
Abstract
Background:
The efficacy and safety of anti–nerve growth factor (NGF) antibody therapy used for osteoarthritis (OA) pain are controversial.
Purpose:
To evaluate the efficacy and safety of anti-NGF antibody therapy via a meta-analysis of randomized controlled trials (RCTs).
Study Design:
Systematic review; Level of evidence, 1.
Methods:
PubMed, the Cochrane Central Register of Controlled Trials, Embase, and the Web of Science databases were searched for RCTs assessing anti-NGF antibody treatments for hip and knee OA. A total of 623 records were retrieved from the databases. A random-effects model was used to assess primary and secondary outcomes. Bias was assessed using the Cochrane Collaboration tool, funnel plots, and the Egger test. Subgroup analyses were used to assess the efficacy and safety of the independent variables. Sensitivity analysis was conducted to evaluate the effectiveness of tanezumab and the effectiveness of anti-NGF antibodies compared to active comparator drugs. We present the effects of dose, administration mode, and treatment duration on the efficacy and safety of anti-NGF antibody therapy.
Results:
There were 19 RCTs included in our meta-analysis. Anti-NGF antibody treatment showed significant improvements on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) for pain, physical function, and stiffness as well as on a patient global assessment (PGA). The overall standardized mean differences were as follows: WOMAC pain (–0.31 [95% CI, –0.36 to –0.26]; Z = 11.75; P < .001; I 2 = 38%), WOMAC physical function (−0.36 [95% CI, –0.41 to –0.30]; Z = 12.67; P < .001; I 2 = 44%), WOMAC stiffness (–3.59 [95% CI, –4.87 to –2.30]; Z = 5.47; P < .001; I 2 = 98%), and PGA (−0.28 [95% CI, –0.34 to –0.22]; Z = 9.39; P < .001; I 2 = 50%). Anti-NGF antibody treatment resulted in a greater incidence of adverse events (risk ratio, 1.09 [95% CI, 1.06 to 1.12]; Z = 5.60; P < .001; I 2 = 0%). The incidence of serious adverse events was similar between the treatment and control groups (risk ratio, 1.15 [95% CI, 0.98 to 1.34]; Z = 1.71; P = .09; I 2 = 0%).
Conclusion:
Anti-NGF antibody treatment significantly relieved pain and improved function in patients with hip and knee OA. However, no conclusion could be drawn regarding the optimal treatment plan for anti-NGF antibodies when all 3 variables (dose, administration mode, and treatment duration) were combined in the analyses.
Osteoarthritis (OA) affects approximately 250 million people worldwide and is a major cause of pain and disability among older adults. 20,22 OA is a burden on both individual persons and developed countries, with an effect representing 1.0% to 2.5% of the average gross domestic product. 15,20,31
Joint pain and stiffness are the most common symptoms of OA in patients. 20 Most guidelines recommend a combination of nonpharmacological and analgesic treatments for OA symptoms. 15,21,25 Nonsteroidal anti-inflammatory drugs (NSAIDs) are highly recommended. 25 Because NSAIDs may cause side effects, safety is important when choosing treatments for OA. 20
Nerve growth factor (NGF) is an essential protein for the growth and maintenance of sympathetic and sensory nerves 28 and plays a role in the modulation of nociceptive sensitization. 11 Inflamed tissues resulting from arthritis increase the expression of NGF, thus increasing pain sensation. 8,23,42,43 Anti-NGF antibodies have reduced pain-related behaviors in arthritis animal models, 42 providing support for anti-NGF antibody therapy for OA pain in humans. 16 NGF inhibitors in the advanced phases of development for OA include tanezumab, fasinumab, and fulranumab. Tanezumab is a human immunoglobulin G2 monoclonal anti-NGF antibody that blocks the interaction of NGF with its receptors tropomyosin receptor kinase A (TrkA) and p75. 1 Fasinumab is a fully human high-affinity monoclonal anti-NGF antibody 41 ; fasinumab has a subpicomolar binding affinity for NGF and does not detectably bind to most other members of the neurotrophin family, including brain-derived neurotrophic factor and neurotrophin-3. 41 Fulranumab is a human recombinant immunoglobulin G2 monoclonal anti-NGF antibody that specifically neutralizes the biological actions of NGF. 32
Although meta-analyses of anti-NGF antibody therapy for relieving OA pain have been published, 9,36,37,44 the appropriate dose, administration mode, and treatment duration have not been assessed. The purpose of this study was to present a meta-analysis assessing dose, administration mode, and treatment duration on the efficacy and safety of anti-NGF antibodies for the treatment of hip and knee OA.
Methods
Search Strategy
This meta-analysis was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, 30 and the study protocol was registered with PROSPERO (registration identification CRD42021242967). We searched for relevant double-blind randomized controlled trials (RCTs) in PubMed, Embase, the Web of Science, and the Cochrane Central Register of Controlled Trials databases between inception and March 21, 2021, using a detailed search strategy (Appendix 1). There were no language restrictions.
Inclusion Criteria
The inclusion criteria were as follows: (1) full-text RCT articles; (2) patients with OA of the knee or hip according to the American College of Rheumatology criteria, ranked grade ≥2 according to the Kellgren-Lawrence classification for OA severity; (3) administration of anti-NGF antibodies at any dose versus a placebo or active comparator drug (if both a placebo and active comparator drug were used, only the placebo results were included in the analysis); (4) outcomes of the standardized mean difference (SMD) or mean difference between baseline and the endpoint in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC; pain, physical function, and/or stiffness subscales) and patient global assessment (PGA) scores; and (5) safety data (including the incidence of adverse events [AEs] and serious AEs [SAEs]).
Data Extraction
There were 2 investigators (Y.G. and Z.H.) who independently extracted data from RCTs including the study name, pain condition, sample size, mean age of participants, percentage of included women, content of the experimental and control interventions, and outcomes. When the same research appeared in different articles, only the most complete set of data was selected. Disagreements were arbitrated by a third investigator (Y.H.). The SMDs for outcomes between baseline and the endpoint were pooled. If the mean, standard deviation (SD), or standard error of the mean were not obtainable from the text, values were extracted from diagrams and tables.
Numeric values that were only available from graphs or charts were extracted using GetData Graph Digitizer (Version 2.26; https://apps.automeris.io/wpd/index.zh_CN.html). When only the standard error of the mean was reported, the SD was estimated using the equation
Quality and Risk-of-Bias Assessments
The quality of the RCTs was independently evaluated by 2 investigators (Y.G. and Z.H.) using the Cochrane Collaboration tool, funnel plots, and the Egger test for assessing the risk of bias. 13 A judgment of “yes” indicated a low risk of bias, “no” indicated a high risk of bias, and “unclear” indicated an unclear or unknown risk of bias. When the same research appeared in different articles, only the most complete set of data was selected. The remaining duplicate data were eliminated. Any disagreements regarding data extraction and quality assessment between the 2 investigators were resolved via a consensus or, if necessary, by a third investigator (Y.H.).
Data and Statistical Analyses
The meta-analysis was performed using Review Manager (Version 5.4; Cochrane) and Stata (Version 16.0; StataCorp). SMD changes from baseline to the endpoint in WOMAC scores (pain, physical function, and stiffness) and PGA scores were determined. Secondary outcomes were the incidences of AEs and SAEs. Control groups used either a placebo or active comparator drug. In studies that included results from both placebos and active comparator drugs, only placebo results were extracted.
We conducted subgroup analyses to assess the effects of anti-NGF antibody dose, administration mode, and treatment duration on efficacy and safety. A sensitivity analysis was performed on RCTs that assessed fixed-dose tanezumab. Data from RCTs comparing anti-NGF antibodies and active comparator drugs were extracted separately for the sensitivity analysis.
Continuous outcomes are presented as SMDs with 95% CIs, and dichotomous data are presented as risk ratios (RRs) with 95% CIs. A random-effects model was used to assess variations in the meta-analysis characteristics. Heterogeneity was determined using the I 2 statistic. The significance of pooled effects was evaluated via the Z test. The threshold of significance was set at P < .05.
