
Abstract
Background:
The results of surgical treatment of shoulder injuries in high-level male gymnasts have not yet been documented.
Purpose:
To evaluate the functional and subjective results after surgical treatment of shoulder injuries in high-level gymnasts and the possibilities to return to sport at the same level.
Study Design:
Case series; Level of evidence, 4.
Methods:
Over a 20-year period (1994-2014), 23 high-level male gymnasts (26 shoulders) underwent surgery by a single experienced shoulder surgeon. At the time of surgery, 7 gymnasts competed at the international level, 12 at the national elite level, and 4 at the regional level. According to symptoms and anatomic lesions, the shoulders were classified into 2 groups: painful shoulders (n = 11) and unstable shoulders (n = 15). Fifteen capsulolabral repairs, 10 cuff debridements, 1 cuff repair, 4 SLAP (superior labral anterior and posterior) repairs, and 8 suprapectoral biceps tenodesis were performed. Twelve shoulders (46%) had >1 procedure performed. Outcomes assessment was performed by an independent observer at a mean of 5 years (range, 2-15 years) postoperatively. In addition, patients completed the Subjective Shoulder Value (range, 0%-100%).
Results:
After shoulder surgery, 21 (91%) of the 23 gymnasts returned to competitive gymnastics, and 20 gymnasts (87%) regained their preinjury level of sport. All international-level gymnasts returned to their preinjury level of sport. Three athletes (13%) underwent revision surgery, and 1 athlete (4%) ended his career without returning to competition. The postoperative period before resumption of competitive gymnastics was 9 ± 3.5 months (mean ± SD). Of the 15 gymnasts treated for shoulder instability with arthroscopic stabilization, 12 were able to return to their previous level of sport. All 8 gymnasts who had arthroscopic biceps tenodesis were able to return to their previous level of sport, as opposed to only 2 of 4 gymnasts treated with SLAP repair. The gymnastics-specific Subjective Shoulder Value score was 80% ± 11%.
Conclusion:
Most gymnasts who required surgical treatment for a shoulder injury were able to return to competition at their previous level, although there was a considerable postoperative recovery period. Current arthroscopic reconstruction techniques were effective for treating structural lesions and allowing return to high-level gymnastics.
Artistic gymnastics subjects the athlete’s shoulder to considerable forces with specific biomechanics, as gymnasts rapidly combine complex movements with extremes of humeral rotation. 16,28 Gymnasts bear their body weight on the support arm while using support apparatus (floor exercises, pommel horse, the beam, and the vaulting table) or they carry body weight using suspension apparatus (the rings, the parallel bars, the uneven bars, and the horizontal bar). Existing literature has focused on biomechanical studies 2,12,26,32 performed during gymnastic activity.
The results of surgical treatment for shoulder injuries in high-level gymnasts have not yet been documented, despite a relatively high rate of shoulder injuries in male gymnasts (16.8%-19% of all gymnastic injuries). 13 Caine and Nassar 13 reported a lower frequency of shoulder injuries in women (0%-4.2% of all gymnastic injuries). This disparity may reflect the different types of gymnastic apparatus used by men (suspension and acrobatics apparatus such as the horizontal or the parallel bars) and the greater physical demands placed on the upper limbs and body in the men’s gymnastics maneuvers (eg, the iron cross position on the rings). 2,3,19
Many questions remain unanswered when surgeons have to deal with injured shoulders in athletes such as high-level gymnasts, who place high loads on their upper limbs during weightbearing and suspensory exercises. First, the diagnosis may be difficult since ligamentous and tendinous lesions may be present, adding some confusion. For instance, a deep partial supraspinatus tear can be isolated or combined with an anteroinferior labral tear (in case of shoulder instability) or with a posterosuperior labral tear (in case of posterosuperior glenoid impingement). 17 Second, whatever lesions are observed during arthroscopy (tendinous and/or ligamentous), the surgical treatment remains controversial. For instance, in the case of an articular-side supraspinatus tear, the question arises: Should the surgeon perform only an arthroscopic tendon debridement or complete and repair the tendon tear? Similarly, the surgeon who has to treat an unstable shoulder in a high-level gymnast faces a cruel dilemma: If the shoulder is too tight, the gymnast will not be able to do the dislocation maneuver (which is needed to accomplish some acrobatic figures), whereas if the shoulder is too loose, there is a risk of recurrent instability. Another unsolved problem is the treatment of disinsertion of the biceps anchor (type 2 SLAP [superior labral anterior and posterior] lesion). The following questions arise: Is it reasonable to perform biceps tenodesis in a high-level gymnast? Or is it preferable to perform a SLAP repair with the risk of having persistent shoulder pain and stiffness, which preclude return to high-level sport? Finally—as the last and probably most stressful question for the surgeon—will this high-level gymnast be able to return to competition at the same level after surgery?
