
Abstract
Background:
Prior studies revealed the presence of superior labrum anterior-to-posterior (SLAP) injury together with Bankart lesions in some patients. The purpose of the study is to compare the clinical results of isolated Bankart repairs with the clinical results of Bankart repairs when performed with concomitant SLAP repairs.
Methods:
The patients who underwent arthroscopic surgery for treatment of anterior glenohumeral instability were evaluated retrospectively. Group 1 consisted of 19 patients who had arthroscopic SLAP repair together with Bankart repair. The mean age of the patients was 23. Group 2 consisted of 38 patients who underwent isolated Bankart repair. The mean age was 24. Knotless anchors were used in both groups.
Results:
The mean follow-up was 34 months (range: 26–72). In group 1, the mean preoperative Constant score was 84 (range: 74–90, standard deviation (SD): 5.91) and Rowe score was 64.1 (range: 40–70, SD: 8.14). In group 2, the preoperative Constant score was 84.4 (range: 70–96, SD: 5.88) and Rowe score was 60 (range: 45–70, SD: 7.95). In group 1, the postoperative mean Constant score raised to 96.8 (range: 88–100, SD: 2.91) and the mean Rowe score raised to 92.3 (range: 85–100, SD: 5.17). In group 2, the postoperative mean Constant score was 94.9 (range: 88–100, SD: 3.70) and the mean Rowe score was 94.2 (range: 80–100, SD: 4.71). The difference between the scores of two groups was insignificant (p > 0.05). When the numbers of redislocations and range of motion were compared, no significant difference was found (p > 0.05).
Conclusion:
Accompanying SLAP repair in surgical treatment with Bankart repair for shoulder instability does not affect the results negatively. Properly repaired labral tears extending from anterior inferior to the posterior superior of the glenoid in instability treatment have the same outcome in overall results as repaired isolated Bankart lesions.
The Bankart lesion was described as the detachment of the inferior glenohumeral ligament in the labrum from the anterior glenoid as a result of anterior shoulder instability. 1 The inferior glenohumeral ligament complex, labrum, and bony anatomy are the main stabilizers of the shoulder joint. Lack of healing of the labrum results in recurrent anterior dislocations of the shoulder joints. 1–4 In addition to classical Bankart lesions, different labrum injuries can be seen in these patients. These are anterior labroligamentous periosteal sleeve avulsion lesions, superior labrum anterior-to-posterior (SLAP) lesions, a triple labral (anterior, posterior, and superior) lesion, or glenoid rim fractures. 3,5 SLAP lesions are labral tears involving the biceps tendon. Common symptoms of SLAP lesions include pain, catching sensations, and locking. Itoi et al. showed that the long head of the biceps tendon has a stabilizing function when the arm is in abduction and in external rotation. 6 When Andrews et al. first defined the lesion, they proposed that the reason for the tear was increased tension during throwing. 2 Later, Snyder et al. reported the compression of the shoulder joint as a common cause of SLAP lesions. 7 Although SLAP lesions can occur as isolated injuries, they can also be accompanied by Bankart lesions in anterior shoulder instability. 2,3 SLAP lesions may also play a role in etiology of anterior instability. 8 Snyder et al. classified SLAP lesions into four types, from simple degenerative frying to buckle handle tears. 2,7 Maffet et al. later classified SLAP lesions into seven types with three more variations. 9
Maffet et al. described a type V lesion as a combined Bankart and SLAP lesions (Figure 1). In this injury, the anteroinferior lesion of the labrum is concomitant with a Snyder’s type II SLAP lesion, which is commonly seen in instability patients. 7,9 The severity of labrum lesions increases with the number of dislocations. The coincidence rate of this combined lesion in different series was reported between 20% and 57%. 1,3,10,11 Gartsman et al. reported an increased incidence of combined Bankart and type II SLAP lesions in patients with chronic anterior instability. 12 The repair of the entire labrum tear from the anteroinferior to the superior edge of the glenoid is recommended in type V lesions. 3 The fixation of these lesions requires more anchors or sutures for fixation, which may result in over-tightening of the soft tissues. Therefore, a limitation of postoperative range of motion or symptomatic SLAP repair might be detected. We hypothesized that a higher frequency of symptomatic biceps tendon and/or shoulder re-dislocation in addition to increased deficits in postoperative range of motion in combined repairs with respect to isolated Bankart repairs would be observed. Concordantly, the clinical outcomes of patients with anterior shoulder instability were retrospectively evaluated.