Results
Study Characteristics
A total of 623 records were retrieved from the databases. Of these, 47 RCTs met initial eligibility criteria. Ultimately, 19 double-blind RCTs § were included in this meta-analysis (Figure 1).

Study selection flowchart. RCT, randomized controlled trial.
The characteristics of the included RCTs are shown in Table 1. The RCTs were double-blind, parallel-group, and placebo or active comparator drug–controlled studies. In the 19 RCTs, 13 used tanezumab ∥ , 4 used fulranumab, 23,27,32,33 and 2 used fasinumab. 10,41 In addition, 10 included only intravenous (IV) injections, ¶ 8 included only subcutaneous (SC) injections, 3,10,18,23,27,32,33,34 and 1 included both modes. 4 There were 4 studies that included active comparator drug controls, 14,18,27,40 and 6 studies reported outcomes at 8 weeks. 2,4,14,29,40,41
Characteristics of Included Studies a
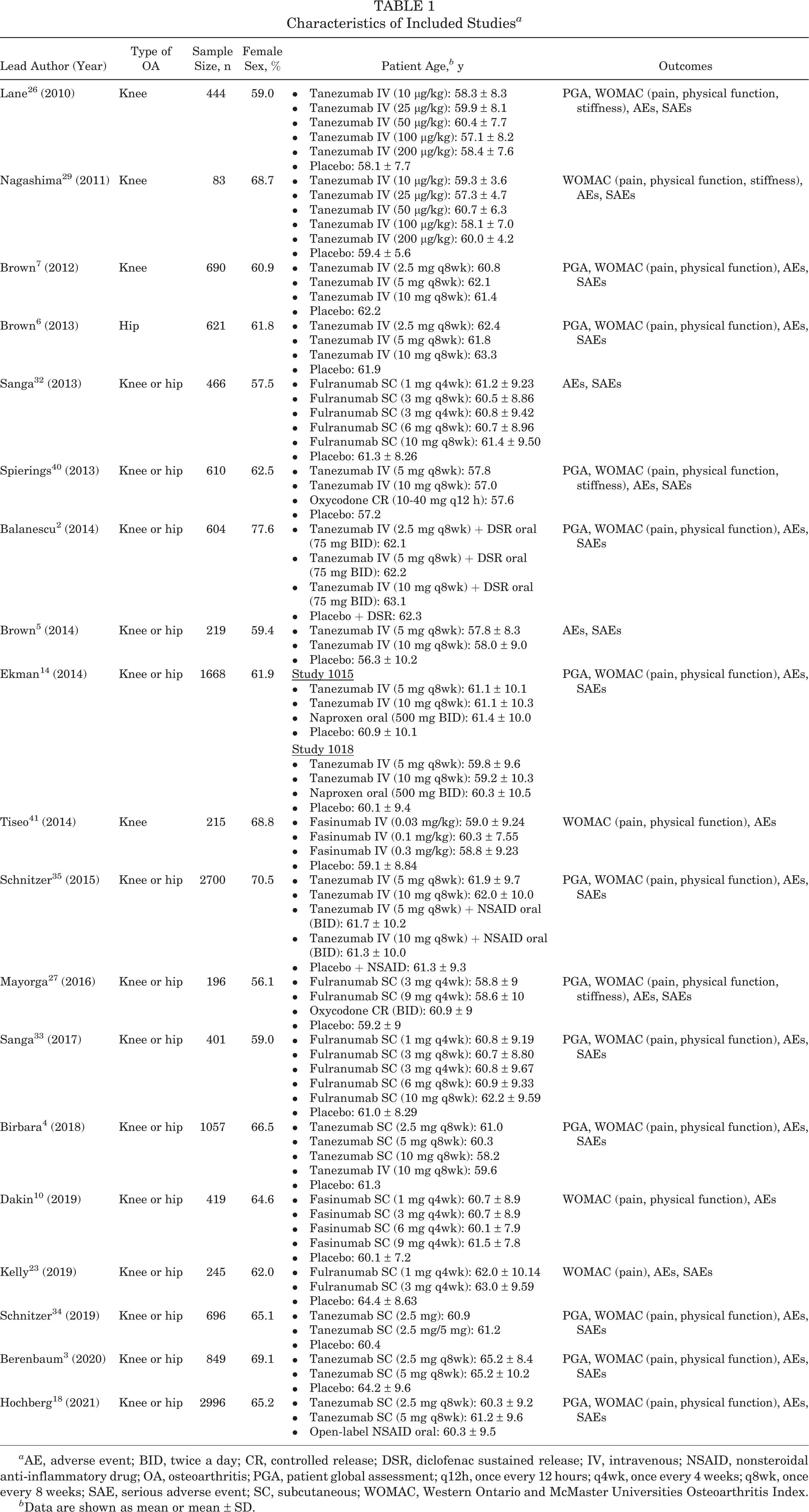
a AE, adverse event; BID, twice a day; CR, controlled release; DSR, diclofenac sustained release; IV, intravenous; NSAID, nonsteroidal anti-inflammatory drug; OA, osteoarthritis; PGA, patient global assessment; q12h, once every 12 hours; q4wk, once every 4 weeks; q8wk, once every 8 weeks; SAE, serious adverse event; SC, subcutaneous; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Data are shown as mean or mean ± SD.
Most of the RCTs used fixed-dose drugs, but 3 studies used weight-adjusted drugs. 26,29,41 According to the methods of a previous meta-analysis, 9 the classification of drug metering in the literature, and a comparison of drug doses in different studies, we divided drug doses into 3 levels. The low-dose subgroup included tanezumab (10 μg/kg, 25 μg/kg, and 2.5 mg), fulranumab (1 mg every 4 weeks and 3 mg every 8 weeks), and fasinumab (0.03 mg/kg, 1 mg, and 3 mg). The moderate-dose subgroup included tanezumab (50 μg/kg and 5 mg), fulranumab (3 mg every 4 weeks and 6 mg every 8 weeks), and fasinumab (0.1 mg/kg and 6 mg). The high-dose subgroup included tanezumab (100 μg/kg, 200 μg/kg, and 10 mg), fulranumab (10 mg every 8 weeks), and fasinumab (0.3 mg/kg and 9 mg).
Risk of Bias
The assessment of the risk of bias in the RCTs is shown in Figure 2. A total of 7 studies had insufficient information about random sequence generation and allocation concealment, 2,4,6,7,14,40,41 4 lacked information regarding blinding of participants, 4,14,18,40 7 lacked information regarding blinding of outcome assessors, 4,14,18,27,32,33,40 and 5 showed a high risk of bias for incomplete outcome data. 2,4,14,23,27 All RCTs showed a low risk of selective reporting bias. Other biases in the RCTs were unclear (all research was sponsored by pharmaceutical companies). # Overall, the quality of the reported trials was high.