This is part 2 of a 2-part study. The objectives of part 1 were to describe the epidemiology and provide a pathoanatomic classification of shoulder lesions in high-level gymnasts. 18 The aim of part 2 was to evaluate the results of shoulder surgery in high-level gymnasts. We hypothesized that return to the preinjury level of gymnastics is possible after shoulder surgery.
Methods
Study Design
This was a retrospective case series of gymnasts’ shoulders treated surgically from 1994 to 2014, with a minimum follow-up period of 2 years. The ethics committee of our institution provided approval for this study. Inclusion criteria for the study included the following: (1) athletes competing at or above the regional level; (2) shoulder injuries precluding training and competition that were sustained during gymnastics and referred by the medical staff (rehabilitation specialists, sports physicians, and coaches) of the national gymnastics training center in Antibes, France; and (3) athletes treated with surgical procedures by the senior shoulder surgeon. Study exclusion criteria were a history of ipsilateral shoulder surgery in another unit (3 cases) and gymnasts already at the end of their careers (1 case).
Study Population
A total of 23 high-level male gymnasts (26 shoulders) met the inclusion criteria for the study. Three gymnasts underwent surgery on both shoulders. The mean age at surgery was 22 years (range, 16-33 years). All gymnasts performed all routines. The support arm (the weightbearing arm when the gymnast moves on 1 arm) was involved in 15 cases. All patients had failed nonoperative treatment. At the time of surgery, 7 gymnasts competed at the international level, 12 at the national elite level, and 4 at the regional level. The mean weekly training regime was 22.5 hours (range, 12-30 hours). The mean duration of symptoms before surgery was 8 months (range, 6-24 months).
Pathoanatomy
Using the groupings developed in part 1 of this study, 18 the shoulder pathologies and symptoms were classified into 2 groups according to the clinical, radiological, and arthroscopic findings: painful or unstable shoulders. In 12 of 26 shoulders (46%), there were several associated lesions.
Painful Shoulder Group
Eleven shoulders demonstrated no clinical, radiological, or arthroscopic findings of instability. In this group, patients were diagnosed with posterosuperior glenoid impingement 36 (n = 3), articular-side supraspinatus tear (n = 5), and biceps tear (n = 3).
Unstable Shoulder Group
Fifteen shoulders presented a history or lesion of instability, including 1 isolated traumatic dislocation and 7 isolated subluxations. In the other 7 cases, there were obvious anatomic lesions of instability, with excessive glenohumeral translation during arthroscopy (>75%). Although the gymnasts could not recall any clear shoulder dislocation or subluxation episodes, here the capsulolabral tears were considered witnesses of unrecognized subluxations, and the location oriented the direction of the instability. 10
Surgical Procedures
All procedures were performed under general anesthesia with interscalene nerve block and the patient in a beach-chair position. The patient’s arm was placed in a mobile gutter support without traction, allowing the surgeon to mobilize the limb as required. A single experienced shoulder surgeon performed arthroscopic diagnosis and treatment (P.B.). Table 1 shows the surgical procedures performed according to the principal and associated pathological lesions found.
