
Abstract
Obesity is a known major contributing risk factor for knee osteoarthritis (OA). It is also believed that obese unicompartmental knee arthroplasty (UKA) patients tend to have poorer outcome and possible early failure. The purpose of this study is to investigate the early outcome of obese UKA patients in a single institution. Patients who underwent fixed bearing medial UKA in between year 2005 and 2010 were included in this study. They were divided into four groups based on Body Mass Index (BMI): 25 kg/m2 (Control); 25–29.9 kg/m2 (Overweight); 30–34.9 kg/m2 (Obese); >35 kg/m2 (Severely Obese). Functional outcome was assessed using Knee Society Score (KSS), Oxford Knee Score (OKS) and Short-form 36 (SF-36). One-way ANOVA with Bonferroni post-hoc test was used to compare the four groups for quantitative variables. There were 673 patients in this study, no significant difference between the four BMI groups for gender and side of operated knee (p > 0.05). The functional outcome of all four groups at 2 years were comparable (all p > 0.05). At a mean follow up of 5.4 (range 2.5, 8.5) years, 9 revision surgeries (1.3%) were identified. The mean duration from initial surgery to revision surgery was 49 months (Range 6, 90). Patients’ pre-operative BMI did not influence the early outcome of UKA patients. However, patients with higher BMI had relatively lower functional score prior to the surgery and tended to be younger. This did not translate to early failure and the functional improvement was similar among all four groups.
Introduction
Unicompartmental knee arthroplasty (UKA) had been a common surgical treatment 1 for single compartment osteoarthritis (OA) other than total knee arthroplasty (TKA) and high tibial osteotomy (HTO). The outcome of UKA is comparable with TKA, 2 having the advantages of lesser bone resection, lower risk of infection, lesser thromboembolic event, reduced length of hospitalization 3 and early functional recovery. 4 Furthermore, preservation of the anterior and posterior cruciate ligaments with intact patellofemoral joint (PFJ) and meniscus may allow the operated knee mimicking near normal knee kinetics. 5,6 Despite having such reported advantages, patients who underwent UKA surgery were known to have a higher risk of revision as compared to patients who had TKA surgery. 7
Careful patient selection is vital to ensure a good outcome of UKA surgery, minimizing the risk of UKA failure and the need of revision surgery. Kozinn and Scott 8 had proposed that the best candidates for UKA surgeries were those who were older than 60 years with low physical demand, minimum rest pain, preoperative arc of flexion of at least 90°, flexion contracture of less than 5°, limited angular deformity, intact anterior cruciate ligaments, no OA in the contralateral compartment and no patellofemoral pain. An ideal weight of less than 82 kg (180 lb) for patients undergoing UKA surgery had been recommended as well.
High body mass index (BMI) had been identified as one of the major contributing risk factors for OA of the knee, and there had been documented trend towards a rising prevalence of high BMI and OA in younger patients. 9,10 As obesity has become pandemic in both developing and developed countries in recent decades, strict patient selection based on weight had not always been possible. Furthermore, some surgeons were reserved in offering UKA to obese patients in fear of the possible complications and adverse outcomes.
The purpose of this study is to compare the early functional outcomes, survival and complication rates of UKA in patients with normal BMI to those who were overweight and obese.
Methods
After obtaining approval from the Centralized Institutional Review Board (CIRB 2013/471/D), a review of medical records was conducted in all patients who underwent UKA at a tertiary hospital between year 2005 and 2010, and who had a minimum of 2-year follow-up. Patients who had bicompartmental knee arthroplasty or lateral UKA were excluded from this study. All surgeries were performed by five experienced adult reconstruction surgeons using medial parapatellar approach. The implants used in all surgeries were cemented fixed-bearing implants. Preoperative demographic data such as patients’ age, gender, height and weight at the time of surgery were documented.
The patients who underwent UKA procedure were those who experienced medial knee pain with radiographic evidence of degenerative joint disease confined to medial compartment only and no evidence of patellofemoral disease. They all had intact anterior cruciate ligament and without significant deformity (varus malalignment less than 15°, valgus malalignment less than 10°, fixed flexion deformity of less than 5° and flexion more than 90°). 11,12 No patients were excluded because of weight or BMI. The patients were divided into four groups based on BMI at the time of surgery; group 1: BMI less than 25 kg/m2 (control), group 2: BMI between 25 kg/m2 and 29.9 kg/m2 (overweight), group 3: BMI between 30 kg/m2 and 34.9 kg/m2 (obese) and group 4: BMI ≥ 35 kg/m2 (severely obese).
