
Abstract
Background:
Favorable outcomes have been reported regarding postoperative shoulder pain and function after repair of anteroinferior (Bankart) glenohumeral labral tears. However, the outcomes of patients after repair of isolated superior labral anterior-posterior (SLAP) tears are a contentious topic. The authors have also anecdotally noted that patients evaluated with labral tears complained of numbness and tingling in their ipsilateral hand.
Purpose:
To determine if there is a difference in the temporal outcomes of shoulder pain and hand paresthesia in patients with SLAP tears versus Bankart tears after arthroscopic repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 66 consecutive patients who underwent arthroscopic labral repair at a single institution between August 2018 and February 2021. The prevalence and magnitude of shoulder pain as well as numbness and tingling of the hand were assessed using questions from the L’Insalata Shoulder Questionnaire and the Boston Carpal Tunnel Questionnaire preoperatively and at 1 week, 6 weeks, 12 weeks, and 6 months after surgery.
Results:
Preoperatively, patients with SLAP lesions reported a higher prevalence of shoulder pain during sleep compared with those with Bankart tears (P < .05). Postoperatively, patients who underwent SLAP repair reported a larger proportion and more severe magnitude of shoulder pain during rest, overhead activities, and sleep compared with those who underwent Bankart repair (P < .05). Only patients who underwent Bankart repair reported improvements in the prevalence and magnitude of their shoulder pain during rest, overhead activities, and sleep by 6 months postoperatively compared with preoperative levels (P < .05). Preoperatively, 30% of patients with Bankart repairs and 40% of patients with SLAP repairs reported hand tingling, while 35% and 50%, respectively, reported hand numbness. The prevalence and magnitude of hand tingling and numbness were not significantly different between groups at any time point.
Conclusion:
Study results indicated that patients who underwent SLAP repair experienced worse shoulder pain outcomes compared with those who underwent Bankart repair using the same anchor and surgical technique. Only patients who underwent Bankart repair reported improvements in their hand numbness after surgery. Therefore, labral tear location does matter with respect to shoulder pain and hand numbness.
Keywords
Damage to the glenohumeral labrum is common, often arising after traumatic anterior shoulder dislocation (>95%). 32 The most typical sequelae of an initial dislocation include severe shoulder pain and episodes of recurrent instability, particularly in young patients. 17 Arthroscopic repair of this lesion is the most common surgical management of anterior instability, 13 with favorable outcomes in postoperative pain, range of motion (ROM), and instability recurrence rates. 1,5,8 Damage to the anteroinferior glenoid labrum (Bankart lesion) is present in >90% of traumatic anterior shoulder dislocations. 23
The superior glenoid labrum can also be damaged via a traumatic load through the long head of the biceps. 7 Concomitant superior labral anterior-posterior (SLAP) and Bankart lesions occur in >20% of anterior instabilities, 30,35 in which the presence of the SLAP lesion significantly exacerbates shoulder instability. 11 The outcomes of operative repair of isolated SLAP lesions are an area of contention. Several studies have found that patients with SLAP lesions present with significant shoulder pain, which improves along with shoulder function after arthroscopic repair. 3,9,27 However, Schrøder et al 28 performed a double-blinded trial comparing sham surgery with labral repair or biceps tenodesis in patients with SLAP lesions and found no clinical benefit of SLAP repair. Murphy et al 20 compared the clinical outcomes of patients who underwent Bankart, SLAP, or combined Bankart and SLAP repair. They found that patients who underwent isolated SLAP repair had more pain both preoperatively and at 6 months after surgery compared with those who had isolated Bankart and combined Bankart and SLAP repair.
Numbness and tingling of the hand have traditionally been associated with compression neuropathies of the upper limb, namely carpal tunnel syndrome, cervical radiculopathy, and thoracic outlet syndrome. 24 Despite this, we anecdotally noted that a large proportion of patients evaluated with labral pathologies complained of numbness and tingling in their ipsilateral hand. We were only able to identify 1 study that has investigated the relationship between hand paresthesia and shoulder conditions. Sivan et al 29 performed a clinical observation study on 100 consecutive patients undergoing surgery for subacromial impingement of the shoulder. They found that 54% of patients reported paresthesia symptoms (tingling, pins and needles, burning, or woolly sensations) of the ipsilateral hand. However, it is undetermined whether patients with labral tears also experience hand numbness and tingling. We were accordingly interested in evaluating the association (if any) between glenohumeral labral tear location, shoulder pain, and paresthesia before and after labral repair.