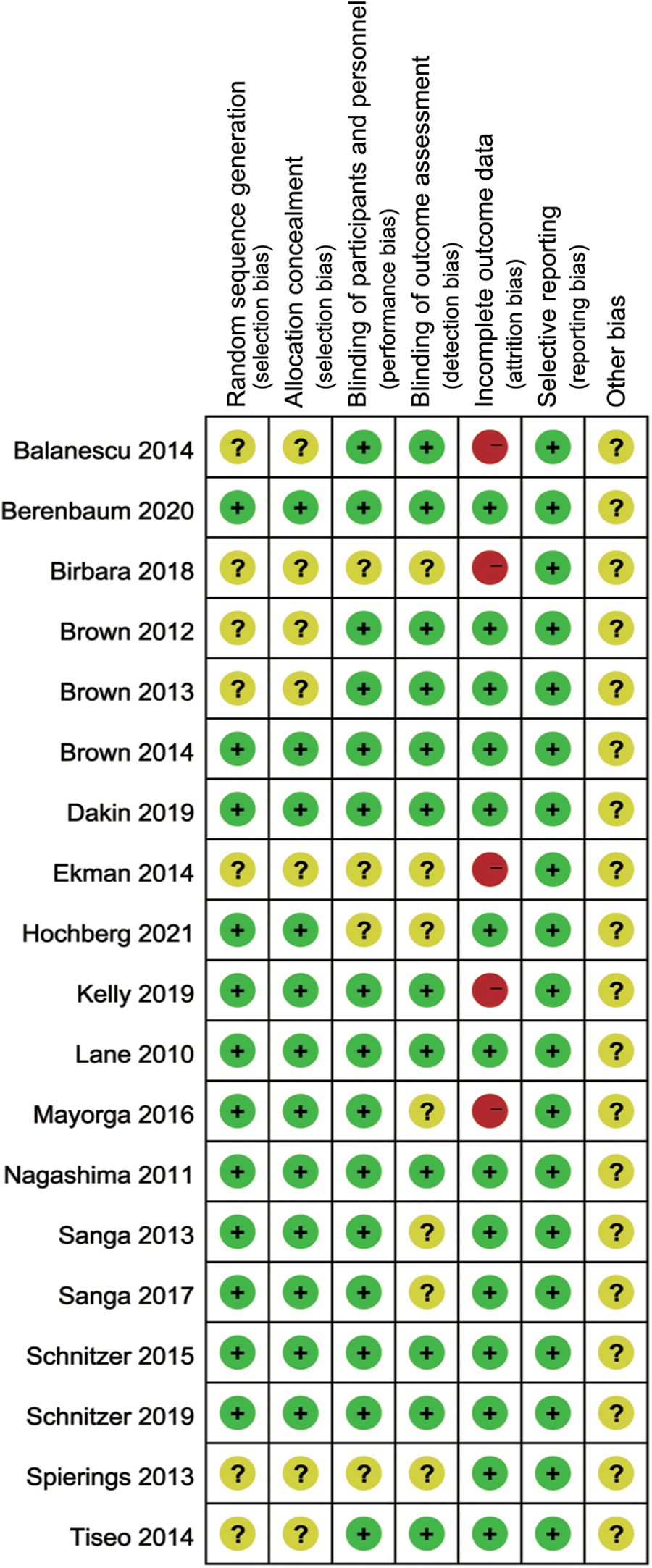
Risk of bias of the included studies. + = low risk; – = high risk; ? = unclear risk.
WOMAC Pain Score
A total of 17 studies ** were assessed to determine anti-NGF antibody treatment effects on WOMAC pain scores (Figure 3). The results demonstrated a significant decrease in pain (SMD, –0.31 [95% CI, –0.36 to –0.26]; Z = 11.75; P < .00001; I 2 = 38%).

Forest plot of changes from baseline to the endpoint for the Western Ontario and McMaster Universities Osteoarthritis Index pain score. DSR, diclofenac sustained release; IV, intravenous; IV, inverse variance; q4wk, once every 4 weeks; q8wk, once every 8 weeks; SC, subcutaneous; Std. Mean Difference, standardized mean difference.
There were 9 studies that reported only intravenous (IV) administration, †† 7 that reported only subcutaneous (SC) administration, 3,10,18,23,27,33,34 and 1 that reported both administration modes. 4 The WOMAC pain score was reported at 8 weeks in 6 studies, 2,4,14,29,40,41 at 16 weeks in 13 studies, ‡‡ and at 24 weeks in 1 study. 3 To directly compare the effects of dose, administration mode and treatment duration combined on the outcome indicators, we divided the RCTs into 14 subgroups. The results are shown in Table 2 and Appendix 2 (Figure A1). The results of the subgroup analysis showed that the IV administration of a high-dose anti-NGF over a period of 16 weeks significantly improved the WOMAC pain score (SMD= −0.42; [95% CI, −0.55 to −0.28]; Z = 5.99; P < .00001; I2 = 55%).
Subgroup Analysis of WOMAC Pain Scores According to Dose, Administration Mode, and Treatment Duration a
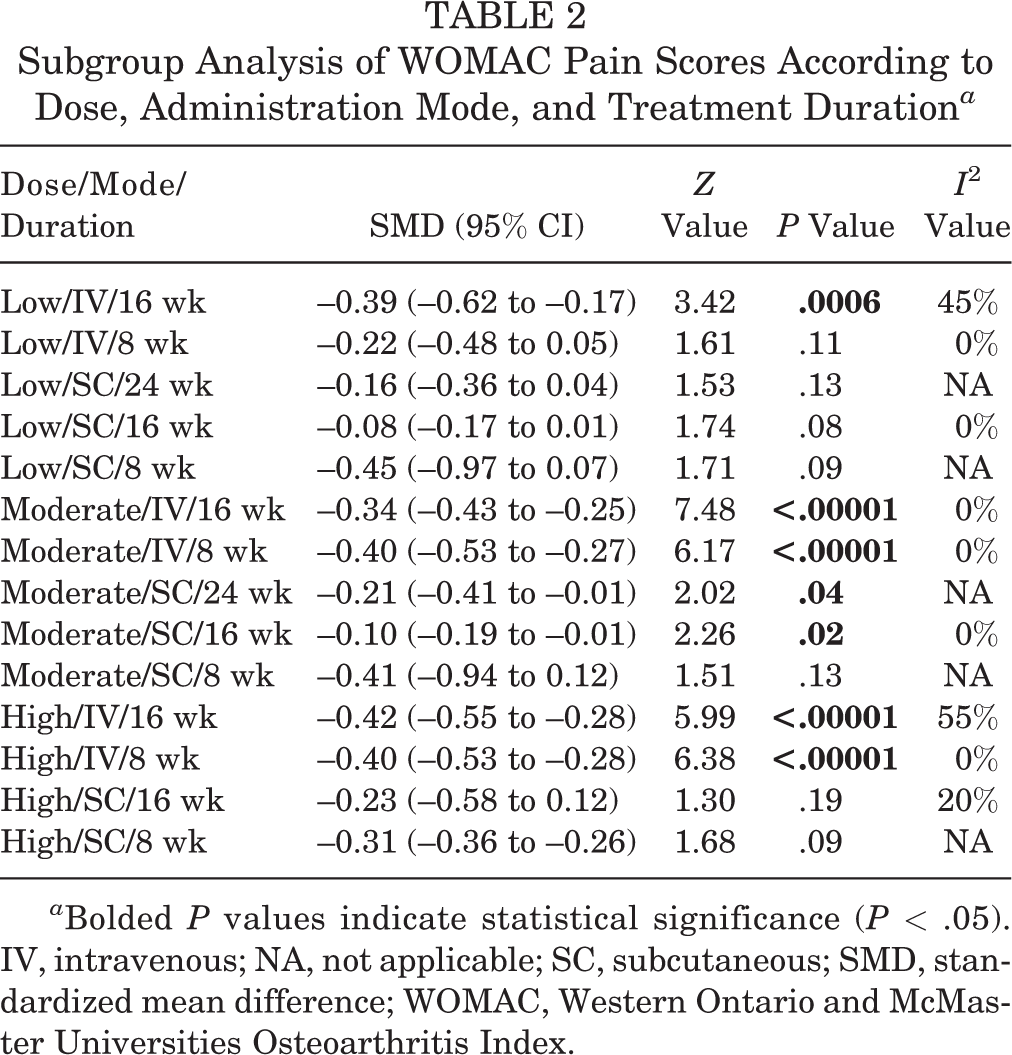
a Bolded P values indicate statistical significance (P < .05). IV, intravenous; NA, not applicable; SC, subcutaneous; SMD, standardized mean difference; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
WOMAC Physical Function Score
A total of 16 studies §§ were assessed to determine anti-NGF antibody treatment effects based on the WOMAC physical function score (Figure 4). The overall physical function score significantly improved (SMD, –0.36 [95% CI, –0.41 to –0.30]; Z = 12.67; P < .00001; I 2 = 44%) (Figure 4).