Pathological Lesions Seen at Index Arthroscopy and Surgical Procedures Performed a

a LHB, long head of the biceps; PS, painful shoulder; PSGI, posterosuperior glenoid impingement; SLAP, superior labral anterior and posterior; SSP, supraspinatus; US, unstable shoulder.
Outcome Assessment
Assessment was performed by an independent surgeon, himself a former high-level gymnast and orthopaedic surgeon, at a mean of 5 years (range, 2-15 years) postoperatively (P.G.). No patients were lost to follow-up. Functional outcomes were assessed with a structured interview and detailed physical examination using the Constant-Murley score. 15 The Walch-Duplay and Rowe scores were employed for the unstable painful shoulder group as part of the assessment. 31,37 Elbow flexion and forearm supination strengths were also evaluated using mechanical dynamometers (MSE100; Chatillon) in all patients who underwent surgery on the long head of the biceps (Figure 1). Mechanical testing was bilateral, with findings being compared with the noninjured side.

Measurements of strength in (A) elbow flexion and (B) forearm supination using mechanical dynamometers. These measurements were made on the operated side and the contralateral side in all patients who underwent a SLAP (superior labral anterior and posterior) repair or a biceps tenodesis.
We recorded the time needed for athletes to return to their initial levels of using all gymnastic apparatus. The Subjective Shoulder Value (SSV) was used to evaluate the operated shoulder relative to a healthy shoulder during activities of daily living. 20 We also used the SSV-Gym to adapt the subjective assessment of the shoulder to the specific constraints of gymnastics and, like the SSV, is recorded as a percentage from 0% to 100%. The patients’ subjective satisfaction with surgery was assessed with 3 questions: “Are you very satisfied, satisfied, dissatisfied, or disappointed with the outcome of your shoulder treatment?” “Would you be willing to repeat this procedure for the same problem?” “Would you recommend this procedure to a patient who had the same initial complaint?”
Statistical Analysis
We performed descriptive statistics, including calculation of mean data and indicating maximum, minimum, and standard deviation. We also conducted comparative statistics using a comparison test of means (Student t test) or the Mann-Whitney test depending on the normality of data distribution or otherwise, as assessed by the Agostino-Pearson test. Results were considered statistically significant if P < .05. Statistical calculations were performed with MedCalc software (Version 8.0; MedCalc).
Results
Complications and Reoperations
Three gymnasts in the unstable shoulder group had failure of the index procedure and underwent reoperation; their results were included in the final assessment. One of these patients had recurrent instability and underwent revision surgery at 18 months postoperatively with an open Latarjet 35 procedure for failed Bankart repair. He was able to return to competition and to his preoperative level after the Latarjet procedure. The second patient had persistent shoulder pain with anterior apprehension and subluxation and was unable to resume gymnastics at 1 year after Bankart repair. This gymnast underwent revision with a repeat arthroscopic Bankart repair, was not able to return to his preoperative level, and ended his career. The third gymnast had failure of a biceps tenodesis 4 weeks after surgery while carrying a heavy object despite being instructed to avoid lifting. This patient underwent revision biceps tenodesis with success and returned to competition.
Return to Competitive Gymnastics
The time taken to return to competitive sport, the level of gymnastics attained after surgery, and the SSV-Gym scores are summarized in Table 2. The overall mean ± SD postoperative period before resuming competitive gymnastics was 9 ± 3.5 months (range, 3-18 months).