Illustration of SLAP type V lesion. (α) Anterior labrum, (β) long head of biceps tendon, and (γ) glenoid. SLAP: superior labrum anterior-to-posterior.
Patients and methods
The Human Research Studies Ethics Committee approved this retrospective study. Sixty-nine patients were operated arthroscopically for anterior shoulder instability between November 2008 and April 2013. Prospective collected data of the patients were reviewed retrospectively. The patients operated for isolated Bankart or combined Bankart and SLAP repair were included in this study. The inclusion criteria were as follows: (1) a preoperative history of traumatic anterior shoulder instability; (2) Magnetic Resonance Imaging (MRI) findings of Bankart lesions; (3) more than one episode of anterior shoulder dislocation; (4) a positive apprehension test at the initial examination; (5) age below 35 at surgery; (6) loss of substance of humeral head not exceeding 30%, as documented by MRI; and (7) the absence of glenoid fractures (bony Bankart lesion). The exclusion criteria were as follows: (1) clinical evidence of multidirectional instability, (2) previous or later shoulder surgery, (3) hyperlaxity, (4) documented rotator cuff tear during arthroscopy, and (5) history of epilepsy. Twelve patients were excluded from the study because of the following conditions: partial articular-side thickness supraspinatus tear (one patient), bony Bankart lesion (six patients), age over 35 (two patients), and no response or lost to follow-up (three patients); the preoperative functional status of patients was evaluated by physical examination, Constant, and Rowe scores. The patients were examined by the first author, and a shoulder examination form was completed at the outpatient clinic. The latest follow-up physical examination consisted of a general shoulder examination, stability testing, range of motion, apprehension test, and O’Brien test. The O’Brien test was performed when the patient was sitting with the shoulder in 90° of elevation, 40° of horizontal adduction, and maximal internal rotation. The patient horizontally adducted and flexed the shoulder against the examiner’s manual resistance. The test was repeated with the patient’s arm in an externally rotated position. Pain in the internally rotated position (but not in the externally rotated position) was a positive test. 13 The apprehension test was performed when the patient was lying down. A passive external rotation of 90° of abduction with a forward pressure was applied. The pain or apprehension was noted as a positive result. 14 The patients were divided into two groups according to the intraoperative arthroscopic findings. Group 1 consisted of 19 patients (15 males and 4 females) who had arthroscopic SLAP repair together with Bankart repair (Maffet type V). The mean age of the patients was 23 (range: 16–34). Group 2 consisted of 38 patients (31 males and 7 females) who had isolated Bankart repairs. The mean age was 24 (range: 17–33).
The same surgeon operated on all the patients under general anesthesia in a beach chair position with cefazolin prophylaxis. The bony anatomy and arthroscopic portals were marked on the skin. The fluid inflow was regulated with a digital pump between 40 mmHg and 50 mmHg pressures throughout the procedure. The scope was inserted from the posterior portal, and a diagnostic arthroscopy of the joint was performed. Any intra-articular pathology was noted. Anterosuperior and anteroinferior working portals were determined with intra-articular position of a spinal needle at the rotator interval: 5.5 mm and 8 mm cannulas were used. A short distance between two portals was established particularly for easy manipulation of the sutures. With a blunt elevator and chisel, the labrum was elevated and released through the 5 to 6 o’clock position. The anterior edge of the glenoid was abraded with a shaver to gain a bleeding surface for attachment of labrum (Figure 2).
Arthroscopic view of Bankart lesion in right shoulder. (a) Anterior labral pathology. (b) Mobilization of anterior labrum. (c) Insertion of the suture shuttle. (d) At the end of the repair.