The aim of this study was therefore to answer the following questions: Is there a difference in the temporal outcomes between patients with a surgically reattached (SLAP) tear versus (Bankart) tear? Specifically, is there a difference in patient-reported prevalence and magnitude of shoulder pain and hand paresthesia in patients undergoing SLAP versus Bankart repair? We hypothesized that patients who undergo SLAP repair would report a higher prevalence and severity of shoulder pain and hand paresthesia.
Methods
Study Design
This study was a prospective analysis of the prevalence and magnitude of shoulder pain and hand numbness and tingling among patients who presented for arthroscopic labral repair. This was part of a larger investigation of hand paresthesia among patients who came to our clinic with a shoulder problem. We performed a post hoc analysis specifically on patients who underwent labral repair. To be included, patients must have had undergone either SLAP or Bankart repair for shoulder instability and/or shoulder pain and completed a shoulder questionnaire before surgery. Patients underwent surgery at a single institution by a single surgeon (G.A.C.M.). Patients were excluded from the study if they had previous surgery on the same shoulder. Ethics approval was received for the study protocol. Patients provided informed consent for the use of their details in this study.
This study assessed the prevalence and magnitude of shoulder pain and numbness and tingling of the hand in this population preoperatively and at 1 week, 6 weeks, 12 weeks, and 6 months postoperatively. At each point, patients were asked to complete a questionnaire (Appendix Figure A1). The following questions of the L’Insalata Shoulder Questionnaire were used to determine the prevalence and magnitude (none/mild/moderate/severe/very severe) of shoulder pain: “How often is your shoulder painful during activity/painful when you sleep/extremely painful?” “What is the level of your shoulder pain when you are resting/with activities above your head/when you sleep?” “How ‘stiff’ is your shoulder?” “How much difficulty do you have with reaching behind your back/with activities above your head?” “How is your shoulder overall?”
To assess hand numbness and tingling symptoms, we used a well-cited questionnaire (the Boston Carpal Tunnel Syndrome Questionnaire [BCTQ]), which has been validated in its use to assess symptom severity and functionality in patients with carpal tunnel syndrome. 15 We used it outside of its validated purpose because there are no shoulder scoring systems that include an assessment of hand numbness and tingling. Accordingly, we utilized 2 questions from the BCTQ in this study: “Do you have tingling sensations in your hand?” and “Do you have numbness (loss of sensation) in your hand?” Patient responses were assessed using the standard responses of the BCTQ (none/slight/medium/severe/very serious).
In addition, patients underwent a standardized examination of their shoulder preoperatively and at 6 weeks, 12 weeks, and 6 months postoperatively (see the Appendix Figure A1). Examiners visually measured patient shoulder ROM in passive forward flexion, abduction, external rotation, and internal rotation according to a validated protocol. 25 Examiners also measured patient shoulder strength in internal rotation, external rotation, abduction in the scapular plane (supraspinatus), liftoff, and adduction using a handheld dynamometer according to validated protocols. 4
Surgical Technique
All procedures included in this study were performed by a single shoulder surgeon. Patients received a regional interscalene block using 0.75% ropivacaine and 2% lignocaine with adrenaline (1:100,000) and were placed in the beach-chair position. A standard posterior viewing portal was created to complete arthroscopic evaluation of the glenohumeral joint.
An anterior-superior portal was established along with an anterior-inferior portal for Bankart repairs and a superior-lateral portal for SLAP repairs, as described by O’Brien et al. 22 Sutures were placed through the detached labral tissue, and drill holes were created using a drill for the placement of anchors on the margin of the articular cartilage. The anchors were loaded onto a PEEK PushLock Anchor (Arthrex). The anchors were then pushed into each bone socket, and the suture ends were pulled through until there was adequate tension on the apposition of labral tissue to bone. One to 5 anchors were used for both SLAP and Bankart procedures depending on the size of the labral tear. 19
Postoperative Rehabilitation Protocol
All patients who underwent labral repair underwent a standardized rehabilitation protocol postoperatively. In the first phase, patients were instructed to wear a sling for 6 weeks after their surgery and began scapular strengthening and pendulum arm exercises from the first day after surgery. Patients were permitted to passively flex their shoulder by 2 weeks postoperatively. By 6 weeks after surgery, patients were evaluated by a physical therapist, and the second phase of the rehabilitation program was initiated from 6 weeks to 18 weeks after surgery. This phase included a combination of isometric strengthening exercises and actively supported external rotation movements. At 18 weeks after surgery, patients were evaluated again by a physical therapist, and the third phase of rehabilitation was initiated up to 6 months postoperatively. This phase involved the use of a stretchable latex band to perform internal and external rotation, shoulder extension, straight-arm lifts, adduction, and rowing movements.