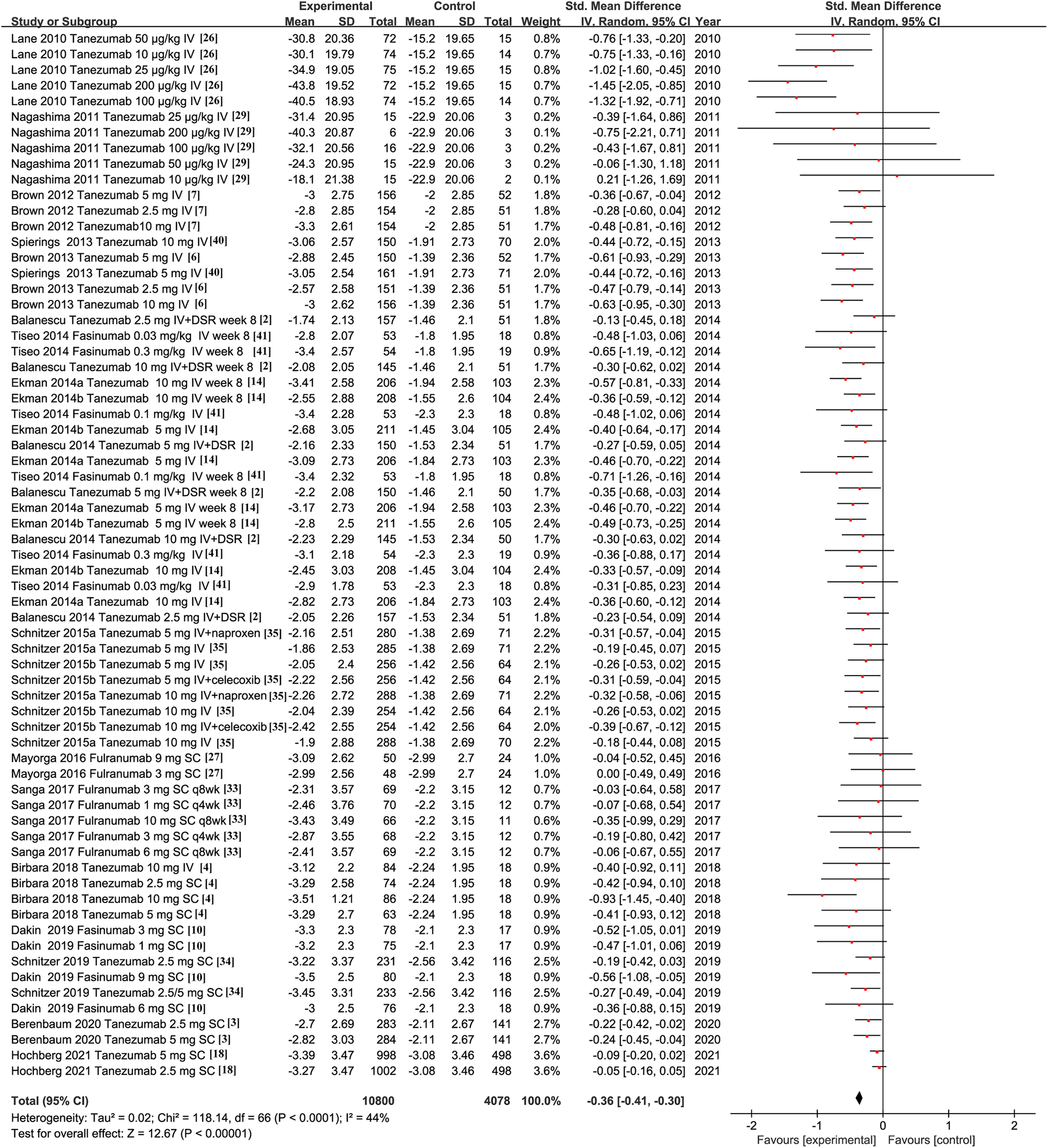
Forest plot of changes from baseline to the endpoint for the Western Ontario and McMaster Universities Osteoarthritis Index physical function score. DSR, diclofenac sustained release; IV, intravenous; IV, inverse variance; q4wk, once every 4 weeks; q8wk, once every 8 weeks; SC, subcutaneous; Std. Mean Difference, standardized mean difference.
There were 9 studies that reported only IV administration ∥∥ 6 that reported only SC administration, 3,10,18,27,33,34 and 1 that reported both modes. 4 The WOMAC physical function score was reported at 8 weeks in 6 studies, 2,4,14,29,40,41 at 16 weeks in 12 studies, ¶¶ and at 24 weeks in 1 study. 3 To directly compare the combined effects of dose, administration mode, and treatment duration on the outcome indicators, we divided the RCTs into 14 subgroups. The results are shown in Table 3 and Appendix 2 (Figure A2). The results of the subgroup analysis showed that IV administration of a moderate dose of anti-NGF antibody treatment over a period of 8 weeks significantly improved the WOMAC physical function score (SMD, –0.46 [95% CI, –0.58 to –0.33]; Z = 7.01; P < .00001; I 2 = 0%).
Subgroup Analysis of WOMAC Physical Function Scores According to Dose, Administration Mode, and Treatment Duration a

a Bolded P values indicate statistical significance (P < .05). IV, intravenous; NA, not applicable; SC, subcutaneous; SMD, standardized mean difference; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
WOMAC Stiffness Score
A total of 4 studies 26,27,29,40 assessed anti-NGF antibody treatment on WOMAC stiffness scores (Figure 5). The overall stiffness score significantly improved (SMD, –3.59 [95% CI, –4.87 to –2.30]; Z = 5.47; P < .00001; I 2 = 98%) (Figure 5).

Forest plot of changes from baseline to the endpoint for the Western Ontario and McMaster Universities Osteoarthritis Index–stiffness score.
PGA Score
A total of 13 studies ## were assessed to determine anti-NGF antibody treatment effects on the PGA score. The overall PGA score significantly improved (SMD, –0.28 [95% CI, –0.34 to –0.22]; Z = 9.39; P < .00001; I 2 = 50%) (Figure 6).

Forest plot of changes from baseline to the endpoint for the patient global assessment score. DSR, diclofenac sustained release; IV, intravenous; IV, inverse variance; q4wk, once every 4 weeks; q8wk, once every 8 weeks; SC, subcutaneous; Std. Mean Difference, standardized mean difference.
There were 7 studies that reported only IV administration, 2,6,7,14,26,35,40 5 that reported only SC administration, 3,18,27,33,34 and 1 that reported both modes. 4 PGA scores were reported at 8 weeks in 4 studies, 2,4,14,40 at 16 weeks in 10 studies, a and at 24 weeks in 1 study. 3 To directly compare the combined effects of dose, administration mode, and treatment duration on the outcome indicators, we divided the RCTs into 14 subgroups. The results are shown in Table 4 and Appendix 2 (Figure A3). The results of the subgroup analysis showed that IV administration of a moderate dose of anti-NGF antibody treatment over a period of 8 weeks significantly improved the PGA score (SMD, –0.45 [95% CI, –0.58 to –0.31]; Z = 6.63; P < .00001; I 2 = 0%).
Subgroup Analysis of PGA Scores According to Dose, Administration Mode, and Treatment Duration a

a Bolded P values indicate statistical significance (P < .05). IV, intravenous; NA, not applicable; SC, subcutaneous; SMD, standardized mean difference.
Adverse Events
AEs were reported in all RCTs. b Nausea, arthralgia, paresthesia, hypoesthesia, and headache were the most frequently reported AEs in the treatment groups. The overall incidence of patients with AEs was higher in the anti-NGF antibody treatment groups than in the control groups. RRs for AEs were significantly increased (RR, 1.09 [95% CI, 1.06-1.12]; Z = 5.60; P < .00001; I 2 = 0%) (Figure 7).