Return to Sport and SSV-Gym Scores for the Study Groups a
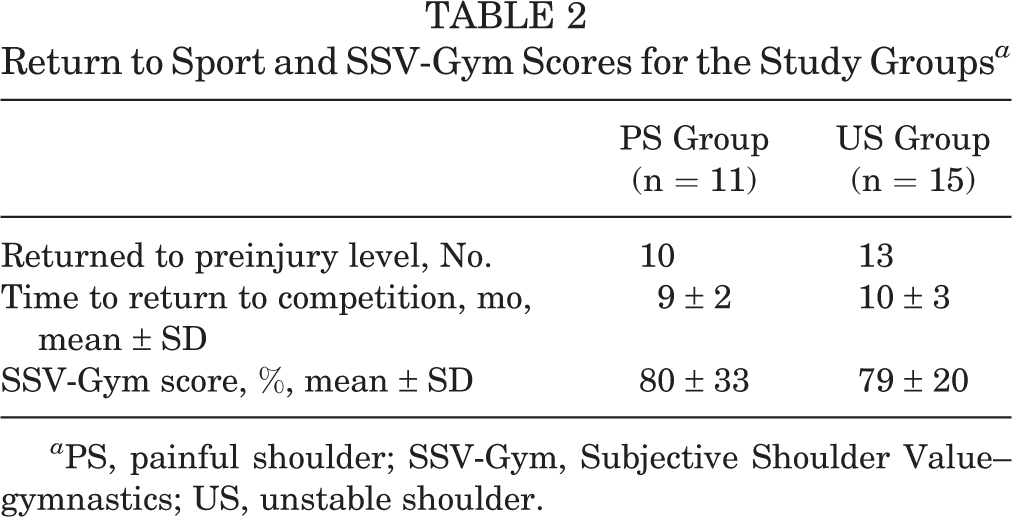
a PS, painful shoulder; SSV-Gym, Subjective Shoulder Value–gymnastics; US, unstable shoulder.
After shoulder surgery, 21 (91%) of the 23 gymnasts returned to competitive gymnastics, and 20 gymnasts (87%) regained their preinjury level of sport and returned to the same level of competition. All gymnasts at the international level returned to their preinjury level of sport. Two gymnasts won an Olympic medal: 1 in Sydney in 2000 and 1 in Beijing in 2008. One gymnast at the national level decreased his level of competition because of persistent pain during suspension exercises after arthroscopic Bankart and type 2 SLAP repair. Two national-level gymnasts ended their careers: the first had stiffness and pain after arthroscopic stabilization (gymnast who underwent revision with a repeat arthroscopic Bankart repair), whereas the second had persistent pain performing suspension exercises (the rings and the horizontal bars) after isolated type 2 SLAP repair.
Functional Results
There was no significant change in active forward flexion or internal rotation, but a decrease was evident in external rotation (from 65° to 54°; P = .01) across the groups. The overall mean Constant score significantly improved (P < .01) (Table 3).
Clinical Outcome Measurements (N = 26 Shoulders) a

a Values are presented as mean ± SD. NS, not significant.
Results According to Symptoms and Anatomic Lesions
In the unstable shoulder group (n = 15), results were considered excellent in 5 cases, good in 8 cases, and fair in 2 cases according to the Walch-Duplay and Rowe scores. Ten gymnasts had pain or discomfort during gymnastics. However, 3 gymnasts experienced persistent apprehension, specifically when using suspension apparatus with exercises requiring hyperabduction associated with humeral rotation (Table 4).
Instability Scores for the Unstable Shoulder Group (n = 15)

All gymnasts were able to return to competition and to their previous level of sport after suprapectoral biceps tenodesis (8 gymnasts), and 2 of 4 gymnasts returned to the same level after SLAP repair.
Strength in Elbow Flexion and Forearm Supination
No significant differences in elbow flexion and forearm supination strength were found between the gymnasts who underwent SLAP repair versus biceps tenodesis (Figure 2). There was also no difference to these strengths when comparing the operated shoulder with the contralateral noninjured shoulder (Table 5).
