
Abstract
Background:
Arthroscopic repair of combined Bankart/superior labral anteroposterior (SLAP) lesions is commonly performed to treat anterior shoulder instability, the clinical outcomes of which have not been widely studied.
Purpose:
To compare the clinical outcomes for arthroscopic repair of combined Bankart/SLAP lesions in the treatment of anterior shoulder instability and to ascertain whether it is inferior to isolated Bankart repair.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A systematic review of the literature was performed through use of the MEDLINE, EMBASE, and Cochrane Library databases according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Study bias was assessed using the MINORS (Methodological Index for Non-Randomized Studies) scoring system. Randomized controlled trials, prospective or retrospective cohort studies, and case-control studies were included, whereas systematic reviews, literature reviews, conference abstracts, case reports, case series, and non-peer-reviewed studies were excluded to guarantee the quality of the study. Data on outcomes including recurrence rate, functional scores, and range of motion (ROM) were pooled, with statistical analysis performed. A P value of <.05 was considered statistically significant.
Results:
The review included 7 studies with a total of 520 patients. The pooled recurrence rate after combined Bankart/SLAP repair was 6.47% (9/139). Significant improvements of postoperative versus preoperative functional scores were observed, including a reduction in the visual analog scale score for pain (mean ± SD: 0.99 ± 1.36 vs 4.13 ± 2.26; P < .00001) and an increase in mean Rowe score (89.56 ± 11.46 vs 43.16 ± 8.87; P < .00001) and mean Constant score (91.41 ± 7.57 vs 59.70 ± 5.63; P < .00001). In terms of ROM, no reduction was found in external rotation (66.56° ± 13.33° vs 67.22° ± 14.27°; P = .21), and a significant increase in abduction was found (157.67° ± 4.11° vs 144.18° ± 8.28°; P < .00001). No statistically significant difference was found between arthroscopic repair of combined Bankart/SLAP lesions and isolated Bankart repair regarding recurrence rate, functional scores, or ROM.
Conclusion:
Of the pooled data, patients who underwent arthroscopic repair of combined Bankart/SLAP lesions in treatment of anterior shoulder instability showed a low recurrence rate, favorable functional scores, and no significant restriction on ROM, all of which were not significantly worse than outcomes of isolated Bankart repair. Therefore, combined repair was proven to be a viable option for extensive labral lesions.
Combined Bankart/superior labral anteroposterior (SLAP) lesions, which are increasingly reported during arthroscopic surgeries in treatment of anterior shoulder instability, are defined as glenoid labral tears from anteroinferior to superior, regardless of whether there is continuity. 27 In most cases, they can simply be considered Bankart lesions with concomitant SLAP injuries. According to previous studies, 8,19,59 approximately 20% to 57% of patients with anterior shoulder instability have combined Bankart/SLAP lesions. 15,16 Although Bankart lesions are a primary pathological feature in posttraumatic anterior shoulder instability, 18 SLAP tears can also impair shoulder stability by damaging the superior labrum and the biceps tendon, both of which play an essential role in maintenance of proper glenohumeral joint functions. 11,54,57,58 Therefore, the treatment for combined Bankart/SLAP lesions to maintain shoulder stability also draws surgeons’ attention. In current clinical practice, surgical fixation of both Bankart lesion and concomitant SLAP lesion to stabilize the shoulder joint in cases of anterior shoulder stability is advocated by most authors. 8,23,27,33,34,40,45,56
Several studies 10,14,34,51,54,56 have reported that arthroscopic repair of combined Bankart/SLAP lesions produced satisfactory postoperative outcomes including a low recurrence rate, pain alleviation, and shoulder function improvement. Furthermore, among young and active patients, the combined repair promotes early return to sports, especially overhead sports. 25,43 However, compared with isolated Bankart lesions, combined Bankart/SLAP lesions present a larger range of labral injuries, which adds difficulty to the surgical repair process with potential visual limitations and extra procedures such as a suspension sling to hang the superior labrum during the surgery. Other complications can include loss of range of motion (ROM), delayed recovery of ROM, shoulder stiffness, and low rate of return to sports. 5,7,19,21,26,29,56
The overall effect of the combined repair on clinical outcomes has not been widely studied, although some controversies still exist. Many studies ‡ found no statistically significant difference between combined arthroscopic Bankart/SLAP repair and isolated arthroscopic Bankart repair through assessment of postoperative shoulder function. Nevertheless, several studies 10,19,32,36,50,56 noted that arthroscopic repair of combined Bankart/SLAP lesions might result in limitation of shoulder ROM because the repair of more extensive labral lesions from the anteroinferior to superior portion of the glenoid requires more anchors and sutures for fixation, which could cause excessive tension to surrounding soft tissues, leading to excessive tension and stiffness. 29,37,56 Additionally, a delayed recovery after surgery was observed, which could result from a slower healing rate of extensive combined lesions. 10,14 Since these results are based on relatively limited sample sizes, more robust evidence is needed to determine the actual outcomes for arthroscopic repair of combined Bankart/SLAP lesions.