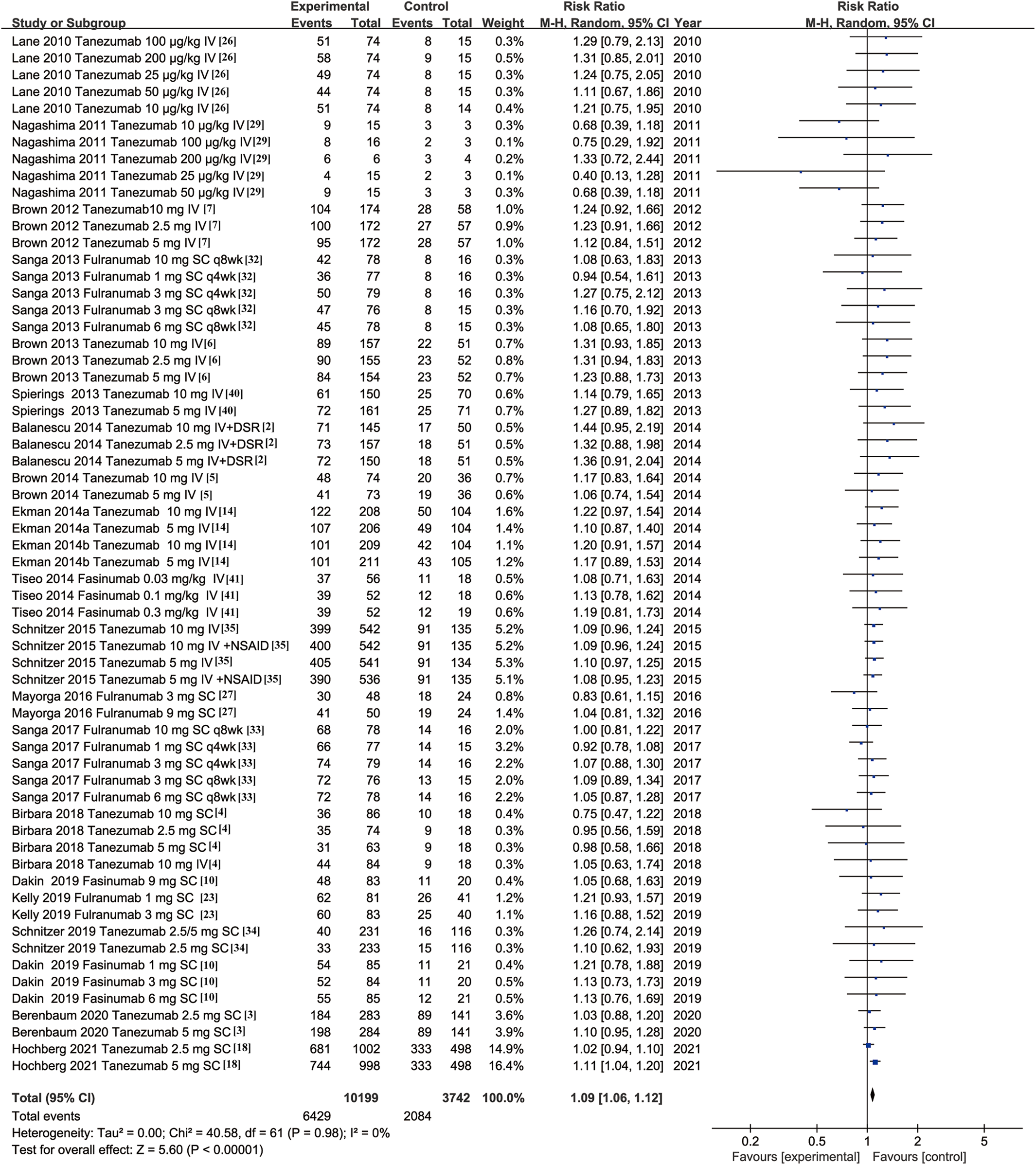
Forest plot of differences in adverse event rates between the experimental and control groups. DSR, diclofenac sustained release; IV, intravenous; M-H, random Mantel-Haenszel random-effects model; q4wk, once every 4 weeks; q8wk, once every 8 weeks; SC, subcutaneous.
There were 10 studies that reported only IV administration, c 8 that reported only SC administration, 3,10,18,23,27,32,33,34 and 1 that reported both modes. 4 To directly compare the combined effects of dose and administration mode on outcome indicators, we divided the RCTs into 6 subgroups. The results are shown in Table 5 and Appendix 2 (Figure A4). The results of the subgroup analysis showed that IV administration of a low dose of anti-NGF antibodies significantly increased the incidence of AEs (RR, 1.28 [95% CI, 1.05-1.55]; Z = 2.44; P = .01; I 2 = 0%).
Subgroup Analysis of Adverse Events According to Dose and Administration Mode a

a Bolded P values indicate statistical significance (P < .05). IV, intravenous; RR, risk ratios; SC, subcutaneous.
Additionally, 17 studies d were assessed to determine anti-NGF antibody treatment effects on SAEs. Increased OA, osteonecrosis, and arthralgia were the most commonly reported SAEs in all treatment groups. Compared with the control groups, the incidence of SAEs in the anti-NGF antibody treatment groups did not increase significantly (RR, 1.15 [95% CI, 0.98-1.34]; Z = 1.71; P = .09; I 2 = 0%) (Figure 8).
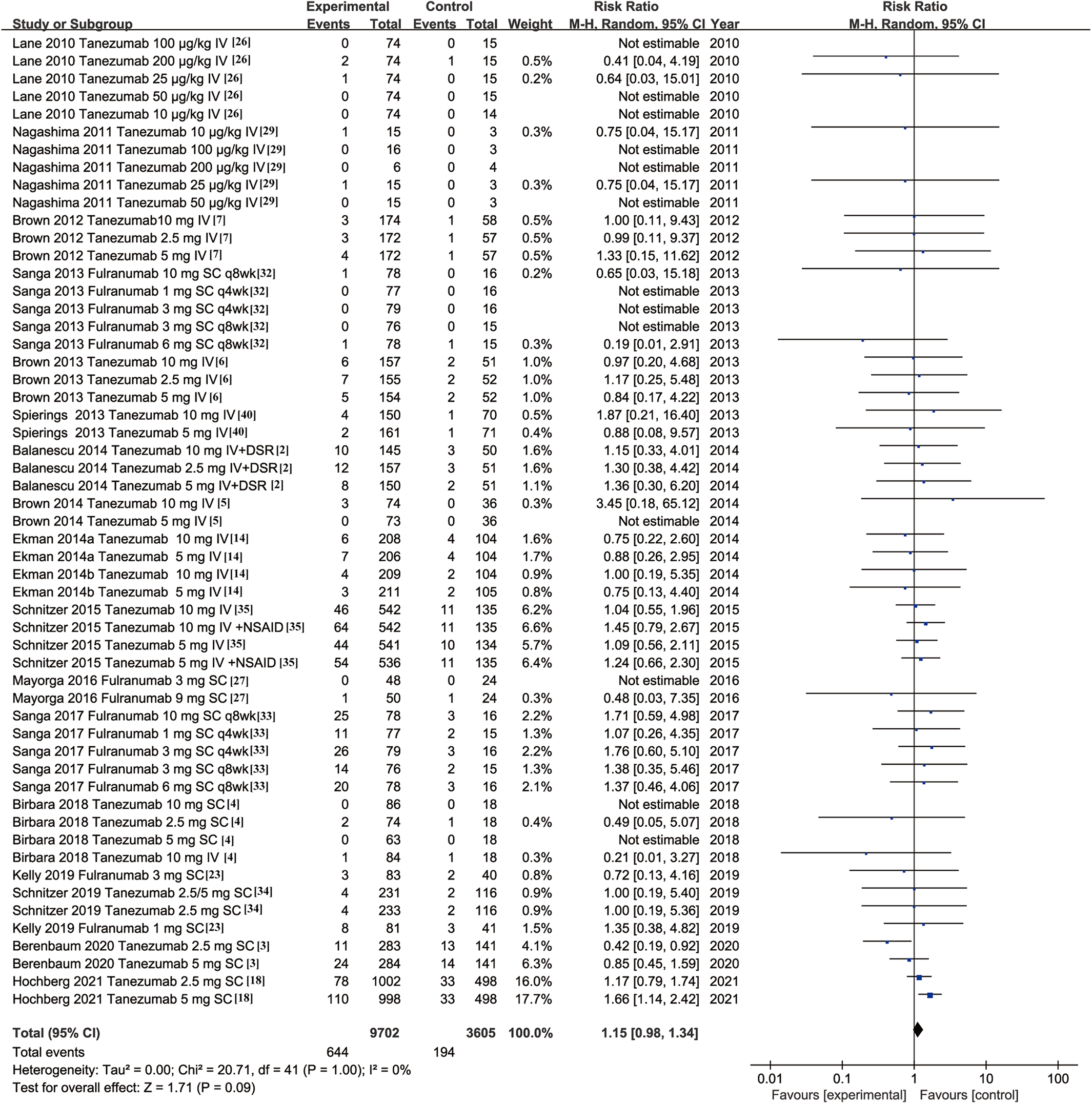
Forest plot of differences in serious adverse event rates between the experimental and control groups.