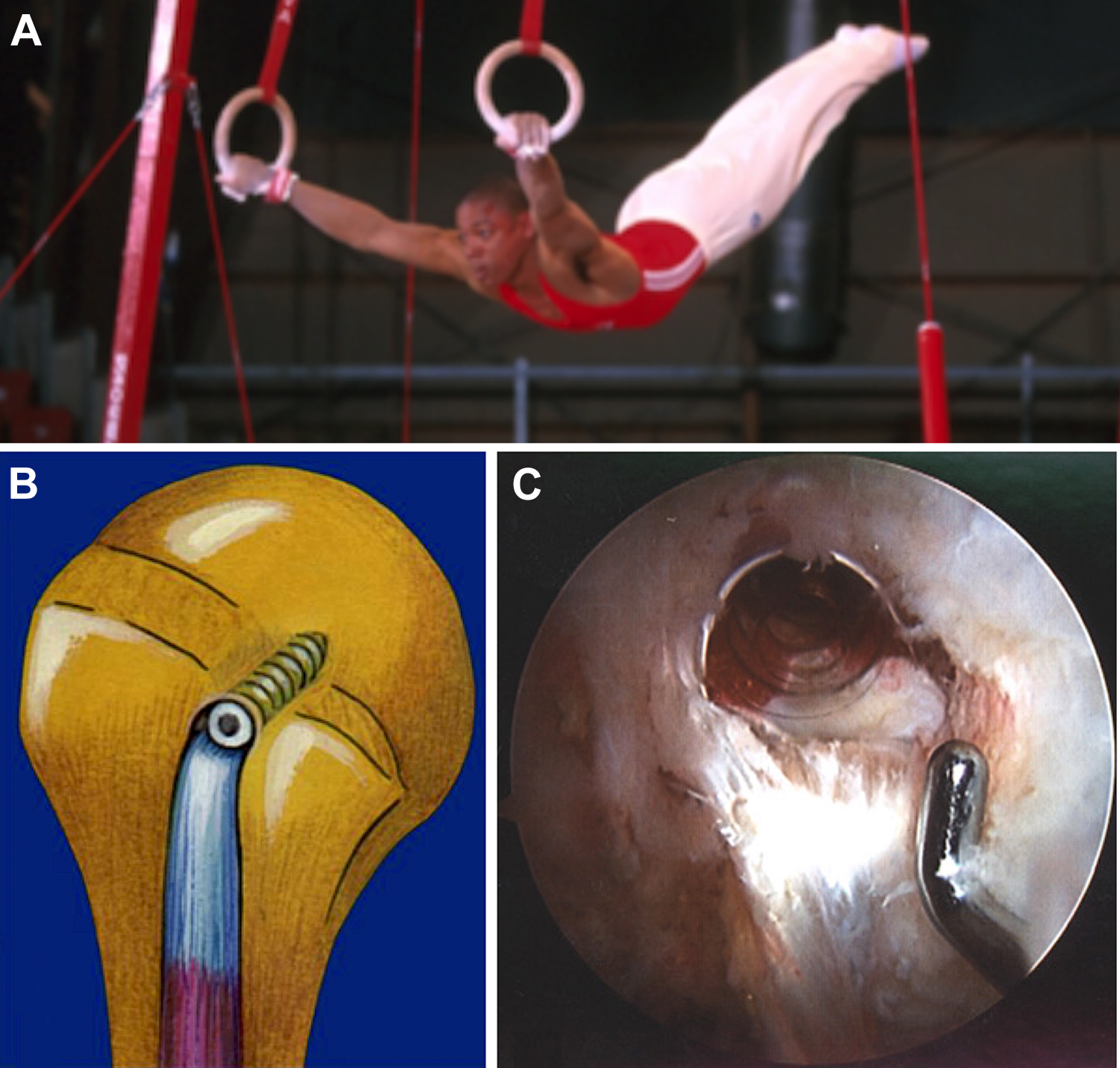
(A) French gymnast on the rings during the 2003 world championship 2 years after Bankart repair on the left shoulder and (B, C) 1 year after cuff repair and biceps tenodesis with interference screw on the right shoulder.