Statistical Analysis
The prevalence of shoulder pain and hand paresthesia was measured by comparing the proportion of patients who responded “none” to that of patients who responded at least “slight” on the questionnaire. This proportion was reported as a percentage. The chi-square test was used to compare the prevalence of shoulder pain and hand paresthesia between the Bankart and SLAP groups at each time point. The magnitude of shoulder pain and hand paresthesia was measured on a 5-point Likert scale (0 = none, 1 = slight, 2 = medium, 3 = severe, 4 = very serious) and was reported as mean ± SEM. Overall scores among symptomatic patients in the Bankart and SLAP groups at each time point were compared using the Mann-Whitney test. The Kruskal-Wallis test was used to compare the prevalence and magnitude of the measured outcomes within each group across all time points.
To determine the factors associated with hand paresthesia, we conducted bivariate correlation analysis to compare variables from before surgery and at 6 months postoperatively in the Bankart and SLAP groups. The Spearman correlation coefficient (r) was used to determine the relationship between the variables taken from the preoperative and postoperative data (alpha level = 0.05).
Results
Study Group
A total of 89 arthroscopic labral repair surgeries were performed by a single surgeon during the study period (August 2018-February 2021). Of these, 11 were excluded for being revision surgeries, and 4 patients were excluded for not answering the preoperative questions. Eight patients were excluded for undergoing a concomitant Bankart and SLAP repair. This resulted in 66 patients who underwent arthroscopic labral repair and formed the study cohort (Figure 1). Of these, 47 underwent isolated Bankart repair, and 19 underwent isolated SLAP repair.

Patient selection flowchart. SLAP, superior labral anterior-posterior.
Study Characteristics
The characteristics of the study groups are outlined in Table 1. Patients in the SLAP group were older (P < .05) and reported a lower rate of shoulder dislocations before their evaluation (P < .001) and more work-related injuries (P < .05) compared with the Bankart group. No other significant differences were recorded with respect to patient sex, time from symptom onset to surgery, side of affected shoulder, and if the patient’s evaluation was related to a specific injury.
Study Cohort Characteristics a
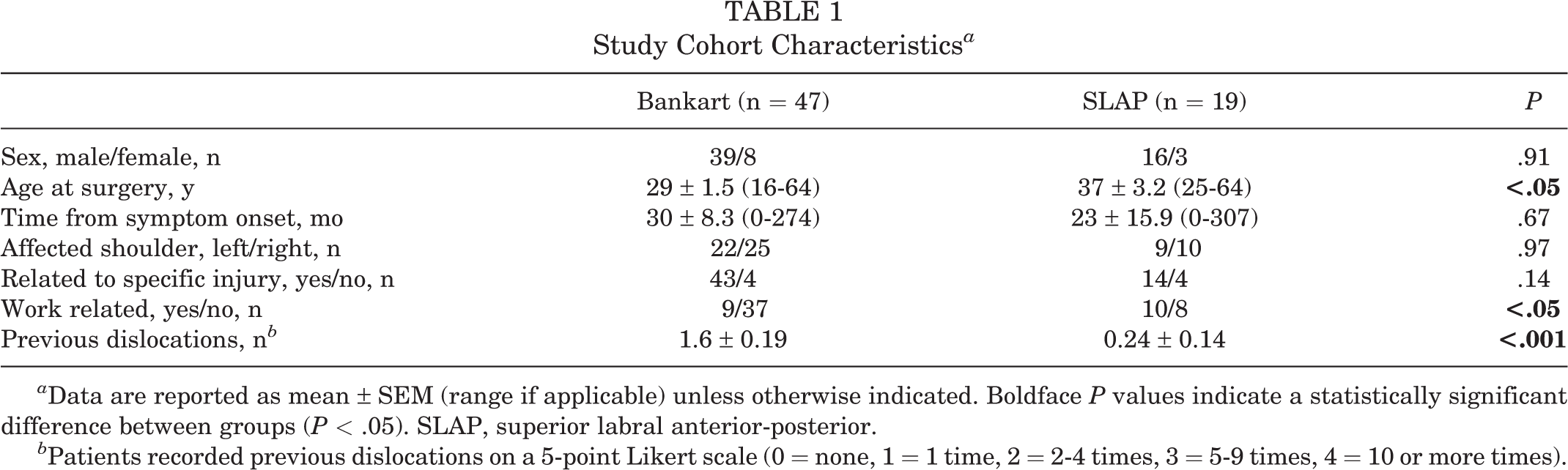
a Data are reported as mean ± SEM (range if applicable) unless otherwise indicated. Boldface P values indicate a statistically significant difference between groups (P < .05). SLAP, superior labral anterior-posterior.