There were 9 studies that reported only IV administration, 7 that reported only SC administration, and 1 that reported both modes. To directly compare the combined effects of dose and administration mode on the outcome indicators, we divided the RCTs into 6 subgroups. The results are shown in Table 6 and Appendix 2 (Figure A5). The results of the subgroup analysis showed that in all treatment groups, the incidence of SAEs did not significantly increase.
Subgroup Analysis of Serious Adverse Events According to Dose and Administration Mode a

a IV, intravenous; RR, risk ratios; SC, subcutaneous.
Sensitivity Analysis
A sensitivity analysis was performed on 9 RCTs 2 –7,14,18,35 that assessed fixed-dose tanezumab (Table 7 and Appendix 3). The analysis revealed significant improvements in the overall WOMAC pain score (SMD, –0.27 [95% CI, –0.32 to –0.21]; Z = 9.51; P < .001; I 2 = 32%), WOMAC physical function score (SMD, –0.31 [95% CI, –0.37 to –0.25]; Z = 10.12; P < .001; I 2 = 42%), and PGA score (SMD, –0.24 [95% CI, –0.30 to –0.17]; Z = 7.44; P < .001; I 2 = 47%) (Table 7). The proportion of the fixed-dose tanezumab group that discontinued treatment because of AEs was significantly higher than that of the control group (RR, 1.12 [95% CI, 1.08 to 1.15]; Z = 6.15; P < .001; I 2 = 0%). Compared with the control group, the incidence of SAEs in the fixed-dose tanezumab group did not significantly increase (RR, 1.14 [95% CI, 0.97 to 1.34]; Z = 1.55; P = .12; I 2 = 0%).
Sensitivity Analysis of Fixed-Dose Tanezumab a
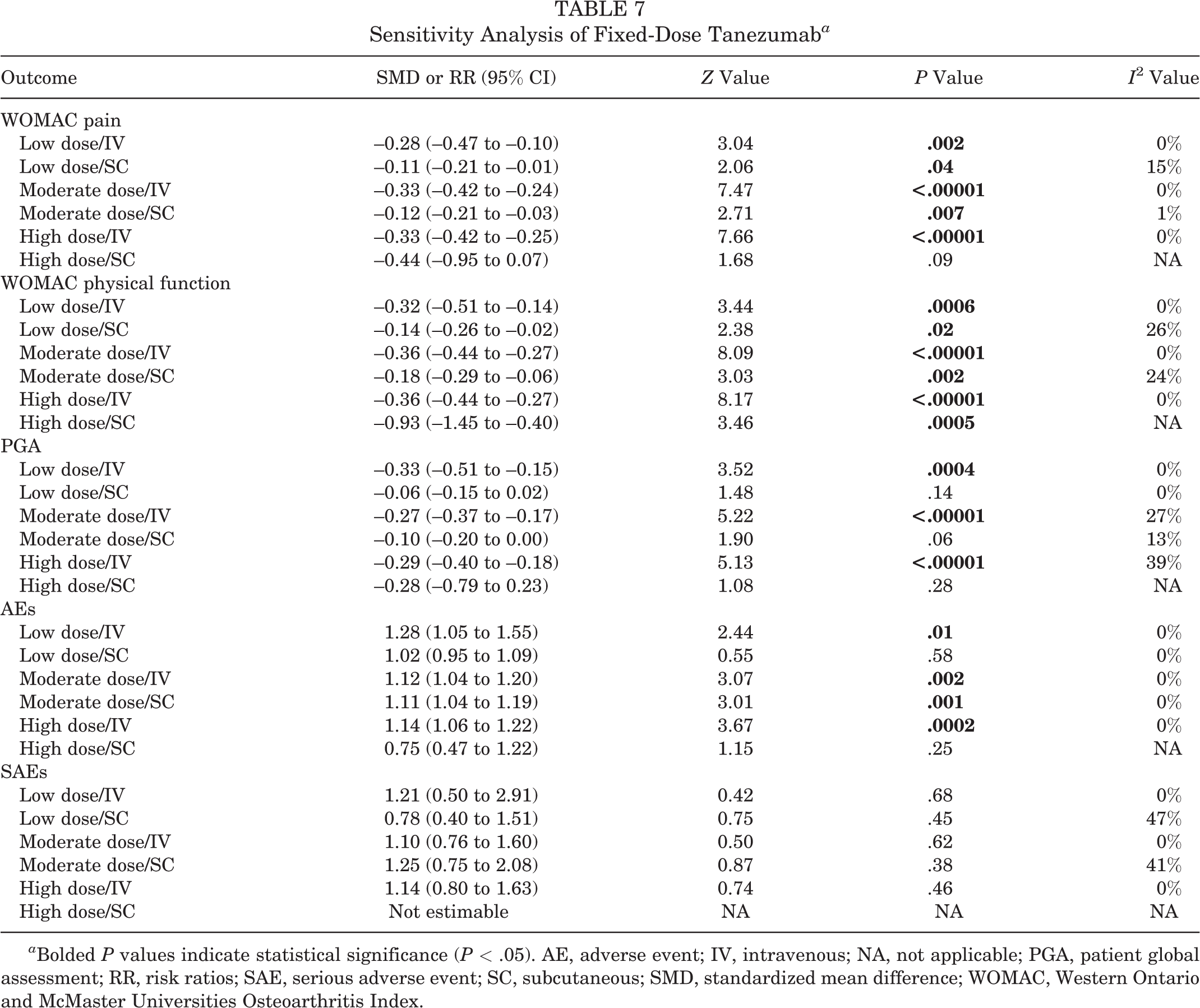
a Bolded P values indicate statistical significance (P < .05). AE, adverse event; IV, intravenous; NA, not applicable; PGA, patient global assessment; RR, risk ratios; SAE, serious adverse event; SC, subcutaneous; SMD, standardized mean difference; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
A sensitivity analysis of 4 RCTs with active comparator drugs was performed (Appendix 4). There were 2 RCTs 27,40 that used controlled-release oxycodone and 2 RCTs 14,18 that used NSAIDs as active comparator drug controls. There were significant improvements in the WOMAC pain score (SMD, –0.21 [95% CI, –0.31 to –0.11]; Z = 3.99; P < .001; I 2 = 54%), WOMAC physical function score (SMD, –0.24 [95% CI, –0.34 to –0.13]; Z = 4.40; P < .001; I 2 = 56%), and PGA score (SMD, –0.20 [95% CI, –0.32 to –0.09]; Z = 3.45; P = .0006; I 2 = 63%). The results of the sensitivity analysis showed that there was no significant difference in the rate of treatment discontinuation due to AEs between the Anti-NGF antibody group and the active comparator drugs group (RR, 0.94 [95% CI, 0.85 to 1.04]; Z = 1.14; P =0.26; I 2 = 73%). Compared to the control group, the incidence of SAEs in the fixed-dose tanezumab group did not significantly increase (RR, 1.20 [95% CI, 0.90 to 1.61]; Z = 1.22; P = .22; I 2 = 9%).
Publication Bias
Asymmetry in the funnel plots indicated a publication bias (Figure 9). The P value from the Egger test 13 was <.001 for the WOMAC pain score, indicating an inflation of SMD values due to publication bias.

Funnel plots with pseudo–95% CIs. Funnel plot of changes from baseline to the endpoint for the Western Ontario and McMaster Universities Osteoarthritis Index–pain score. IV, inverse variance.