Currently, no systematic review exists of studies evaluating clinical outcomes for arthroscopic repair of combined Bankart/SLAP lesions or the comparison between combined and isolated procedures. Therefore, the goal of this systematic review and meta-analysis was to evaluate clinical outcomes for arthroscopic repair of combined Bankart/SLAP lesions and to ascertain whether combined repair was inferior to isolated Bankart repair. It was hypothesized that the included studies would demonstrate favorable clinical outcomes after combined repair as well as postoperative outcomes that were no worse than after isolated Bankart repair.
Methods
Search Strategy
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were used to perform a systematic review of all available literature. A literature search was performed of the MEDLINE, EMBASE, and Cochrane Library databases in February 2019, with the following search algorithm: ((Bankart lesion OR Bankart tear OR anteroinferior labrum lesion) AND (Superior Labrum from Anterior to Posterior Injury OR SLAP injury OR SLAP tear) OR SLAP V lesion OR type V SLAP lesion) AND (arthroscopic repair OR combined repair) AND (shoulder dislocation OR glenohumeral dislocation OR shoulder instability). No filter was used during the database search, in order to increase sensitivity. All search results were examined for relevance after removal of duplicates. The titles and abstracts were reviewed and screened first. Then, potentially eligible studies received a full-text review. Moreover, bibliographies of relevant studies were manually screened for possible additional studies meeting the inclusion criteria.
Eligibility Criteria
To be included in the systematic review, the studies had to (1) include patients with combined Bankart/SLAP lesions and isolated Bankart lesions, both of which underwent arthroscopic surgeries; (2) compare arthroscopic repair of combined Bankart/SLAP lesions with arthroscopic repair of isolated Bankart lesions; (3) evaluate clinical outcomes; (4) be a randomized controlled trial, prospective or retrospective cohort study, or a case-control study; and (5) be written in English. Exclusion criteria were as follows: (1) studies that did not quantify clinical outcomes; (2) systematic reviews, literature reviews, conference abstracts, case reports, case series, and non–peer reviewed studies; and (3) animal or cadaveric studies.
Quality Evaluation
No randomized trials were found during the literature search; therefore, 2 reviewers (S.F. and Y.S.) independently assessed the risk of bias for every included study using the MINORS (Methodological Index for Non-Randomized Studies) scale, which was specially developed and validated to evaluate and determine the quality of nonrandomized studies. 48 The results could give an indication of potential sources of bias among included studies. Disagreements were resolved through discussion. A total of 12 items were included, and the last 4 items were specific for comparative studies. Each item included in the MINORS scale was scored as follows: 0 for not reported; 1 for reported but poorly or inadequately conducted; 2 for reported sufficiently and conducted adequately. A noncomparative study had a maximum possible score of 16, whereas a comparative study had a maximum possible score of 24.
Data Extraction and Analysis
Studies that met the inclusion criteria were evaluated, and relevant data were extracted by the 2 reviewers independently before reaching a consensus. The following data were extracted: study characteristics (study design, level of evidence [LOE], number of participants), mean follow-up period, sample size, patient characteristics (mean age at the time of surgery, sex, dominant arm involvement), and clinical outcomes (recurrence rate, functional scores, ROM). We focused on outcomes that measured (1) recurrence rate, including all incidences of recurrent dislocations, subluxations, and revisions due to recurrence after arthroscopic repair; (2) functional scores, mainly assessing visual analog scale for pain (VAS), Rowe, and Constant scores; and (3) ROM, mainly measuring external rotation with arm at side and abduction.