b Patients recorded previous dislocations on a 5-point Likert scale (0 = none, 1 = 1 time, 2 = 2-4 times, 3 = 5-9 times, 4 = 10 or more times).
Operative Details
The operative data of the study groups are summarized in Table 2. A larger average number of anchors were used in the Bankart group compared with the SLAP group (P < .01). There was no difference in operative time between the SLAP and Bankart groups.
Study Cohort Operative Data a
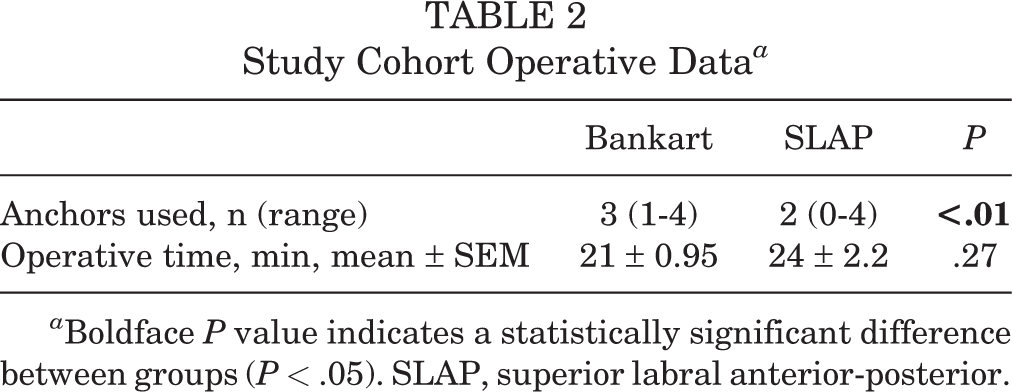
a Boldface P value indicates a statistically significant difference between groups (P < .05). SLAP, superior labral anterior-posterior.
Bankart Versus SLAP Repair: Temporal Outcomes
Prevalence of Shoulder Pain and Hand Paresthesia
Figures 2 and 3 show the percentage of patients who reported shoulder pain and hand paresthesia as at least 'slight.' Patients in the SLAP group reported a higher prevalence of shoulder pain during rest, overhead activities, and sleep compared with those in the Bankart group (Figure 2). Patients in the Bankart group reported reductions in the prevalence of their shoulder pain compared with preoperative levels by 6 months after surgery. There was no between-group difference in the prevalence of hand tingling or numbness at any time point (Figure 3). Patients in the Bankart group reported a reduction in the prevalence of numbness from 40% to 15% by 1 week after surgery (P < .05).

Temporal outcomes in the prevalence of shoulder pain during (A) rest, (B) overhead activities, and (C) sleep between the Bankart and superior labral anterior-posterior (SLAP) groups. Significant difference between groups: † P < .05; †† P < .01; †††† P < .0001. Significant within-group difference across time: *P < .05; **P < .01. Pre-op, pre-operatively.

Temporal outcomes in the prevalence of (A) hand tingling and (B) hand numbness between the Bankart and superior labral anterior-posterior (SLAP) groups. Significant within-group difference across time: *P < .05. Pre-op, pre-operatively.
Magnitude of Shoulder Pain and Hand Paresthesia
Figures 4 and 5 show the magnitude of shoulder pain and hand paresthesia (0 = none, 1 = slight, 2 = medium, 3 = severe, 4 = very serious). Regarding the shoulder, no patients reported pain as “very serious” during rest, overhead activities, or sleep at any time point. Patients in the SLAP group reported worse preoperative shoulder pain during sleep compared with those in the Bankart group (2.2 ± 0.22 vs 1.6 ± 0.18, respectively; P < .05). Postoperatively, patients in the SLAP group reported worse shoulder pain during rest, with overhead activities, and during sleep at 6 weeks, 12 weeks, and 6 months after surgery (P < .05 vs Bankart group for all). Only patients in the Bankart group reported reductions in the severity of their shoulder pain during rest, with overhead activities, and during sleep from preoperatively to 6 months postoperatively (P < .05 for all) (Figure 4).