Discussion
According to our results, anti-NGF antibody therapy was an effective type of treatment for OA. The pooled results showed a significant reduction in the change in WOMAC pain (SMD, –0.31 [95% CI, –0.36 to –0.26]; Z = 11.75; P < .00001; I 2 = 38%), WOMAC physical function (SMD, –0.36 [95% CI, –0.41 to –0.30]; Z = 12.67; P < .00001; I 2 = 44%), WOMAC stiffness (SMD, –3.59 [95% CI, –4.87 to –2.30]; Z = 5.47; P < .00001; I 2 = 98%), and PGA scores (SMD, –0.28 [95% CI, –0.34 to –0.22]; Z = 9.39; P < .00001; I 2 = 50%). In contrast to good treatment effects, the incidence of AEs also increased (RR, 1.09 [95% CI, 1.06 to 1.12]; Z = 5.60; P < .00001; I 2 = 0%).
There have been reports on the use of the anti-NGF antibodies tanezumab, fulranumab, and fasinumab to treat hip and/or knee OA pain. 10,18,33 However, there is still controversy over the effectiveness and safety of this treatment. The optimal dose, administration mode, and treatment duration of each drug have not been determined for this therapy in a clinical setting.
The therapeutic effects and safety of anti-NGF antibody treatment from 19 RCTs were assessed for hip and knee OA pain. Pooled results showed significant reductions in WOMAC scores for pain, physical function, and stiffness as well as in PGA scores. These changes show the clinical significance of anti-NGF antibody treatment for hip and/or knee OA. The results are consistent with previous RCTs indicating that anti-NGF antibody drugs have a significant effect on pain relief and functional improvement in patients with hip and/or knee OA pain. 18,35 It may be that NGF plays a key role in the process of pain generation under chronic pain conditions. 39,42 Anti-NGF antibodies have the potential to normalize noxious hyperactivity and produce pain relief in a clinical environment. 42 These drugs may reduce the concentration of free NGF, prevent NGF from binding to TrkA, or prevent TrkA from being activated and thus play a role in pain treatment. 12,24 Our meta-analysis showed that the incidence of AEs in the treatment group was higher than that in the control group, but the incidence of SAEs was similar between the 2 groups.
We believe that the overall research quality was high. Most of the RCTs in this study were low risk in terms of random sequence generation, allocation of hidden information, blinding, and selective reporting. However, there were 5 high-risk studies in terms of the completeness of the results. 2,4,14,23,27 All the studies were sponsored by pharmaceutical companies, which could have an effect on the findings. Our results indicate that a large number of unpublished studies and studies reporting nonsignificant results have led to publication bias.
High doses of anti-NGF antibodies improve OA pain but increase the incidence of AEs. Our meta-analysis focused on the effect of dose, administration mode, and treatment duration on the treatment of OA pain. Our subgroup analysis of the effects of the 3 combined variables showed that there was no unique treatment that achieved an optimal therapeutic effect. High doses of anti-NGF antibodies via IV administration over a 16-week treatment period significantly improved pain scores. Moderate doses of anti-NGF antibodies via IV administration over an 8-week treatment period significantly improved physical function scores. Low doses of anti-NGF antibodies via IV administration over a 16-week treatment period significantly improved PGA scores. In general, the IV administration of anti-NGF antibodies was a more effective treatment method compared to SC administration. Low doses of anti-NGF antibodies had the highest incidence of AEs using IV administration. Moderate doses of anti-NGF antibodies had the lowest incidence of AEs using SC administration. The incidence of AEs in all treatment groups was higher than that in the control groups. An indirect comparison of the incidence of AEs in subgroup analyses showed that the incidence of AEs with SC administration was lower than that of the corresponding dose with IV administration. In all treatment groups, the incidence of SAEs was similar to that in the control groups. This finding is consistent with the results of the direct comparison between the IV and SC administrations of tanezumab. 4
RCTs that assessed the SC administration of tanezumab as a new treatment method 4,18,33 allowed us to conduct a sensitivity analysis on fixed doses of tanezumab. Results of the analysis showed that tanezumab effectively relieved pain, improved physical function and stiffness, and improved PGA scores. Birbara et al 4 examined the effects of the IV versus SC administration of tanezumab for the treatment of OA pain. Their results showed that there was no significant difference in the effectiveness of the 2 administration modes. Our sensitivity analysis showed that medium- and high-dose tanezumab had the most significant improvement in pain with IV administration. High doses of tanezumab had the most significant improvement in physical function with SC administration, and high doses of tanezumab had the most significant improvement in PGA scores with IV administration. Although our results are consistent with the observation that a higher dose of tanezumab provides improved efficacy, 38 our findings of the effectiveness of IV administration on treatment outcomes differ from the results of Birbara et al. 4 Considering that only one study used a high dose of tanezumab (10 mg) with SC administration, 4 we believe that additional studies comparing different administration modes should be performed.
Our sensitivity analysis demonstrated that compared with oxycodone, 27,40 and NSAIDs, 14,18 anti-NGF antibodies significantly improved pain scores, physical function scores, and PGA scores. There was no significant difference in the incidence of AEs for anti-NGF antibodies compared to analgesics. 14,18,27,40
The safety of anti-NGF antibodies has been a concern in clinical applications. 17 Our meta-analysis showed that the frequency of drug withdrawal because of AEs in the treatment group was higher than that in the control group and that the incidence of SAEs was similar between the 2 groups. In multiple studies, a lower incidence of AEs in the placebo group or placebo combined with NSAID group compared to the anti-NGF antibody group or anti-NGF antibody combined with NSAID group was reported. 2,35 Several studies reported that the frequency of treatment discontinuation because of AEs with anti-NGF antibodies is similar to or lower than the rates observed with NSAIDs. 14,27,35,40 Our safety data showed that the incidence of drug withdrawal because of AEs and SAEs meets the prescribed standards. 14,27,35,40 We found that anti-NGF antibody treatments are well tolerated and safe.
The most common AEs associated with the use of anti-NGF antibodies include peripheral edema, joint and limb pain, and peripheral neuropathy. 12,33,35,41 Less than 10% of patients have neuropathy. 12 Symptoms of abnormal peripheral sensation are usually mild to moderate, transient in nature, and without continuous changes on neurological examination, and most AEs disappeared before the end of the study by Dietz et al. 12
Early clinical trial studies have shown that rapidly progressive OA is a potential SAE. 3,17,35 The United States Food and Drug Administration concluded that tanezumab was unrelated to an increased risk of osteonecrosis. 19,36 Schnitzer et al 34,35 showed that joint safety events were rare and most were considered normal OA progression. No joint safety event was judged to be osteonecrosis, a subchondral insufficiency fracture, or a pathological fracture. 35 The incidence of rapidly progressive OA may be related to the dose of tanezumab. 34 SAEs in clinical trials of anti-NGF antibodies should be monitored to determine the overall risk-benefit ratio of anti-NGF antibodies in controlling OA pain.
We found that anti-NGF antibodies provided pain relief and improved physical function in patients with OA as well as had acceptable AEs. Compared with classic OA analgesics (oxycodone and NSAIDs), anti-NGF antibodies improved treatment outcomes better. There were significant improvements in the WOMAC pain score (SMD, −0.21 [95% CI, −0.31 to −0.11]; Z = 3.99; P < .001; I 2 = 54%), WOMAC physical function score (SMD, −0.24 [95% CI, −0.34 to −0.13]; Z = 4.40; P < .001; I 2 = 56%), and PGA score (SMD, −0.20 [95% CI, −0.32 to −0.09]; Z = 3.45; P = .0006; I 2 = 63%). Our results may provide an important foundation for investigating anti-NGF antibody treatment policies.
This meta-analysis had several limitations. First, few RCTs examining fulranumab and fasinumab were available, which may have affected outcomes. Second, RCTs did not distinguish between knee and hip outcomes. Third, most of the RCTs that we included only reported the outcome indicators at 16 weeks, and more outcome indicators at different treatment durations are needed to increase the reliability of the results. Fourth, there was only 1 study that directly compared the IV and SC administrations of tanezumab. Fifth, the WOMAC stiffness scores were highly heterogeneous (I 2 = 98%), and few RCTs reported on this outcome indicator. Finally, all RCTs were sponsored by pharmaceutical companies, possibly introducing funding bias.