The instruments to pass the sutures were ACCU-PASS (Smith & Nephew, Memphis, Tennessee, USA) in 12 patients and SutureLasso™ (Arthrex, Naples, Florida, USA) in 44 patients: 45° suture-passing devices were used. The repair was started from the inferior point of the labrum. Highly durable Ultrabraid sutures (Smith & Nephew, Memphis, Tennessee, USA) were used in 12 patients and Fiberwire sutures (Arthrex, Naples, Florida, USA) were used in 44 patients. The sutures passed close to the outer margin of the labrum. If the margins of the labrum were faint, the capsule was grasped with deeper sutures for identification. After a simple vertical passing, the suture ends were transferred to the anterior-inferior portal. The anchor holes were drilled on the glenoid edge using the guide, and the fixation was performed by nonabsorbable polyetheretherketone (PEEK) knotless anchors in all patients. A 2.9 mm Bioraptor Knotless (Smith & Nephew, Memphis, Tennessee, USA) was used in four patients in group 1 and eight patients in group 2. The rest of the repairs were performed with a 3.5 mm PushLock Anchor (Arthrex, Naples, Florida, USA). During fixation, the shoulder was kept in a neutral position and applying excess tension was avoided to prevent a suture cut (Figure 3). Four anchors were used in group 1 and three anchors were used in group 2. The stability of the repairs was checked with an arthroscopic probe. A simple arm sling was used for the postoperative for 3 weeks. A rehabilitation protocol was started on the first day with a pendulum, active elbow, and wrist and hand Range of Motion (ROM) exercises. The rehabilitation protocol was progressed after the third week until the achievement of a fully active motion range. The rehabilitation of the patients was done in different centers, according to the patient’s preference. The external rotation was restricted for the first 2 months, and excessive external rotation (> 45°) was avoided until 6 months. The patients were evaluated by physical examination, the Constant score, the Rowe score, and the O’Brien test. Any recurrent dislocations were noted.

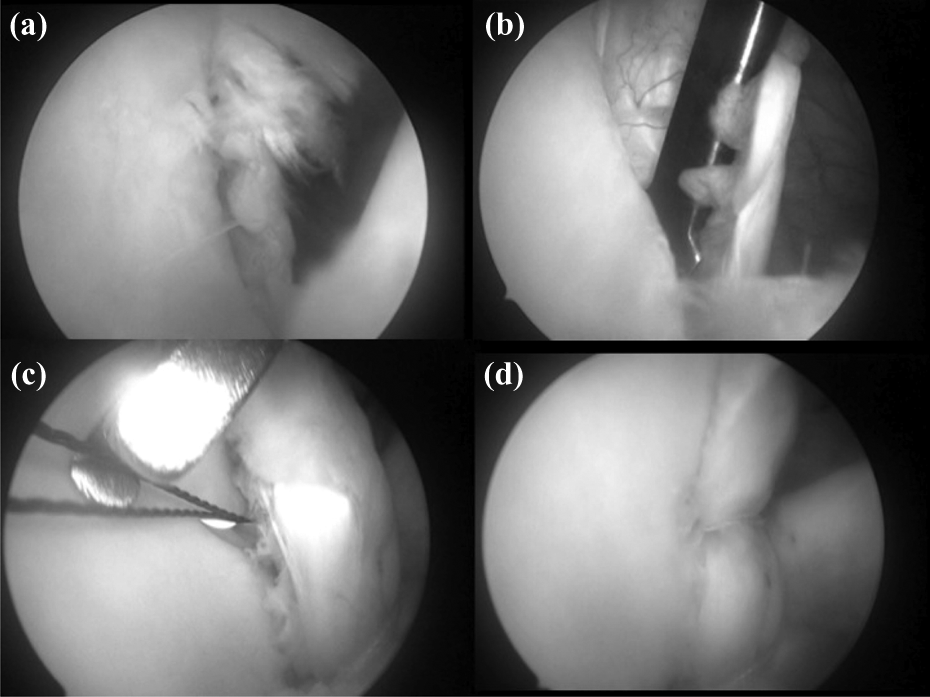
Arthroscopic view of Bankart and SLAP lesions. (a) Detachment of long head of the biceps tendon (β). (b) Preparation of the anchor insertion point for SLAP repair. (c) At the end of the repair. (d) Before the insertion of the anchor. SLAP: superior labrum anterior-to-posterior.
A paired t test was used to compare postoperative outcomes. A Fisher exact test was employed to analyze re-dislocations and special tests. The significance was set as p < 0.05.
Results
The mean follow-up period was 34 months (range: 26–72 months). There were no postoperative complications regarding infection or late adhesive capsulitis and stiffness. During follow-up, two patients in group 1 experienced re-dislocation, one at the 8th month while swimming and the other at the 18th month while wrestling. In group 2, re-dislocation occurred in three patients at the 6th, 10th, and 14th months because of motor vehicle accident, fall during sports, and heavy construction work, respectively. When the number of dislocations was compared, no statistically significant difference was found between the two groups.