Temporal outcomes in the magnitude of shoulder pain during (A) rest, (B) overhead activities, and (C) sleep between the Bankart and superior labral anterior-posterior (SLAP) groups. Significant difference between groups: † P < .05; †† P < .01; ††† P < .001; †††† P < .0001. Significant within-group difference across time: *P < .05; **P < .01; *** P < .001 ****P < .0001. Pre-op, pre-operatively.

Temporal outcomes in the magnitude of (A) hand tingling and (B) hand numbness between the Bankart and superior labral anterior-posterior (SLAP) groups. Significant within-group difference across time: *P < .05. Pre-op, pre-operatively.
Regarding hand paresthesia, no patients reported an average severity worse than “slight” in either group at any time point. There were no significant differences in the severity of hand tingling or numbness between the SLAP and Bankart groups. Only patients who underwent Bankart repair had a significant reduction in the severity of their preoperative hand numbness, at 1 week postoperatively, from 0.7 ± 0.14 to 0.2 ± 0.08 (P < .05).
Factors Associated With Hand Paresthesia
Table 3 summarizes the preoperative factors significantly associated with hand tingling and hand numbness, and Table 4 summarizes the 6-month postoperative factors. In the Bankart group, both preoperative hand numbness and tingling were positively associated with the preoperative frequency of shoulder pain during activity and the level of resting and overhead shoulder pain and shoulder stiffness and were negatively associated with ROM in abduction, external rotation, and internal rotation. Only patient age was negatively associated with preoperative tingling in the SLAP group, and the preoperative level of sleep pain was positively associated with numbness. At 6 months postoperatively, tingling was positively associated with age in the Bankart group, although it was negatively associated with age in the SLAP group.
Correlation Coefficients for Significant Factors Associated With Preoperative Hand Tingling and Numbness in Patients Who Underwent Bankart and SLAP Repairs a

aP < .05 for all values. Dashes indicate nonsignificant associations. ROM, range of motion; SLAP, superior labral anterior-posterior.
Correlation Coefficients for Significant Factors Associated With 6-Month Postoperative Hand Tingling and Numbness in Patients Who Underwent Bankart and SLAP Repairs a
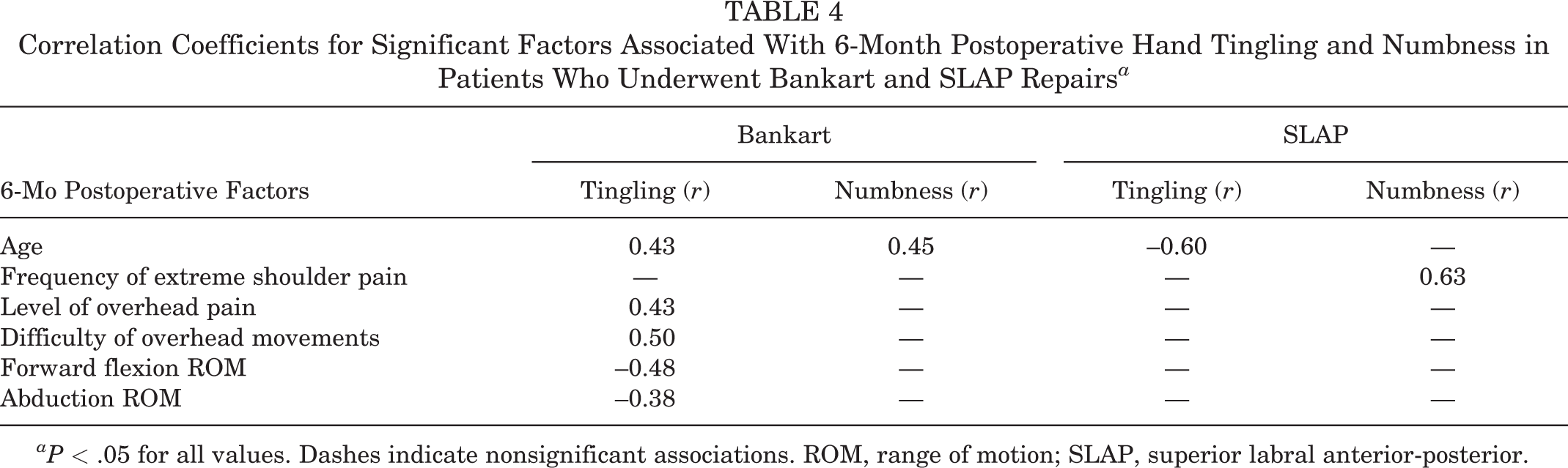
aP < .05 for all values. Dashes indicate nonsignificant associations. ROM, range of motion; SLAP, superior labral anterior-posterior.
