
Abstract
Objective
To evaluate the effect of parecoxib on preventing postoperative shivering.
Methods
Main outcomes were the relative risk (odds ratio, OR) and 95% confidence interval (CI) relative to the incidence of shivering.
Results
Fourteen trials with 1,175 patients were analyzed. The pooled evidence suggested that parecoxib sodium, given before anesthesia or postoperatively (only 4 cases), had the potential to prevent postoperative shivering (OR = 0.21, 95% CI, 0.16, 0.29). Compared with the placebo, parecoxib sodium significantly lowered the incidence of postoperative shivering as follows: mild shivering [OR = 0.51, 95% CI (0.35, 0.74)]; moderate shivering [OR = 0.28, 95% CI (0.18, 0.45)]; severe shivering [OR = 0.18, 95% CI (0.10, 0.33)]. Compared with placebo, there was no significant association of parecoxib sodium with restlessness [OR = 0.95, 95% CI (0.59, 1.52)] or nausea/vomiting [OR = 0.24, 95% CI (0.09, 0.66)]. In addition, pethidine rescue was used significantly more often in the control group than in the parecoxib sodium group [OR = 0.22, 95% CI (0.09, 0.53)].
Conclusions
Parecoxib sodium may be an effective strategy for preventing postoperative shivering.
Background
Postoperative shivering is common. At least 10%, and as many as 66%, of surgical patients shiver during the course of recovery. 1 Shivering is defined as irregular, spontaneous, continuous constriction of muscle activities for >15 min. It is a physiological response that can increase the metabolic rate and maintain normal body temperature to ensure the continuation of physiological functions. 2 Shivering, however, may incur severe adverse effects, such as increasing oxygen consumption and burdening cardiopulmonary function. 2 It can also elevate intracranial and intraocular pressures and increase the risk of myocardial ischemia. 2 Thus, shivering is a common complication, causing patient severe pain and discomfort. It could have an adverse effect on patients’ physiology and psychology and even influence the postoperative prognosis. 2 In addition, it could also cause the patient to interfere with the wound, causing worse pain, and to interrupt monitoring equipment. 1
Burned patients are more likely to shiver. The mechanism of perioperative shivering is unclear, but shivering after being burned may be due primarily to hypothermia, 3 a common complication of severe burns. The lack of the skin’s protection and the high metabolite rate in burned patients can lower body temperature by disrupting the evaporation and convection that takes place on skin. 3 Increased heat loss from the skin and body surfaces increases the risk of lowering the core body temperature.
Multimodal pain therapy has been used recently to address postoperative pain. It involves the use of non-opioid analgesics, opioids, and co-analgesics. 4 Opioids are frequently used to treat preoperative and postoperative pain, although with many severe adverse effects. In contrast, non-opioids, such as nonsteroidal anti-inflammatory drugs (NSAIDs), can be administered to reduce postoperative pain, with opioid doses given as an adjuvant. 4 Parecoxib, the first cyclooxygenase-2 (COX-2)-selective agent, can be administered intravenously or intramuscularly, providing an advantage for patients experiencing postoperative nausea and vomiting. 4 Unlike opioids, it does not influence platelet aggregation or lead to gastrointestinal ulceration. Its few severe side effects include respiratory depression and excessive sedation. 4
Prostaglandin E2 (PGE2), which plays a key role in thermoregulatory pathways, has been shown to affect body temperature and shivering in animal models. It has also been reported that overexpression of COX-2 in the mouse brain intensified the febrile response. 1 Thus, parecoxib, being a selective COX-2 inhibitor, may affect perioperative thermoregulation by allowing the body to avoid a shivering response. The mechanism of shivering is unclear. Shivering after general anesthesia may be influenced by low body temperature, although pain and uncomfortable sensations may also be related to postoperative shivering. 1 Parecoxib transforms into valdecoxib immediately after intramuscular injection, which releases its precise, powerful analgesic effects. 1 Hence, shivering prevention by parecoxib may be related to its analgesic effects.
Methods
Search strategy and trials selection
The randomized controlled trials included in this analysis were sought from the following databases: PubMed, Ovid, EMBASE, Cochrane Central Register of Controlled Trials, China National Knowledge Infrastructure Database (CNKI), Google Scholar, and Web of Science (January 1985 to October 2016). The following search terms were included in the search: “parecoxib”, “parecoxib sodium”, or “selective cyclooxygenase-2 inhibitor”, and “shiver”. References of selected studies were reviewed for additional trials. Publication languages were not limited.