Pre- and post-operative clinical outcomes were evaluated using the Knee Society Score (KSS), Oxford Knee Score (OKS) and Short Form Health Survey (SF-36). All of them were followed up prospectively and the functional outcome was assessed at 2 years post-surgery. Complications including infection, 30-day readmission, post-operative stiffness, deep vein thrombosis, fracture and persistent pain after surgery were noted. Failure was defined as the need for revision surgery without an infective cause. Revision to TKA was performed or recommended to all failed UKA patients.
Statistical analysis was conducted using SPSS® 19.0 (IBM, Chicago, Illinois, USA). Comparisons of KSS, OKS and SF-36 scores among the four groups preoperative and at 2 years after surgery were performed. The change of each score based on BMI was analysed as well. The one-way analysis of variance with Bonferroni post hoc test was used to compare the age of patients in the four groups, while the Pearson χ 2 test was used for categorical variables such as gender, side of operating knee and number of UKA failures. To limit the confounding effect of patient’s age, which is known to influence functional outcome in UKA surgeries, multiple linear regression was used to adjust the preoperative, 2 years post-operative and change in functional outcome scores observed in the four BMI groups. This adjustment effectively accounts for any differences in the distribution of patient’s age and its influence on the functional outcome scores within each of the BMI groups. Statistical significance was defined as a p value of <0.05.
Results
Between 2005 and 2010, there were a total of 966 knees operated among 901 patients. After excluding patients with lateral UKA and bicompartmental knee arthroplasty, 673 patients had completed at least a 2-year follow-up. Majority of the patients were females (502 patients) with female-to-male ratio of 2.96:1. Mean age of the patients was 62 years old (range 45–88) at the point of surgery being performed. There were a total of 365 right knees being operated on as compared to 308 left knee (1.19:1). Sixty-five patients had undergone simultaneous bilateral UKA surgeries, while 46 of them had staged UKA; both knees undergone surgery in different hospitalization. The average height of our patients was 156.2 cm with average weight of 66.1 kg. This gave rise to mean BMI of 27.08 kg/m2.
Out of the 673 patients, 230 patients had a BMI of less than 25 kg/m2 (control), 289 patients were overweight (BMI: 25–29.9 kg/m2), 124 obese patients (BMI: 30–34.9 kg/m2) and 30 severely obese patient (BMI ≥ 35 kg/m2). The mean age, BMI and post-operative tibiofemoral angle, as well as gender and side of surgery for each group, were further stratified in Table 1. Severely obese patients noted to have lower mean age (p < 0.001).
Patients’ demographics and post-operative alignment.

BMI: body mass index.
Preoperatively, the average KSS function score for all four groups was 61 ± 16, knee score of 43 ± 18 and OKS of 33 ± 8. This had improved to 80 ± 17, 87 ± 12 and 18 ± 5 post-operatively at 2 years. Preoperative average range of motion was 5–128°, which improved to an average of 3–129° at 2 years.
The breakdown of the KSS function score, KSS knee score, OKS, SF-36 physical component score and SF-36 mental component score corrected for patients’ age were as shown in Table 2.
Functional outcome scores.

KSS: Knee Society Score; OKS: Oxford Knee Score; SF-36: Short Form Health Survey.
Compared to control, overweight and obese groups, the preoperative KSS knee score was lower in the severely obese group by 11 (95% confidence interval (CI) 5, 18), 10 (95% CI 4, 17) and 13 (95% CI 7, 21) points, respectively (p = 0.001, p = 0.002 and p < 0.001, respectively). Similarly, the preoperative OKS was poorer in the severely obese group by 5 (95% CI 2, 8), 4 (95% CI 1, 7) and 4 (95% CI 1, 8) points, respectively (p < 0.01, p = 0.003 and p = 0.004, respectively). The preoperative SF-36 physical component score was also lower in the severely obese group by 5 (95% CI 2, 9), 4 (95% CI 1, 8) and 4 (95% CI 1, 8) points, respectively (p = 0.001, p = −0.015 and p = 0.011, respectively).