Statistical Analysis
All statistical analyses were performed by use of Review Manager (version 5.3; Nordic Cochrane Centre, The Cochrane Collaboration). Heterogeneity across studies was quantified using the I 2 statistic. 20 An I 2 value of less than 25% was used to represent low heterogeneity and an I 2 value of greater than 75% indicated high heterogeneity. Random effects models were used when the I 2 value was greater than 50% or when subgroup analysis was conducted; otherwise, fixed-effects models were adopted. When the range was given instead of a standard deviation in the studies included, the methods of Wan et al 55 were used to estimate the standard deviation. Results are presented as risk ratio (RR) for dichotomous outcomes and mean difference (MD) with 95% CI for continuous outcomes. However, considering that different measurement units and definitions were included in scoring scales, all of the included functional scores are presented as standard mean difference (SMD). P < .05 was regarded as statistically significant.
Results
Study Identification
The search strategy and the results used in this systematic review and meta-analysis are shown in Figure 1. The initial literature search resulted in 809 studies. After removal of duplicates, the remaining 752 articles were screened for inclusion and exclusion criteria by reviewing titles and abstracts. Then, 51 full-text articles were assessed for eligibility. In only 7 of 51 studies with potential eligibility were clinical outcomes adequately quantified. These 7 studies, 3,10,14,17,19,25,60 consisting of 520 patients, were included in the final analysis.