In group 1, the mean preoperative Constant score was 84 (range: 74–90, standard deviation (SD): 5.91) and the Rowe score was 64.1 (range: 40–70, SD: 8.14). In group 2, the preoperative Constant score was 84.4 (range: 70–96, SD: 5.88) and the Rowe score was 60 (range: 45–70, SD: 7.95). In group 1 the postoperative mean Constant score was 96.8 (range: 88–100, SD: 2.91) and the mean postoperative Rowe score was 92.3 (range: 85–100, SD: 5.17). In group 2, the mean postoperative Constant score was 94.9 (range: 88–100, SD: 3.70) and the mean Rowe score was 94.2 (range: 80–100, SD: 4.71; Table 1). There was no statistically significant difference between the scores of two groups (p > 0.05). Preoperative mean range of motion values for group 1 was forward elevation 156.4° (range: 130–170°, SD: 13.08), abduction 158° (range: 140–170°, SD: 8.97), and external rotation 65.5° (range: 50–70°, SD: 6.09). Postoperative values were 175.2° (160–180°, SD: 4.99), 168.8° (range: 160–175°, SD: 4.70), and 61.9° (range: 50–70°, SD: 6.48), respectively. Preoperative mean range of motion values for group 2 was forward elevation 155.7° (range: 140–170°, SD: 8.67), abduction 164.2° (range: 145–170°, SD: 7.58), and external rotation 65.4 (range: 55–70°, SD: 3.90). Postoperative values were 171.2° (range: 160–180°, SD: 6.56), 170.7° (range: 160–180°, SD: 6.08), and 61.7° (range: 45–70°, SD: 6.52), respectively. No statistically significant difference was found between two groups in terms of range of motion (forward elevation, abduction, and external rotation; Table 2) When the number of re-dislocations was compared, no significant difference was found between two groups (p > 0.05). At the latest follow-up, the apprehension test and O’Brien test were negative for both groups. No statistically significant difference was found in apprehension tests and O’Brien tests between two groups.
Final follow-up outcome scores.
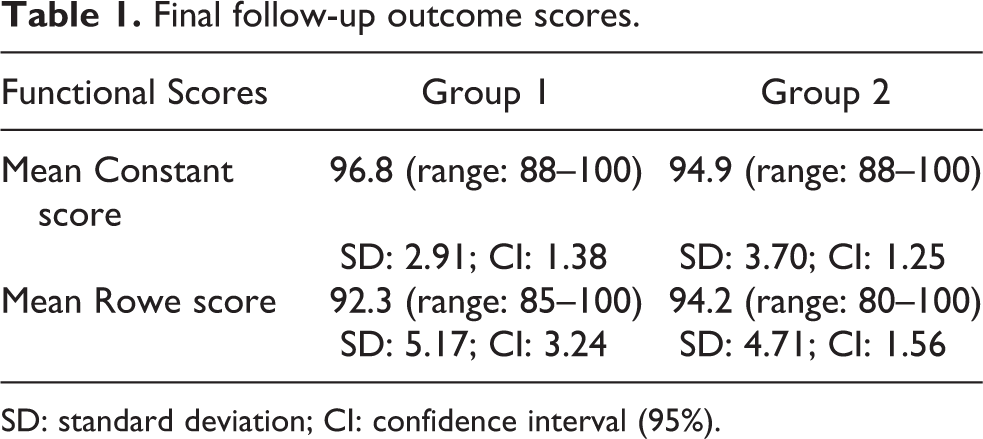
SD: standard deviation; CI: confidence interval (95%).
Mean range of motion at the latest follow-up (group 1/group 2).a

SD: standard deviation; CI: confidence interval; NS: statistically no significance.
aThe patients with re-dislocations were not included.
Discussion
It was shown that 5–57% of the patients with recurrent dislocations had combined Bankart and SLAP lesions. 3,12,15,16 The longer interval between injury and surgery and the number of dislocations were shown to play a significant role in the development of the extension of the labral lesion. 3 The increased anteroinferior translation after detachment of the superior labrum may result in increased shoulder instability. Properly fixing the anteroinferior and superior labrum to the glenoid rim decreases joint volume and provides a bumper effect on the humeral head. 3,12,17
In this study, we found no clinical difference between the two groups in terms of the range of motion, re-dislocations, and a clinical SLAP test. Similar to our study, Hantes et al. found almost the same clinical results. 3 Gartsman et al. also reported no association between the recurrence rate and the number of preoperative dislocations. 12 These authors suggested that the repair of soft tissue injury properly which is the most important factor for the success of the surgical treatment of anterior shoulder instability. For a successful result, the repair of an accompanying SLAP lesion will help to restore the capsular volume anatomically. This can be possible when there is no significant bony deficiency as discussed in our study.