However, at 2 years after surgery, there was no significant difference between patients having different BMI, and the improvement in these scores was comparable. Likewise, there was no any significant difference of note in KSS function score and SF-36 mental component score among the four different BMI groups of patients.
A total of six patients (0.9%) who sustained periprosthetic fracture were identified. All of them sustained fracture at the medial tibial plateau, and almost all occurred in 1 month after surgery. One patient had fracture occurred 5 months post-operative due to trauma. Half of the fracture UKA patients had normal BMI, and the remaining patients were overweight, obese and severely obese each. All of them were offered revision surgery to TKA but only one patient agreeable for such procedure. The rest of the patients had a cast applied onto the affected limb and advised on non-weight bearing for 6 weeks. They subsequently underwent physiotherapy sessions to improve post-casting stiffness. The average KSS function and knee scores of these patients were 70 and 28 preoperatively, 80 and 80 at 6 months after surgery and 90 and 91 at 2 years after surgery, respectively. The mean OKS for this group of patients also improved from 33.5 before surgery to 19 at 6 months post-surgery and 17.5 at 2 years.
The mean follow-up of the patients in this study was 5.4 (range 2.5–8.5) years. The complication rate was 5 (2.2%), 10 (3.5%), 5 (4.0%) and 2 (6.7%) in the control, overweight, obese and severely obese groups, respectively (p = 0.931). Eight patients had a superficial wound infection (two normal, three overweight, two obese and one severely obese). All of them were treated with intravenous antibiotics and two had surgical debridement done. No deep wound infection was noted in this series. There were three patients suffered from post-operative stiffness (two normal and one overweight), of which, they underwent manipulation under anaesthesia and improved. One patient from the overweight and obese group each developed deep vein thrombosis. Three patients were readmitted within 30 days due to superficial wound infection.
A total of nine revision surgeries (1.3%) were identified. The breakdown of reason for revision based on group is shown in Table 3. The mean time for revision was 49 months (range 6–90).
Causes of revision surgery.
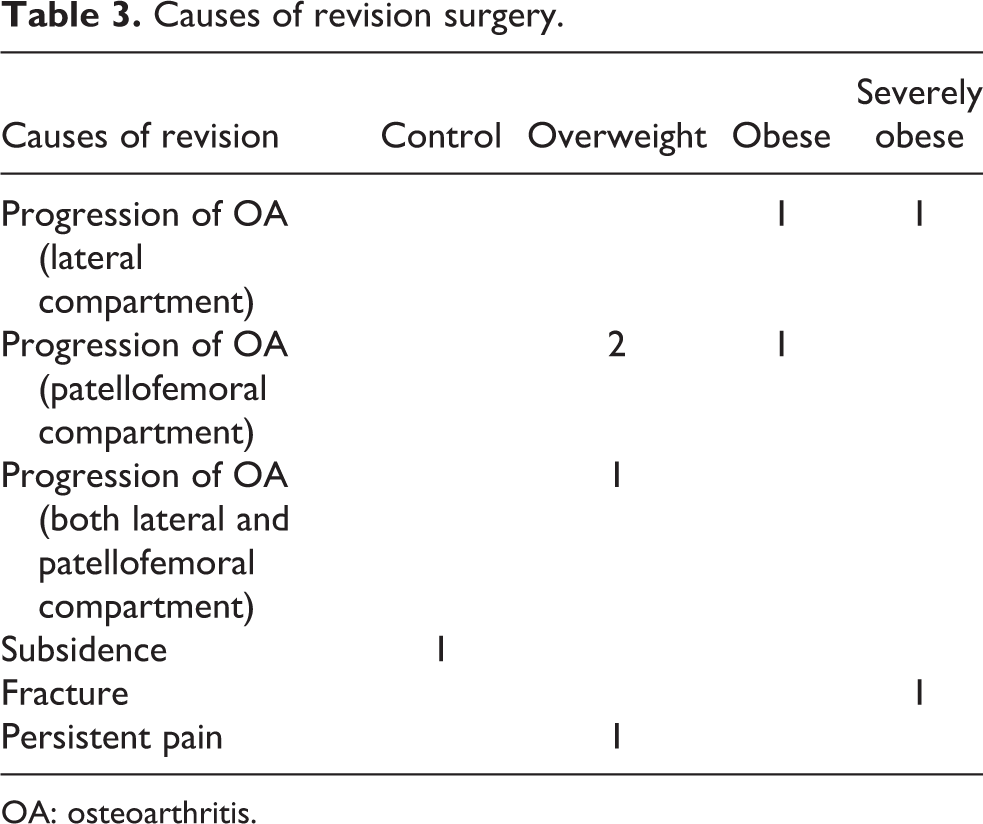
OA: osteoarthritis.
