and Swedish joint registries have a UKA steady utilization rate of 8% of all their knee arthroplasties performed. 17,18 However, Sweden and Finland in particular have noted a drop in total numbers of UKA performed in the latest annual report, citing increased revision rates as the reason for decrease in UKA utilization. 17,19 UKAs are performed on younger patients with the average age being 6–10 years younger compared to those undergoing total knee replacements (TKRs). 12,18 In Hong Kong, our center has noted an increase in UKA performed over the last 2 years (2016–2017) with 28 UKA performed in the last year alone as shown in Figure 3. This renewed interest in UKA is due to better instrumentation and technique such as navigation or robotic-assisted surgery as shown in Figure 4.

Number of UKA performed annually. UKA: unicompartmental knee arthroplasty.
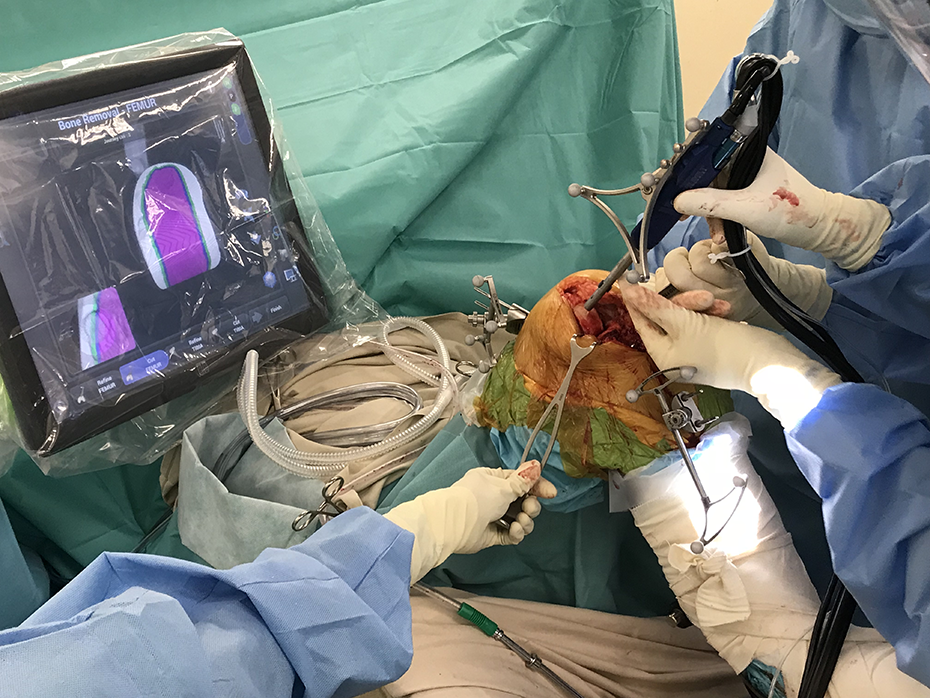
Demonstrating medial femoral condyle bone resection for a UKA using robotic-assisted technology at the Duchess of Kent’s Children Hospital joint replacement center. UKA: unicompartmental knee arthroplasty.
UKA provides unique advantages when compared to total knee arthroplasties as it allows for preservation of bone stock, retention of the cruciate ligaments, less intraoperative blood loss, a faster recovery, higher activity level, and a more normal feeling of the knee. 7,20,21 From the New Zealand Joint Registry, they showed that 83% of patients who had undergone UKA had excellent to good post-operative satisfaction scores compared to only 74% of TKR patients. 16 Lyons et al. showed higher preoperative and postoperative functional scores in UKA compared to TKR but no difference in incremental changes postoperatively. 20 From a meta-analysis, Arirachakaran et al. illustrated that UKA had no difference in functional outcomes including KSKS, range of motion, and pain improvement compared to TKR. 22 They also noted less postoperative complications including deep vein thrombosis, fractures, and infection, albeit higher revision rates for UKA were seen. Our cohort shows similar results with good functional improvement and fast recovery periods with shorter in-patient lengths of stay.