Elbow Flexion and Forearm Supination Strength as Measured by Dynamometer a
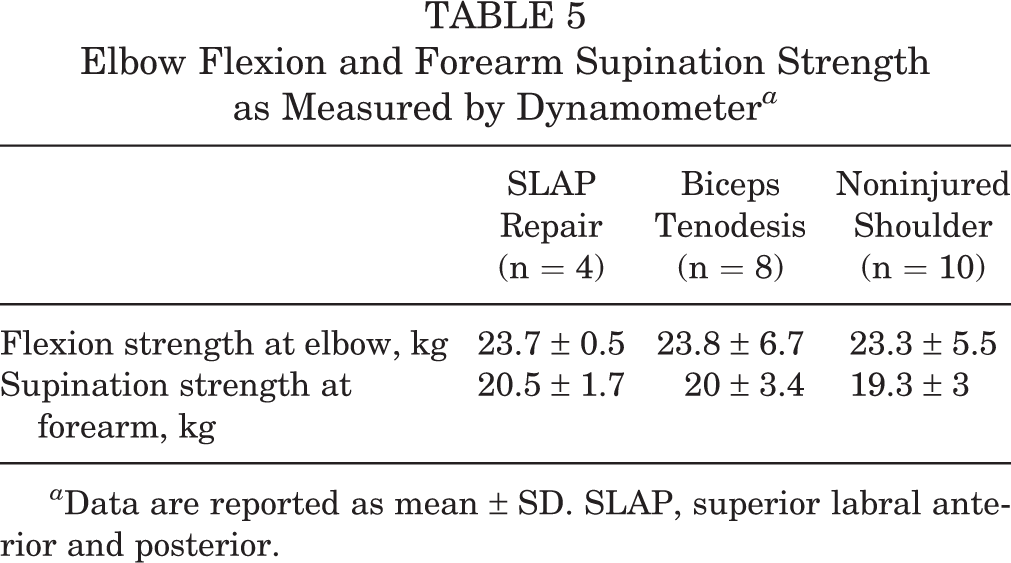
a Data are reported as mean ± SD. SLAP, superior labral anterior and posterior.
Subjective Outcomes
Regarding the 22 shoulders in the 20 gymnasts (87%) who returned to high-level gymnastics, patients were satisfied with their shoulders in 12 cases and very satisfied in 10 cases at final follow-up. Results for the 4 shoulders in the 3 remaining gymnasts were disappointing; these included the 2 gymnasts who ended their careers and the gymnast who decreased his level of competition. All gymnasts stated they would be willing to repeat the procedure and would recommend the procedure to a patient with a similar problem. The SSV was 96% ± 10% (range, 50%-100%) for activities of daily living and 80% ± 11% (range, 0%-100%) for the practice of gymnastics.
Discussion
The pertinent finding of our study is that shoulder surgery need not end the career of a high-level male gymnast, with 21 (91%) of the 23 study patients returning to competitive gymnastics and 20 gymnasts (87%) regaining their preinjury level of sport. The Constant-Murley score was excellent at the last follow-up but probably suffered from a ceiling effect in these high-level athletes. The SSV-Gym adapted the subjective assessment of the shoulder to the specific constraints of gymnastics and seemed to give a more representative score in this population, which scored a mean 80% (range, 0%-100%) at the last follow-up.