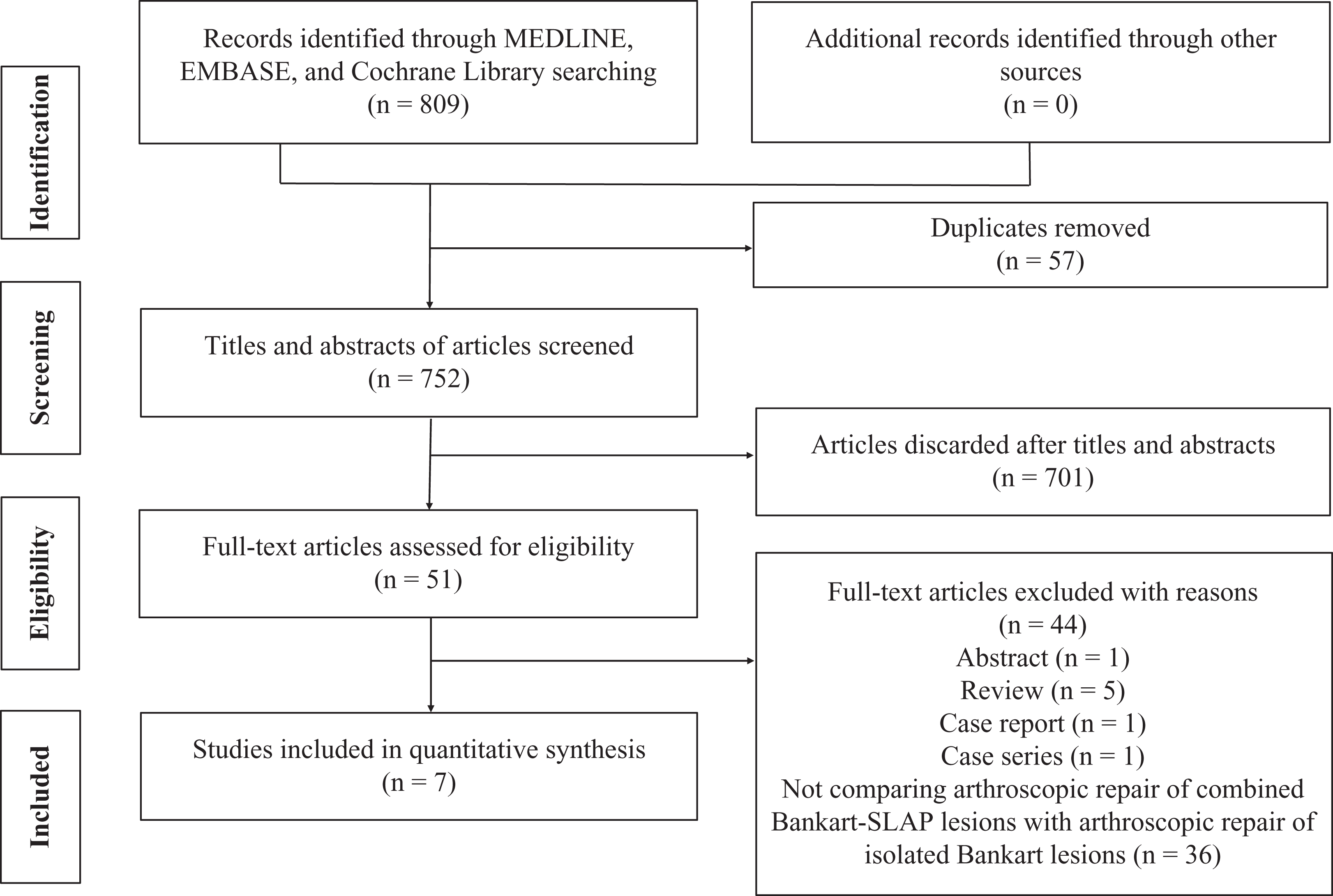
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Study and Patient Characteristics
Of the 7 studies included in this systematic review, 3 were prospective cohort studies (LOE 2) and 4 were retrospective cohort studies (LOE 3) (Table 1). All studies had a MINORS score of 18 or higher. The mean follow-up period was 29.5 months (range, 12-92 months). In total, 520 patients (85.2% males) with a mean age of 25.6 years (range, 15-69 years) were included initially, and 473 completed the follow-up. There were 177 patients (mean age, 26.2 years) treated with arthroscopic repair of combined Bankart/SLAP lesions compared with 343 patients (mean age, 24.9 years) treated with arthroscopic repair of isolated Bankart lesions (Table 2). The baseline age, sex distribution, and other reported variables were similar between the cohorts across the studies included (P > .05).
Study Characteristics a
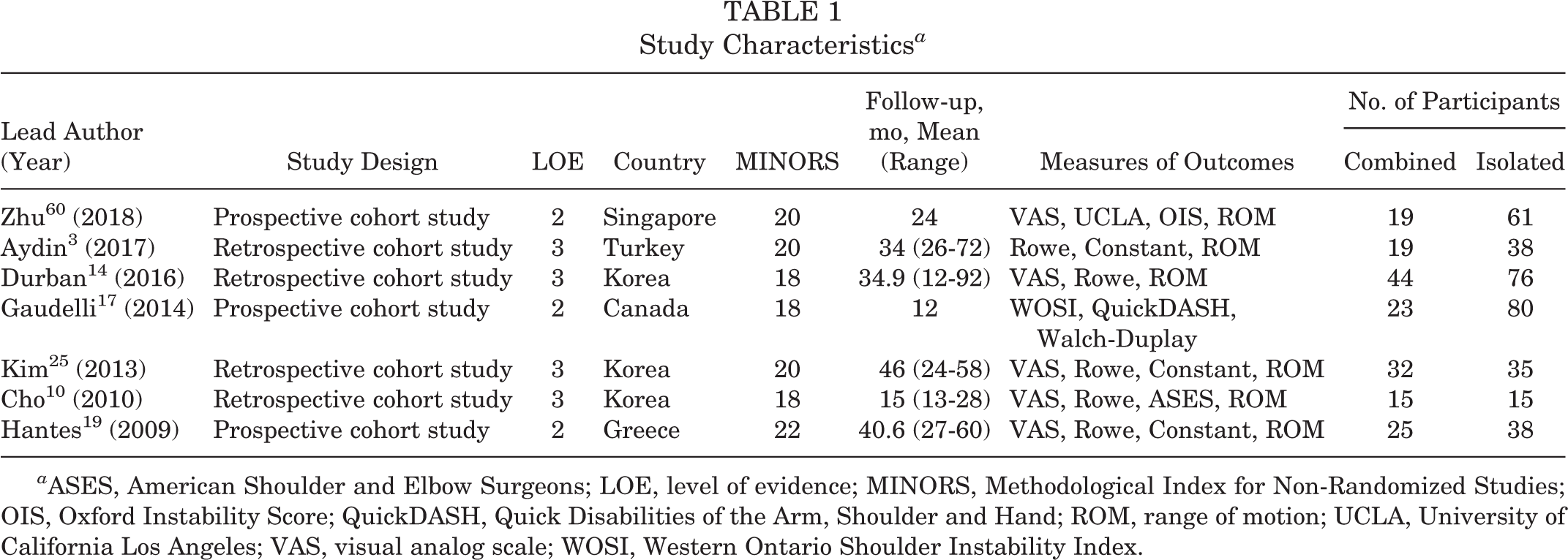
a ASES, American Shoulder and Elbow Surgeons; LOE, level of evidence; MINORS, Methodological Index for Non-Randomized Studies; OIS, Oxford Instability Score; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; ROM, range of motion; UCLA, University of California Los Angeles; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
Participant Characteristics a

a Com, combined Bankart/SLAP lesions; Iso, isolated Bankart lesions; M/F, male/female; NA, not applicable; SLAP, superior labral anteroposterior.