Inclusion and exclusion criteria
Inclusion criteria for this meta-analysis were as follows: (1) the comparison was between parecoxib and placebo or other drugs in regard to shivering after neuraxial anesthesia and general anesthesia; (2) the research objects were humans of any sex and age; (3) there were no restrictions on dosing regimens or the route of administration of parecoxib; (4) the available outcome data were provided; (5) the experimental group was given parecoxib, and the controlled group was given saline; (6) the experimental group was given parecoxib by intravenous injection before anesthesia.
The exclusion criteria were as follows: (1) reports were abstracts, duplicate publications, reviews; (2) they did not report specific results of the comparison between parecoxib and placebo.
Data extraction and quality assessment
Two reviewers independently extracted data from the included studies. We tabulated the studies and systematically assessed them for homogeneity. If any heterogeneity between the studies did not have justified pooling of the assessed outcome parameters, it was settled by discussion with a third review author. The two reviewers solved any disagreement on included studies, quality assessment, data extraction, and outcome parameters through discussion until total agreement was conceded. They recorded each study’s authors, publication year, number of patients, intervention measures, age and sex of the patients, number of withdrawals, outcome parameters, study methodology, and anesthetic type onto a customized data extraction form described in the Cochrane Handbook for Systematic Reviews of Interventions. If necessary, we contacted the corresponding authors for further information.
The group allocation was concealed by using a random number generator. The results were placed in consecutively sealed numbered envelopes by a third party not involved in the trial. Two authors and a third author independently assessed the risk of bias for each research according to the four items of the Oxford scale, which include the reporting and adequacy of randomization (0–2 points), allocation concealment (0–1 point), double blinding (0–2 points), and description of dropouts (0–2 points). The items were then summed, with the summary scores varying from 0 to 7.
Statistical analysis
The Cochrane Collaboration’s statistical software (RevMan 5.0) was used to assess the quantitative data during the statistical analysis. Classification results were assessed with the odds ratio (OR) and 95% confidence interval (CI). For continuous outcome data, the weighted mean difference or standardized mean difference was estimated by means and standard deviations. For dichotomous outcomes, the Peto OR was estimated. The Cochran Q-Statistics
Results