Our study confirms that modern arthroscopic reconstructive techniques are efficient for treating structural lesions and allow return to high-level gymnastics, including competition at an international level. However, athletes, coaches, physical therapists, sport doctors, and surgeons should be aware that after surgical treatment, the mean time taken to resume competitive gymnastics is long (9 months to 1 year). This is a considerable setback for a top athlete, almost a full season of sport. The reasons for delayed return are multifactorial and may be related to the following: (1) the loss of shoulder musculature attributed to postoperative inactivity; (2) the long time needed for recovering enough shoulder laxity necessary for gymnastics (capsular stretching exercises are permitted only once healing and recovery of a normal range of motion are achieved); and (3) the extreme loads put on shoulders when performing suspension apparatus exercises (these exercises were resumed late owing to the large tensile force on the shoulders). 11,22
Shoulder instability is not rare in gymnasts (15 of 26 patients in our series), with most patients experiencing subluxations (and not dislocations), apprehension, or pain when performing suspension figures with the bars or the rings. Shoulder stabilization in high-level gymnasts is challenging, since the athletes need to perform inferior stretching of their shoulders during some figures on suspensory apparatus (see part 1 of this study 18 ). All gymnasts have acquired inferior laxity with an enlarged or stretched joint capsule to allow rotational movements when their hands are locked on the bars or rings. In this population, the senior surgeon chose to perform the most anatomic procedure (P.B.): all gymnasts with shoulder instability were treated with arthroscopic soft tissue repair using suture and absorbable anchors (ie, Bankart repair with some capsular retensioning). 4,9 Although arthroscopic shoulder stabilization allowed most of them to return to their previous level of gymnastics, two-thirds were still experiencing some pain during practice.
Two of 15 gymnasts experienced recurrent instability after soft tissue procedures and needed to undergo reoperation: one had an open Latarjet procedure whereas the other had another Bankart repair with capsular shift. Our study shows that the Latarjet procedure can be an efficient alternative to a soft tissue procedure in case of failed Bankart repair. However, although return to the same level of competition is possible after the Latarjet procedure, transfer of the coracoid process and conjoined tendon may pose a theoretical obstacle to the “dislocation exercise.” The gymnast who underwent reoperation with a Latarjet procedure demonstrated that the stresses on the coracoid fragment could lead to early partial bone block lysis and screw breakage (Figure 3). Since the repositioned conjoined tendon allows reinforcement of the overstretched inferior glenohumeral ligament (sling effect), the Trillat procedure may be a better option in the high-level gymnast with an unstable shoulder and poor capsular tissues. 34,38

Successful shoulder stabilization with an open Latarjet procedure after failed Bankart procedure in an international-level French gymnast. The need for male gymnasts to dislocate their shoulders during some acrobatic figures may explain the partial lysis of the coracoid bone block and the broken screw seen on radiographs taken 2 years after surgery. The sling effect given by the transposed conjoint tendon may contribute to stabilization of the shoulder.
In 6 gymnasts in the unstable shoulder group, arthroscopic exploration of the shoulder allowed us to find some instability lesions involving the inferior labrum and capsule, even though these athletes did not specify instability symptoms, only chronic shoulder pain. Although these athletes did not recall any subluxation or dislocation episodes, they were diagnosed as having an unstable painful shoulder. 10 All 6 gymnasts with unstable painful shoulder were treated with arthroscopic Bankart repair or isolated capsular plication and were able to return to their previous level of competition. Surgeons should be aware that isolated capsular enlargement is frequently seen in asymptomatic athletes (as a result of overuse) and is usually not sufficient to make the diagnosis of unstable painful shoulder. The diagnosis of unstable painful shoulder should be made only if true anatomic lesions of instability (so-called roll-over lesions) are present on imaging studies and/or at arthroscopy. 10
From a diagnostic and therapeutic standpoint, partial articular-side supraspinatus tears are a challenging problem in high-level gymnasts. 1,29,34 In our series, all 8 gymnasts with partial-thickness rotator cuff tears and chronic shoulder pain were able to return to their previous level of sport: 7 were treated with arthroscopic cuff debridement and 1 with completion and cuff repair. 5 Of the 7 athletes treated with arthroscopic debridement, 6 returned to their preoperative athletic activity. Tomlinson and Glousman 33 reported on 46 throwing athletes who underwent arthroscopic glenoid labral tear debridement and found that only 54% had good to excellent results. They concluded that arthroscopic debridement of glenoid labral lesions does not yield consistent long-term results. Arthroscopic debridement of the deep surface of the supraspinatus tendon associated with lesions of the posterosuperior glenoid rim is recommended treatment for posterosuperior glenoid impingement, although results have been variable. 29,33,36 Riand et al 29 noted that in 75 throwing athletes with posterosuperior glenoid impingement treated with arthroscopic debridement, just 12 patients had returned to their former level of sport.