Discussion
This study showed that patients who underwent superior labral (SLAP) repairs had a higher prevalence of shoulder pain compared with those who underwent anteroinferior labral (Bankart) repairs before and after surgery. Patients who underwent SLAP repairs also reported more severe shoulder pain before surgery compared with those who underwent Bankart repairs. The latter patients reported more favorable outcomes after surgery with respect to the prevalence and magnitude of their shoulder pain. We also found that a significant proportion of patients who underwent labral repairs reported symptoms of hand numbness and tingling. Patients who underwent Bankart repairs reported reductions in the prevalence (from 40% to 15%; P < .05) and magnitude (from 0.7 ± 0.14 to 0.2 ± 0.08; P < .05) of hand numbness from preoperatively to 1 week postoperatively.
Both pre- and postoperatively, patients who underwent SLAP repairs reported a higher prevalence of shoulder pain during sleep and rest compared with those who had Bankart repairs. After surgery, patients who had SLAP repairs also experienced a larger proportion of and more severe shoulder pain during rest, sleep, and overhead activities. To our knowledge, there is only 1 study that has compared shoulder pain pre- and postsurgery between patients who underwent SLAP and Bankart repairs. Our findings were consistent with the study by Murphy et al, 20 who illustrated that patients who had SLAP repairs experienced more pain at night and during overhead activities than those who had isolated Bankart or concomitant Bankart and SLAP repair. They also found that patients with SLAP tears have more shoulder stiffness and less satisfaction after surgery compared with those with isolated Bankart or concomitant SLAP and Bankart tears. These findings are further supported by Kim et al, 12 who found no significant differences between patients with isolated Bankart, concomitant Bankart and SLAP, and circumferential labral lesions with respect to postoperative clinical shoulder outcomes, suggesting that the size of the labral lesion does not influence patient outcomes after surgery. Instead, the findings of our study have led us to hypothesize that the location of labral tear may influence shoulder pain before and after surgery.
Alternatively, the results of this study may be related to the difference in symptom presentation between SLAP and Bankart lesions. Patients with SLAP tears are most commonly evaluated with nonspecific shoulder pain, although other symptoms include weakness, popping, and less frequently instability. 6 In contrast, the chief complaint in patients with Bankart lesions is recurrent shoulder instability, while shoulder pain and mechanical symptoms including clunking and locking are also commonly reported in labral injuries. 18 This may suggest that patients with SLAP tears are evaluated mostly because of their shoulder pain, which is more persistent and severe both before and after surgery. Accordingly, the effectiveness of arthroscopic SLAP repair in improving pain and shoulder function is contentious and has been well documented in the literature. Li et al 16 found that both SLAP repairs and biceps tenodesis were effective in improving shoulder pain and function after SLAP tear, although biceps tenodesis was more effective at improving patient satisfaction and return to sports. Therefore, the benefit of biceps tenodesis in improving shoulder pain and its relationship with paresthesia of the upper limb may be an area of future investigation.