Discussion
UKA is known to have significant advantages over both HTO and TKA 13 for patients with isolated OA of a single compartment of the knee. However, some authors had reported high rate of conversion to TKA in UKA patients. 14 Progression of OA 15 had been identified as a primary mode of failure along with other reasons such as polyethylene wear and loosening of components. 16 Therefore, careful patient selection, such as avoiding surgery in obese patients, had been accounted to safeguard the success of UKA surgery. However, in recent years, obesity had been a controversial issue for patients undergoing UKA surgery. As most populations worldwide are suffering from the pandemic of obesity, various studies had been conducted to evaluate the influence of high BMI towards the outcome of UKA surgery.
Conventionally, patients with higher BMI were thought to have poorer outcome with risk of early implant failure. In a series of 79 patients by Berend et al., 17 early implant failure rate of 22% at a mean follow-up of 40.2 months (range 24–49 months) was being reported. The failures were due to tibial loosening, tibial plateau fracture, persistent medial pain, progressive arthritis and sepsis. Hence, the authors suggested that UKA patients with a BMI greater than 32 were associated with a reduced survivorship. Similarly, Peter et al. 18 had addressed higher (12.5%) failure rate was found in the more obese group of UKA patients. A multicentre study consisting 294 patients was conducted by Heck et al. 19 revealed that the patients who had revision surgery performed had a mean BMI of 32.6 kg/m2 compared with 24.7 kg/m2 in the unrevised group. A significantly higher risk of failures in patients heavier than 81 kg was also reported.
Conversely, Cavaignac et al. 20 had showed that obesity had no adverse outcome in UKA patients with 10-year survival rates of 93%. In a study by Xing et al. 21 with 178 patients, the outcome of UKA was not influenced by patient’s age, BMI and early degeneration in the PFJ. Furthermore, the clinical outcome of the 1000 mobile-bearing UKA at a mean of 5.6 year in a prospective study by Pandit et al. 22 was similar for both patients weighing less and more than 82 kg. Tabor et al. 23 reported higher survivorship among obese patients compared with those who were not obese in a 20-year follow-up study of 82 patients.
We have showed in this study that obesity did not guarantee a poorer early outcome for UKA patients. Although obese patients had poorer preoperative KSS – knee score and OKS, the improvements of the respective scores were similar as compared to the normal BMI group. Also, patients with higher BMI in this study did not show increased risk of periprosthetic fracture or the need of revision surgery. Patients who had revision surgery done due to progression of OA were all found to have abnormal BMI.
In contrast to the other studies, 89.3% (601) of our patients weighed less than 82 kg and 95.2% (641) of them were less than 90 kg. They did not meet the absolute weight criteria (82 and 90 kg) as suggested by the other authors 8,24 as a contraindication of UKA surgery. As the Asian population has shorter stature as compared to the Caucasians, less weight is needed to achieve higher BMI. We also noticed that higher BMI patients tend to have UKA surgery done at a younger age. This may be due to early long-term exposure to excessive stress onto their knee joints, which had resulted in early wear. As younger patients are generally more active and had longer lifespan, they are more predisposed to risk of implant wear and subsequent revision surgery in future.
There are limitations in this study. This is a retrospective study of prospectively gathered data. The surgeries were carried out by different surgeons thence; surgical technique (conventional vs. minimally invasive) and post-surgery management differ between surgeons. Although the follow-ups were up to a mean of 5.4 years, no outcome scoring was carried out beyond 2 years after surgery.
Conclusion
Obesity does not influence the early outcomes of UKA. The functional outcome scores at 2 years after surgery and improvement in these scores were comparable to patients with normal BMI. Furthermore, the complication and revision rates were comparable. Hence, obese patients shall not be excluded from the benefit of UKA surgery.
Footnotes
Authors’ Note
All authors have participated in the research for this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.