Arthroscopic repair of type 2 SLAP lesions is still controversial. 23,24,39 Unfortunately, our study does not provide an answer to the question of why some athletes experience performance-limiting pain after SLAP repair. In our series, only 2 of 4 gymnasts were able to return to high-level gymnastics after SLAP repair. One explanation may be that the superior labrum is subjected to excessive traction, up to 6- to 8.5-times body weight, during ring or high bar suspension exercises. 11,14,22 Another explanation may be that despite reattaching the superior labrum using absorbable suture anchors, SLAP repair may create too rigid fixation. 8 De Carli et al 17 reported that SLAP tears seemed to be responsible for most cases of early retirement in gymnasts.
We have already reported our disappointing experience with arthroscopic repair of type 2 SLAP lesions and shown that arthroscopic biceps tenodesis could be an effective alternative to SLAP repair. 8 In the present series, the 8 gymnasts who had arthroscopic suprapectoral biceps tenodesis with interference screw fixation were able to return to their previous level of sport, which confirms our previous findings. Furthermore, no difference was found in elbow flexion and forearm supination strengths between the operated and noninjured sides in the gymnasts treated with either SLAP repair or biceps tenodesis. Arthroscopic suprapectoral biceps tenodesis using interference screw fixation is superior to using simple sutures or suture anchors 21,25,27,30 and is, in our opinion, more appropriate in high-level gymnasts, where the upper limbs are subjected to large tensile forces, especially during suspension exercises. 6,7 Our results may not be transposable with other techniques of fixation (soft tissue or suture anchor fixation).
To the best of our knowledge, this is the first report of arthroscopic surgical treatment of shoulder injuries in a large series of high-level gymnasts with a long follow-up period. Other strengths of this study were that first, all arthroscopic diagnoses and procedures were performed by a single experienced shoulder surgeon; second, all athletes were prospectively followed with minimum 2 years; and, third, patient evaluation was performed by an independent observer, himself a former high-level gymnast and shoulder surgeon. The main limitation of our study was its retrospective nature with mixed pathology and the absence of a control group, which was impossible in the given context. Some preoperative data were missing for Rowe and Walch-Duplay scores. The Constant-Murley score probably suffered from a ceiling effect in these high-level athletes.
Conclusion
Modern arthroscopic reconstructive techniques were efficient for treating structural lesions and allowed return to high-level gymnastics in about 90% of cases. Although shoulder surgery did not compromise the careers of these high-level gymnasts, there was a considerable postoperative recovery period (9 months to 1 year) before resumption of competitive gymnastics. The injured high-level gymnast shoulder often presented with associated tendinous and capsulolabral lesions, which must be all treated at the time of surgery. Arthroscopic Bankart repair and capsular shift were efficient procedures to stabilize the unstable gymnasts’ shoulders. Arthroscopic cuff debridement was efficient for articular-side supraspinatus tears involving <50% of the tendon’s thickness. The results of arthroscopic SLAP repairs were inconsistent, and biceps tenodesis can be an alternative. No difference in elbow flexion and forearm supination strength was found between the gymnasts who underwent SLAP repair and those who underwent biceps tenodesis.
Footnotes
Acknowledgment
The authors thank Laury Païdassi, MD, Philippe Oddoux, and Luc d’Asnières de Veigy for their help with management of high-level gymnasts and Robert Houghton-Clemmey for his help with English writing and translation.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.B. has received consulting fees from Smith & Nephew and royalties from Tornier/Wright. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Final revision submitted April 27, 2021; accepted May 4, 2021.
Ethical approval for this study was obtained from the University Institute for Locomotion and Sports (2016-03).