b Values are expressed as mean (range) or mean ± SD.
Clinical Outcomes
The data for pooled functional scores and ROM are summarized in Table 3, and recurrence rates for both repair types are shown in Figure 2.
Clinical Outcomes a

a Preoperative and postoperative values are expressed as mean (range) or mean ± SD. ER, external rotation; SLAP, superior labral anteroposterior; VAS, visual analog scale.
b Comparison of postoperative outcomes between combined and isolated Bankart repairs.
c Comparison of preoperative and postoperative outcomes for combined repairs.

Forest plot of comparison of recurrence rates after combined Bankart/superior labral anteroposterior (SLAP) repair versus isolated Bankart.
Recurrence rates were measured in all 7 studies. No recurrence (0%) was reported in 2 of the included studies, which couldn’t be pooled due to the rule of Review Manager 5.3. After the recurrence rates from 5 studies were pooled, 3,14,19,25,60 combined Bankart/SLAP repair resulted in a recurrence rate of 6.47% (9/139), whereas isolated repair had a recurrence rate of 5.24% (13/248). No statistically significant difference was found between the 2 repairs (RR, 1.46; 95% CI, 0.63 to 3.38; I 2 = 0%; P = .38) (Figure 2).
The VAS score was reported in 5 studies, 10,14,19,25,60 comprising 135 combined repairs and 225 isolated repairs. The combined repair resulted in a mean VAS score of 0.94 ± 1.30, whereas the isolated repair had a mean VAS score of 0.68 ± 1.38. No statistically significant difference was detected (SMD, 0.07; 95% CI, –0.15 to 0.28; I 2 = 0%; P = .55). In 4 studies, 10,14,25,60 both preoperative (mean, 4.13 ± 2.26) and postoperative (mean, 0.99 ± 1.36) VAS scores of 110 patients with combined repair were reported. A statistically significant decrease was seen in mean VAS score after combined Bankart/SLAP repair (SMD, –1.62; 95% CI, –1.93 to –1.31; I 2 = 0%; P < .00001).
The Rowe score was reported in 5 studies, 3,10,14,19,25 comprising 135 combined repairs and 202 isolated repairs. The combined repair resulted in a mean Rowe score of 89.56 ± 11.46, compared with 91.39 ± 10.33 for the isolated repair. No statistically significant difference was detected (SMD, –0.20; 95% CI, –0.42 to 0.02; I 2 = 0%; P = .07). For the 135 patients with combined repair, both preoperative (mean, 43.16 ± 8.87) and postoperative (mean, 89.56 ± 11.46) Rowe scores were reported. A statistically significant increase was seen in mean Rowe score after combined Bankart/SLAP repair (SMD, 5.08; 95% CI, 2.97 to 7.19; I 2 = 94%; P < .00001).
The Constant score was reported in 4 studies, 3,19,25,60 comprising 95 combined repairs and 172 isolated repairs. The combined repair resulted in a mean Constant score of 91.41 ± 7.57, compared with the isolated repair of 88.67 ± 6.11. No statistically significant difference was detected (SMD, 0.64; 95% CI, –0.44 to 1.72; I 2 = 94%; P = .25). Among these studies, both preoperative (mean, 59.70 ± 5.63) and postoperative (mean, 91.41 ± 7.57) Constant scores were reported for the 95 patients with combined repair. A statistically significant increase was noted in mean Constant score after combined Bankart/SLAP repair (SMD, 3.81; 95% CI, 1.97 to 5.65; I 2 = 93%; P < .00001). Because heterogeneity was observed, a subgroup analysis stratified by mean age of the included patients was performed. In the subgroup of studies with a mean patient age younger than 24 years, the SMD of the Constant score was 2.22 (95% CI, 1.35 to 3.08; I 2 = 53%; P < .00001), whereas it was 5.43 (95% CI, 4.62 to 6.25; I 2 = 0%; P < .00001) in the subgroup of studies in which mean patient age was older than 24 years. A trend toward greater improvement regarding Constant score was suggested in patients older than 24 years, indicating that patients of a certain age group might benefit more from the combined repair than others.