This study also confirmed our anecdotal observation that a large proportion of patients evaluated for labral repair had hand numbness and tingling in addition to their shoulder pain. Of the patients who reported hand numbness, only those who underwent Bankart repair reported significant improvement from preoperatively to 1 week postoperatively. To our knowledge, this is the first study to show a potential association of SLAP and Bankart tears with numbness and tingling of the hand. Hand paresthesia in patients with shoulder pathologies has previously been reported. Sivan et al 29 reported a high prevalence (54%) of hand paresthesia in patients undergoing subacromial decompression surgery. Also, Xu et al 34 obtained arthroscopic biopsies of the shoulder capsule in patients undergoing capsular release. The samples from frozen shoulders revealed increased expression of nerve growth factor receptors, neoinnvervation, neoangiongenesis, subsynovial hypercellularity, and fibroplastic proliferation compared with controls. Tham et al 31 also showed increased glenohumeral capsular thickness on ultrasound after rotator cuff repair. We also have recently reported that early capsulitis is associated with better 2-year outcomes after SLAP repair. 21 These results suggest that early shoulder pain and stiffness is associated with labral healing and better outcomes with respect to shoulder pain, difficulty of movement, and stiffness by 2 years after surgery. Additionally, Gwilym et al 10 reported that a large proportion of patients awaiting subacromial decompression experienced referred pain radiating down the arm and showed hyperalgesia to punctate stimulus of the skin compared with controls, and these patients reported poorer functional outcomes by 3 months after surgery. This study by Gwilym et al provides evidence of central pain sensitization after shoulder injury, which describes features of neuropathic pain including paresthesia occurring because of alterations in excitatory and inhibitory central noxious pathways, which can occur in patients with labral injuries. 26 Therefore, we hypothesize that a healing process involving new nerve formation in the glenohumeral joint capsule may occur after injury, and this may contribute to the manifestation of peripheral upper limb paresthesia because of interactions with the central nociceptive pathways. Although this study did not investigate this hypothesis, future studies may delve into the physiology and symptomology of nociception after shoulder injuries and surgery.
Interestingly, we unexpectedly found that the levels of hand tingling in patients who underwent SLAP repairs both preoperatively (r = –0.57) and at 6 months postoperatively (r = –0.60) were negatively associated with patient age at surgery. In contrast, there was a positive association between patient age at surgery and hand tingling and numbness in the Bankart group 6 months after surgery (r = 0.43 and 0.45, respectively). These results suggest that younger patients with SLAP tears report higher levels of hand tingling both before and after surgery compared with older patients reporting higher levels of hand numbness and tingling by 6 months after surgery. This may be related to the origin of SLAP tears, in which younger patients are more likely to sustain traumatic SLAP lesions, compared with degenerative SLAP injuries, 33 which may affect the level of hand paresthesia symptoms. Before surgery and 6 months postoperatively, respectively, hand tingling was positively associated with the level of shoulder pain (r = 0.44 and 0.43) and difficulty during overhead activities (r = 0.30 and 0.50) and negatively associated with abduction ROM (r = –0.35 and –0.38). These results may further suggest that movements that aggravate the superior aspect of the shoulder joint, such as during abduction and overhead movements, may further precipitate distal upper limb paresthesia.
The strengths of this study were the prospective nature of data collection and the clear inclusion and exclusion criteria of hand numbness and tingling among an adequate sample size. Furthermore, rather than simple yes/no dichotomous questions, the data were collected using a scale, which allows more accurate patient reporting. The study also has high internal validity, with all shoulder pathologies being diagnosed and repaired by the same shoulder surgeon using the same devices, with extensive experience in shoulder surgery at a single campus. However, these factors (same surgeon, same campus) may limit the applicability of the findings to other surgeons and centers.
There were several potential limitations of this study that should be considered. We did not formally perform nerve conduction studies or magnetic resonance imaging to rule out cervical radiculopathy, carpal tunnel syndrome, and cubital tunnel syndrome, which are known causes of hand paresthesia. 2 However, Koulidis et al 14 recently performed a systematic review evaluating the diagnostic accuracy of neurodynamic tests for the assessment of neuropathic pain. They found that nerve conduction studies alone were not useful in the diagnosis of upper limb neuropathies, including carpal tunnel syndrome and cervical radiculopathy. We did not record the dermatomal distribution of patients’ hand numbness and tingling and did not clinically assess for signs of carpal tunnel syndrome. The study was also limited to a 6-month follow-up, which may not have been a long enough time frame to fully observe the temporal outcomes of hand paresthesia. Also, patients in the SLAP group were older at the time of surgery and reported more work-related injuries compared with those in the Bankart group, which may have contributed to worse outcomes.
Conclusion
This study has shown that the location of the labral lesion may have an effect on the outcomes of shoulder pain before and after surgery. Patients who underwent SLAP repairs reported a higher prevalence of and more severe shoulder pain up to 6 months after surgery. Patients who underwent Bankart repairs also reported improvements in their hand numbness at 1 week after surgery.
Footnotes
Final revision submitted March 17, 2022; accepted March 31, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.A.C.M. has received research support and consulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the South-Eastern Sydney Local Health District Human Research Ethics Committee (reference No. HREC/11/STG/37).