The coexistence of Bankart lesion with SLAP lesion may cause technical difficulties during arthroscopic repair. The sagging SLAP lesion may block the vision of scope, which is inserted from posterior portal. 18 Burkhart and Imhoff recommended a technique of hanging the SLAP lesion with a suspension sling for an easy repair. 19 We did not routinely use this technique in our cases. But this can be used in some instances for the reduction of the superior labrum. Even some authors advocate the direction of repair from posterior superior to anterior inferior, we started the repair of the combined lesions from anterior-inferior to posterior-superior directions using knotless anchors. 10 We believe that this will be helpful to perform the best reduction at the anteroinferior labrum. Contrary to our experience, Cho et al., in their series, first repaired the unstable SLAP lesion and then the Bankart lesion in combined lesions. They found that the Bankart lesion could be repaired properly if the unstable SLAP lesion was repaired first. 10 As a fixation material, we did not use metal or bioabsorbable anchors because of published complications such as osteolysis, pseudocysts, or chondrolysis. 20,21 All anchors used in our study were PEEK anchors. The use of knotless anchors is not cost-effective, but there are some advantages: a shorter operation duration, easy handling, and the prevention of high-profiled intra-articular suture remnants which may cause friction. 22 The tightness of the repair must be well-balanced to prevent postoperative stiffness and re-dislocation. 23
Hantes et al. reported 25 cases of combined Bankart and SLAP lesions in a series of 65 patients who underwent arthroscopic repair for anterior glenohumeral instability. Their 2-year follow-up results did not show any difference regarding joint stability or functional results. 3 Cho et al. reviewed 15 cases with combined Bankart and SLAP lesions among 62 patients who underwent arthroscopic repair with absorbable anchors. They found no difference between the two groups in terms of visual analogue scale, American Shoulder and Elbow Surgeons, or Rowe scores. However, their findings showed that the range of motion after arthroscopic repair in combined lesions increased more slowly than in patients with only Bankart repair. 10 On the contrary, in our patient groups, we did not notice such slow rehabilitation improvement.
Similar to other studies, we did not find any difference regarding the re-dislocation rate and functional scores between two groups. 12,23 The clinical results of our study were evaluated by Constant and Rowe scores. We believed that it would make sense to clinically evaluate the biceps anchor or tendon. Thus, both Constant and Rowe scores do not reflect biceps anchor pathologies and associated complaints. Therefore, SLAP and the long head of biceps pain were evaluated by the O’Brien test. The O’Brien test has the highest sensitivity when compared to the other SLAP tests. 24 None of the patients had a positive O’Brien test. This shows that combined SLAP repair healed clinically without pain.
We excluded the patients older than 35 years old in this study. The reason for this exclusion is about the general success of the SLAP repairs. The initial studies suggested an extremely high level of success in arthroscopic SLAP repairs. 25 Provencher et al. found a 37% failure rate and returned to previous activity after SLAP repair limited in patients more than 36 years old. They reported 28% revision surgery. 26 Because of limited results in older patients, Boileau et al. suggested tenodesis of the biceps tendon for SLAP lesions in patients. They found superior results in older patients when treated with tenodesis. 27,28 Because of this, we included only the patients less than 35 years old so as not to interfere with the poor results of SLAP repairs in older patients.
One of the shortcomings of the study is not having had a postoperative MRI evaluation. It might have been interesting to detect bicipital pathologies on MRI. However, our study focuses mainly on the clinical rather than radiological results. Another issue may be the repair or non-repair of the SLAP lesions in instability patients. This might be the basis for a more interesting study. However, for ethical reasons, we believe this would be difficult to do in our facility.
Conclusion
Properly repaired labral tears, extending from the anterior inferior to the posterior superior of the glenoid, do not affect the overall results of instability treatment. Accompanying SLAP repair does not make any difference in overall clinical results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.