The external rotation with arm at side was reported in 3 studies, 3,14,25 comprising 95 combined repairs and 149 isolated repairs. The combined repair resulted in a mean external rotation of 66.56° ± 13.33°, compared with 67.96° ± 14.97° for the isolated repair. No statistically significant difference was detected (MD, –0.01; 95% CI, –2.85 to 2.83; I 2 = 0%; P = .99). Among these studies, both preoperative external rotation (mean, 67.22° ± 14.27°) and postoperative external rotation (mean, 66.56° ± 13.33°) were reported for the 95 patients with combined repair. No statistically significant difference was seen between them (MD, –1.99; 95% CI, –5.09 to 1.11; I 2 = 0%; P = .21).
Abduction was reported in 3 studies, 3,25,60 comprising 70 combined repairs and 134 isolated repairs. The combined repair resulted in a mean abduction of 157.67° ± 4.11°, compared with 154.19° ± 4.99° for the isolated repair. No statistically significant difference was detected (MD, 1.28; 95% CI, –0.01 to 2.56; I 2 = 95%; P = .05). Among these studies, both preoperative abduction (mean, 144.18° ± 8.28°) and postoperative abduction (mean, 157.67° ± 4.11°) were reported for the 70 patients with combined repair. A statistically significant increase was noted in mean abduction after combined Bankart/SLAP repair (MD, 13.82; 95% CI, 11.67 to 15.97; I 2 = 57%; P < .00001).
Discussion
The purpose of this systematic review and meta-analysis was to ascertain the clinical outcomes for arthroscopic repair of combined Bankart/SLAP lesions in the treatment of anterior shoulder instability. Overall, combined repair yielded excellent outcomes in terms of low recurrence, significant reduction in pain, and improvements in shoulder function. Additionally, no significantly worse outcomes, specifically no significant limitation in ROM after multiple points of fixation of the labrum to the glenoid, were observed compared with isolated Bankart repair. The results verified the study hypothesis.
Generally, Bankart lesions can be found in most cases of anterior shoulder instability and are commonly treated by arthroscopic Bankart repair. 28,52 According to several biomechanical studies, 19,33,34,39,40,49 when the injury extends from anteroinferior to the superior portion of labrum (ie, there is a concomitant SLAP lesion), anterior and inferior humeral translations become more extensive, which lead to intensified anterior shoulder instability. Several biomechanical studies have observed that SLAP lesions can lead to increased glenohumeral translations, resulting in anterior shoulder instability. 33,34,39,41,42 Rodosky et al 45 reported that detachment of the superior glenoid labrum decreased the shoulder’s resistance to torsion and placed a greater magnitude of strain on the inferior glenohumeral ligament, which was detrimental to anterior shoulder stability. Moreover, SLAP lesions can disrupt the attachment of the labrum to the glenoid and the origin of the long head of the biceps tendon, both of which would increase shoulder instability. Burkart et al 6 created an artificial SLAP tear in a cadaveric model and observed an increase in anterior and anteroinferior translation. They noted that the joint translations and normal biomechanics of glenohumeral stability could partially be restored by SLAP repair.
Although some isolated SLAP lesions can be treated with nonoperative management, 38,44 combined Bankart/SLAP lesions usually require surgical treatment, which is imperative to restore shoulder stability. 13,18,54,56 Therefore, combined Bankart/SLAP repair is adopted by most surgeons to decrease joint volume and create a bumper effect on the humeral head by fixing the labrum to the glenoid rim for shoulder stabilization and prevention of residual laxity, since fixing only 1 of the 2 lesions might still result in recurrent instability. 15,19,34,40,51,54,56
In the present study, the recurrence rate in the patients who received combined Bankart/SLAP repair was 6.47% (9/139), which was low compared with isolated Bankart repair, according to existing literature. 4,53 In addition, no significant difference in recurrence rate was noted between combined Bankart/SLAP repair and isolated Bankart repair, suggesting that properly performed combined repair does not lead to a higher risk of recurrent anterior shoulder instability than isolated repair, even if the combined lesions appear to be more extensive and severe. Consistent with previous studies, 14,19,25,60 this result indicates that appropriate repair of labral lesions, however large or extensive, may be the most critical factor to avoid recurrent dislocations after arthroscopic management of anterior shoulder instability.