But indeed, higher revision rates are the major drawback to UKA compared to TKR. In New Zealand, they noted a revision rate of 1.24 per 100 observed component years and a 15 year implant survival rate of 81.1%. 16 Revision rates for UKA were similar in Australia and Sweden with 1.90 and 1.15 per 100 observed component years, which were significantly higher than TKR revision rates of 0.83 and 0.71 per 100 observed component years, respectively. 23 In our study, we noted a revision rate of 1.50 per 100 observed component years with an overall implant survival of 91%. Our revision rates per component years are similar to international data, the slightly higher revision rates compared to New Zealand and Sweden can be explained by the shorter average follow-up period of 4.3 years skewed by the increase in UKA performed in the recent 2 years. A longer follow-up period is required for a better reflection of revision rates compared to international standards. A study from Finland noted poorer UKA survivorship of 80.6% at 10 years and 69.6% at 15 years compared to 93.3% and 88.7% for TKR, respectively. 19 Higher revision rates in UKA compared to TKR can be accounted for by various factors. Generally, UKA are performed in younger individuals with higher functional demand, especially at an earlier stage of OA. A previous study noted that UKA performed in patients <55 years old had a significantly increased rate of revision by 7% compared to those older than 65 years old. 24 This may be attributable to higher functional demand and activity level. UKAs performed in older individuals over 75 years of age had the same outcome, revision rates and 5-year implant survivorship compared to their TKR counterparts but with the added benefit of shorter hospital stay, less blood loss, and higher level of activity upon discharge. 21 Patient selection with isolated medial tibiofemoral compartment disease and functional level is thus crucial for implant survivorship. Another reason for higher revision rates seen in registries is the ease of revision surgery for UKA. Often, conversion to TKR is sufficient as a revision operation, and functional outcomes are comparable. 7 This may account for a lower threshold for revision surgeries in patients who had undergone UKA.
A systematic review found the most common causes of UKA failure among 3967 medial UKA were aseptic loosening (36%), followed by OA progression (20%) and pain (14%). 25 Similarly, in our cohort, we had two cases of tibia tray aseptic loosening as a cause of early failure with a mean time to revision surgery of 3.5 years. A multicenter analysis showed that the majority of aseptic loosening cases occurred in the early period with 37.7% of cases occurring within 2 years postoperatively. This occurred much earlier compared to progressive OA and implant wear, which occurred at 7.75 and 9.3 years after the initial operation, respectively. 26 From this study, we noted an average time to revision of 1.85 years from index operation. Further follow-up data are required to note whether the recent increase in UKA procedures done after 2016 will see similar fate in early revision surgery. Moreover, technical reasons accounted for 11.5% of early failures including mal-positioning, major under-correction, or overcorrection of lower limb alignment. Several studies have denoted that high-volume centers and surgeons who performed more UKA per annum had significantly lower revision rates. 27,28 Surgeons performing less than 25 cases per annum had 5.9% lower 5-year survivorship compared to high volume (over 200 UKA per year) surgeons. 27 This illustrates the importance of the technical aspects for performing UKA in addition to patient selection in prevention of early revisions.
Improvements in instrumentation and surgical technique have led to better accuracy and reduction in technical errors. In our study, the majority of revision cases occurred in implants now obsolete (Preservation and Miller-Galante) with only one case occurring in the ZUK (Zimmer Unicompartmental Knee) modern day implant, still being used now. Due to small sample size and low revision numbers, we were unable to provide considerable values for individual prosthesis in the multivariate logistic regression analysis. Longer follow-up is needed to confirm better survivorship of newer implants. However, international data from various joint replacement registries have shown promising results. Apart from improvement in instrument design, additional assistive devices such as computer navigation surgery and robotic-assisted surgery help to improve accuracy in implant positioning and correction of alignment. 29 –31 With the hopes that this technology can help reduce technical reasons leading to early revision surgeries, revision rates for UKA may show an improvement in the future.
In conclusion, there is a rising number of UKA performed in our center for isolated medial compartment OA and has been shown to have good clinical efficacy and improvement in clinical outcome scores. This is the first study to evaluate UKA in Hong Kong. It echoes similar findings to other studies done internationally showing relatively higher early revision rates. Patient selection and surgical technique are imperative for UKA success. Hence, thorough discussion with patients on the risks and benefits of UKA versus TKR is a must before surgical intervention. Further studies and long-term follow-up data are required to show the effects of improved instrumentation systems and assistive technology.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.