Conclusion
Our meta-analysis showed that anti-NGF antibodies could effectively relieve pain, improve physical function, reduce stiffness, and improve the PGA score in patients with knee and hip OA. We found that the AEs caused by anti-NGF antibody treatment were temporary and mild in nature and were usually well tolerated. SAEs were not considered to be related to the use of anti-NGF antibodies. However, no conclusion can be drawn regarding the optimal treatment plan for anti-NGF antibodies based on an analysis of the combined effect of the study variables on treatment outcomes. Additional RCTs are necessary to provide information on the combined effect of dose, administration mode, and treatment duration on the effectiveness and safety of anti-NGF antibody treatment.
Footnotes
Acknowledgment
Final revision submitted November 23, 2021; accepted January 10, 2022.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Approval statement
All studies included in this meta-analysis had been published and declared ethical approval, and we did not collect or utilize any raw data of these results, therefore no ethical approval was needed for this meta-analysis study. This meta-analysis was conducted on the basis of the Preferred Reporting Items for Systematic Reviews and Meta-analysis.
Appendix 1

| Search Strategy | Results | |
|---|---|---|
|
|
||
| #1 | "Osteoarthritis"[Mesh] | 65487 |
| #2 | Osteoarthr* | 101226 |
| #3 | OA[Title/Abstract] | 37442 |
| #4 | "Degenerative Arthriti*" | 1410 |
| #5 | Arthroses [Title/Abstract] | 512 |
| #6 | Arthrosis [Title/Abstract] | 5511 |
| #7 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 ((("Nerve Growth Factor"[Mesh]) OR "fasimimab" | 118192 |
| #8 | [Supplementary Concept]) OR "fulranumab" [Supplementary Concept]) OR "tanezumab" [Supplementary Concept] | 7347 |
| #9 | "nerve growth factor"[Title/Abstract] | 18874 |
| #10 | NGF[Title/Abstract] | 15932 |
| #11 | fasinumab[Title/Abstract] | 19 |
| #12 | REGN475[Title/Abstract] | 3 |
| #13 | fulranumab[Title/Abstract] | 19 |
| #14 | tanezumab [Title/Abstract] | 105 |
| #15 | RN624 MAb[Title/Abstract] | 6 |
| #16 | RN624[Title/Abstract] | 2 |
| #17 | RI 624[Title/Abstract] | 123 |
| #18 | #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 | 23396 |
| #19 | #7 AND #18 | 286 |
| #20 | (randomized controlled trial[pt] OR controlled clinical trial[pt]OR randomized[tiab] OR placebo[tiab] OR clinical trials as topic[mesh:noexp] OR randomly[tiab] OR trial[ti]) NOT (animals [mh] NOT (humans [mh] AND animals[mh])) |
1254914 |
| #21 | #19 AND #20 | 66 |
|
|
||
| #1 | MeSH descriptor: [Osteoarthritis] explode all trees | 7704 |
| #2 | (osteoarthr*) | 19224 |
| #3 | (OA): ti,ab,kw | 6306 |
| #4 | "Degenerative Arthriti*" | 1 |
| #5 | (Arthrosis): ti,ab,kw | 652 |
| #6 | (Arthroses): ti,ab,kw | 40 |
| #7 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 | 20285 |
| #8 | MeSH descriptor: [Nerve Growth Factor] explode all trees | 87 |
| #9 | (NGF): ti,ab,kw OR ("nerve growth factor"):ti,ab,kw | 512 |
| #10 | (SAR164877):ti,ab,kw | 6 |
| #11 | (REGN475): ti,ab,kw | 19 |
| #12 | (fasinumab): ti,ab,kw | 22 |
| #13 | #10 OR #11 OR #12 | 30 |
| #14 | (fulranumab): ti,ab,kw | 23 |
| #15 | (JNJ 42160443): ti,ab,kw | 16 |
| #16 | #14 OR #15 | 35 |
| #17 | (tanezumab): ti,ab,kw | 117 |
| #18 | (RN624): ti,ab,kw | 15 |
| #19 | (RI 624): ti,ab,kw | 3 |
| #20 | (PF 04383119): ti,ab,kw | 13 |
| #21 | #17 OR #18 OR #19 OR #20 | 126 |
| #22 | #8 OR #9 OR #13 OR #16 OR #21 | 642 |
| #23 | #7 AND #22 | 134 |
|
|
||
| #1 | osteoarthritis’/exp | 139060 |
| #2 | oa:ab,ti | 58777 |
| #3 | ‘degenerative arthriti*’ | 1751 |
| #4 | osteoarthr* | 163396 |
| #5 | arthroses:ab,ti | 600 |
| #6 | arthrosis:ab,ti | 7481 |
| #7 | nerve growth factor’/exp | 27373 |
| #8 | nerve growth factor antibody’/exp | 615 |
| #9 | #7 OR #8 | 27611 |
| #10 | ‘fasinumab’/exp | 66 |
| #11 | ‘fulranumab’/exp | 84 |
| #12 | ‘tanezumab’/exp | 409 |
| #13 | ngf:ab,ti | 19411 |
| #14 | ‘nerve growth factor’:ab,ti | 21860 |
| #15 | fasinumab:ab,ti | 22 |
| #16 | fulranumab:ab,ti | 37 |
| #17 | tanezumab:ab,ti | 202 |
| #18 | regn475: ab,ti | 5 |
| #19 | sar164877: ab,ti | 1 |
| #20 | jnj 42160443’: ab,ti | 3 |
| #21 | rn624: ab,ti | 2 |
| #22 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 | 192383 |
| #23 | #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR # 19 OR #20 OR #21 | 35541 |
| #24 | #22 AND #23 ‘crossover procedure’:de OR ‘double-blind procedure’:de OR ‘randomized controlled trial’:de OR ‘single-blind procedure’:de OR random*:de,ab,ti OR factorial*:de,ab,ti OR |
697 |
| #25 | crossover*:de,ab,ti OR ((cross NEXT/1 over*):de,ab,ti) OR placebo*:de,ab,ti OR ((doubl* NEAR/1 blind*):de,ab,ti) OR ((singl* NEAR/1 blind*):de,ab,ti) OR assign*:de,ab,ti OR allocat*:de,ab,ti OR volunteer*:de,ab,ti | 2715860 |
| #26 | #24 AND #25 | 241 |
|
|
||
| #1 | TOPIC: (Osteoarthr*) | 82281 |
| #2 | TOPIC: (OA) | 36559 |
| #3 | TOPIC: ("Degenerative Arthriti*") | 726 |
| #4 | TOPIC: (Arthrosis) | 1975 |
| #5 | TOPIC: ("nerve growth factor") | 100295 |
| #6 | TOPIC: ("nerve growth factor") | 16664 |
| #7 | TOPIC: (NGF) | 9626 |
| #8 | TOPIC: (fasinumab) | 19 |
| #9 | TOPIC: (fulranumab) | 29 |
| #10 | TOPIC: (tanezumab) | 222 |
| #11 | TOPIC: (REGN475) | 3 |
| #12 | TOPIC: (RN624) | 2 |
| #13 | TOPIC: (RN 624) | 3 |
| #14 | #12 OR #13 | 5 |
| #15 | TOPIC: (RI 624) | 9 |
| #16 | TOPIC: (PF-04383119) | 1 |
| #17 | #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #14 OR #15 OR #16 |
19129 |
| #18 | #5 AND #17 TS= clinical trial* OR TS=research design OR TS=comparative stud* OR TS=evaluation stud* OR TS=controlled trial* OR |
419 |
| #19 | TS=follow-up stud* OR TS=prospective stud* OR TS=random* OR TS=placebo* OR TS= (single blind*) OR TS= (double blind*) |
3398291 |
| #20 | #18 AND #19 | 182 |