Numerous studies 2,9,12,30 have demonstrated excellent functional outcomes for arthroscopic Bankart repair because Bankart lesion is the most common cause of anterior shoulder instability; however, combined Bankart/SLAP repair has received much less attention due to relatively low incidence. With the pooled data in the current review, we found that VAS, Rowe, and Constant scores, which have been used more often than other functional scores in assessment of anterior shoulder instability, indicated significantly improved outcomes for combined repair. The results were in accordance with multiple studies, § in which significantly better postoperative functional scores regarding pain, daily activities, and quality of life were reported after combined repair, despite the greater severity of combined injuries and the larger extents of labral repair. Furthermore, several studies 14,25 noted that preoperative functional scores in patients with combined lesions were worse than those scores in patients with isolated lesions, but postoperative scores were not significantly different, which suggests that the combined Bankart/SLAP repair was quite beneficial to treat such serious labral lesions. Because heterogeneity was observed in the comparison between preoperative and postoperative Rowe and Constant scores, several subgroup analyses based on mean age, sex, and duration of immobilization were conducted.
Additionally, compared with isolated Bankart repair, the postoperative functional scores of the combined repair were equally good. Due to the heterogeneous nature of inclusion criteria across the included studies and the limited number of studies, heterogeneity was observed in pooled Constant score in the comparison. We had intended to perform subgroup analyses based on diverse patient variables, but such subgroup analyses were not possible due to variability in the reporting of these factors.
Concerns about limitations in shoulder ROM after multiple-point fixation of the labrum to the glenoid have been mentioned in a few studies. 10,19,32,50 Reduction in postoperative shoulder ROM was found in a variety of operative procedures; specifically, restrictions of external rotation and abduction were noted to occur most commonly after labral repair, 24,47 caused by overstress and stiffness in the glenohumeral joint. 25,29,37,56 Moreover, it has been reported that restriction in shoulder ROM is a common complication after SLAP repair. 43 In the current study, one of the most important findings was that the pooled data showed no significant reduction in either external rotation or abduction after arthroscopic repair of combined Bankart/SLAP lesions compared with isolated Bankart repair. The results are in accordance with several studies, 3,16,19,25,60 indicating that even if more extensive labral injury exists in patients with combined lesions, the combined surgical repair with more anchors used for shoulder stabilization does not necessarily lead to reduction in postoperative external rotation and abduction.
Notably, a significant increase in abduction was observed in the same follow-up period with external rotation, which suggests that the recovery of abduction is better or quicker than that of external rotation after combined repair, as a result of biomechanical parameters and rehabilitation protocols. However, there was still a slight decrease in external rotation after combined repair compared with isolated repair, which needs to be taken into consideration regarding surgical techniques. Of note, 2 studies 10,14 mentioned that although the postoperative ROM at final follow-up was similar in the 2 repair methods, significant differences were observed during the recovery process, which led to a longer recovery period among the patients who underwent combined repair. We could not verify their findings due to the limited data reported across the studies included; however, we surmise that the lengths of recovery reported probably represented a functional adaptation of the shoulder after surgery, which could be different due to various postoperative factors, not only operative factors.
This study has several limitations. First, no study that was included was randomized, and most of the data collected in this systematic review and meta-analysis were derived from retrospective studies, which could cause selective bias and recall bias. Second, few of the studies included had differentiated the outcomes among diverse populations, and the information about surgical findings was limited. Third, sample sizes in some studies were quite small and had uneven distribution over the 2 repair methods, which can cause statistical deviation.
Conclusion
According to the pooled data, patients who underwent arthroscopic repair of combined Bankart/SLAP lesions in treatment of anterior shoulder instability showed a low recurrence rate, favorable functional scores, and no significant restriction in ROM, all of which were not significantly worse than results of isolated Bankart repair. Therefore, combined repair was proven to be a viable option for extensive labral lesions.