We found 1274 potential studies from the databases. The detailed screening flow is shown in Figure 1. After screening the titles and abstracts and after full-text screening, 14 studies were selected from our database (Figure 1). The detailed characteristics of 14 articles5–18 in this meta-analysis are shown in Table 1.
Flow chart. Characteristics of the 14 studies included in this meta-analysis.
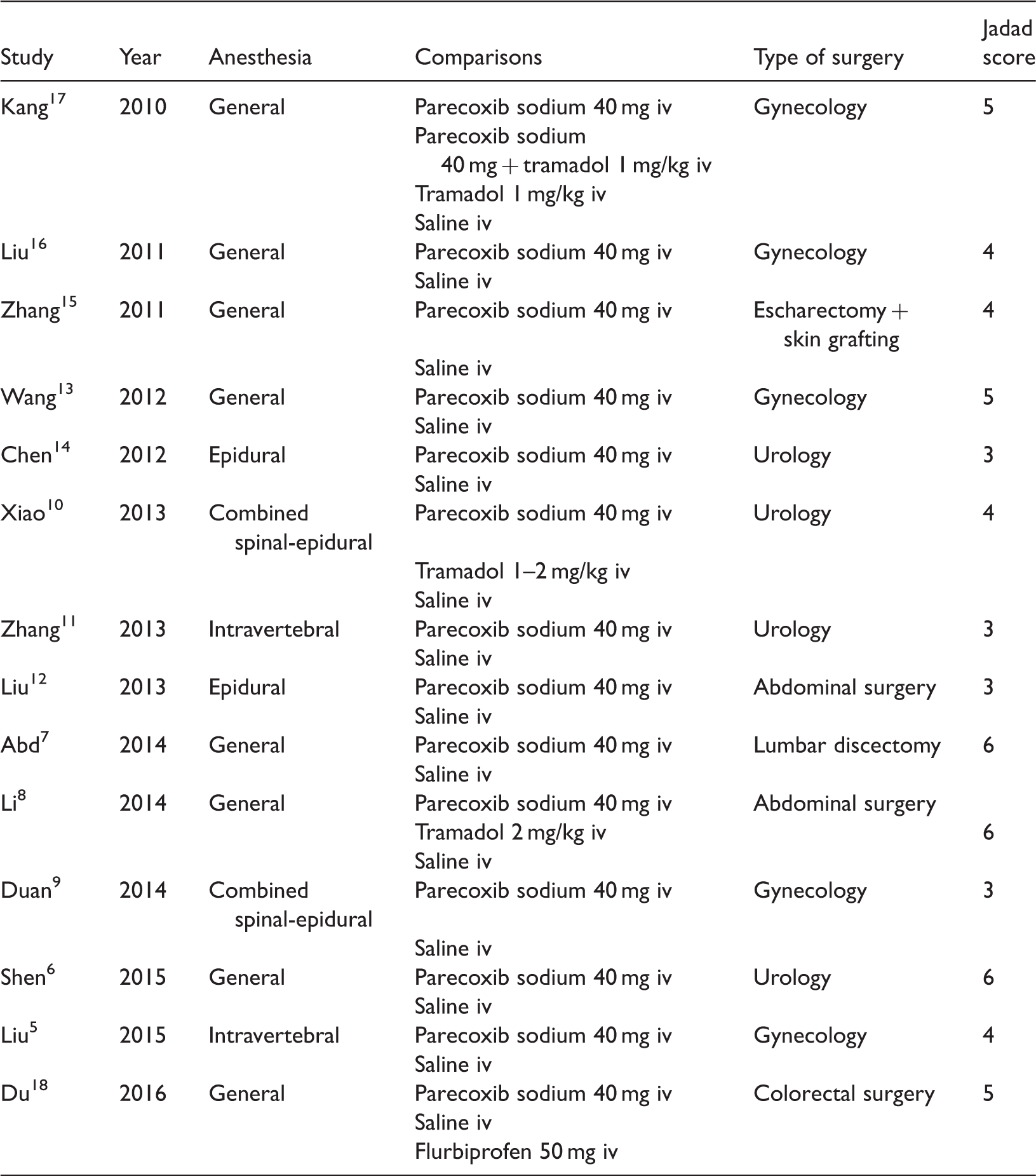
In all, 1175 patients were involved in the 14 included trials. Among them, 602 were given parecoxib sodium, 573 a placebo, and 90 tramadol. The parecoxib sodium dose, which was 40 mg in each case, was given to almost all the subjects before anesthesia. Only four patients received it at the end of the surgery.
The pooled evidence suggested that parecoxib sodium had the potential to prevent postoperative shivering (OR = 0.21, 95% CI, 0.16, 0.29) (Figure 2). No heterogeneity (P = 0.47, I2 = 0%) was found.
Pooled evidence from 14 trials of post-anesthesia shivering: parecoxib sodium versus placebo.
Effect of prophylactic parecoxib on the incidence of shivering, restlessness, PONV, and need for pethidine rescue.

OR, odds ratio; CI, confidence interval; PONV, postoperative nausea and vomiting
In all RCTs (n = 1175 patients), all patients reported on the presence of moderate shivering. As no statistical heterogeneity (P = 0.97, I2 = 0%) was found among the studies, a fixed-effects model was employed for the meta-analysis. The results showed that there was a distinctive difference [OR = 0.28 ,95% CI (0.18, 0.45), P < 0.00001] between the parecoxib sodium group and the controls regarding the incidence of moderate shivering (Table 2).
In all RCTs (n = 1175 patients), all patients reported on the presence of severe shivering. As no statistical heterogeneity (P = 1.00, I2 = 0%) was found among the studies, a fixed-effects model was employed for the meta-analysis. The results showed that there was a distinctive difference [OR = 0.18, 95% CI (0.10, 0.33), P < 0.00001] between the parecoxib sodium group and the controls regarding the incidence of severe shivering (Table 2).
The appearance of adverse reactions in regard to the use of parecoxib sodium versus tramadol was analyzed with a limited test power. Compared with placebo, there was no significant association of parecoxib sodium with avoidance of nausea/vomiting [OR = 0.95, 95% CI (0.59, 1.52), P = 0.83] Table 2 or restlessness [OR = 0.24 , 95% CI (0.09, 0.66), P = 0.006] (Table 2). Compared with placebo, however, the results showed that there were distinctive differences [OR = 0.22, 95% CI (0.09, 0.53), P < 0.0009] between the parecoxib sodium group and the controls regarding the number of patients who required pethidine rescue (Table 2).
Discussion and conclusion
Based on our results, paracoxib sodium decreased the incidence of post-operative shivering. In addition, compared with the placebo group, there was no significant association of parecoxib sodium with alleviation of restlessness or nausea/vomiting. In contrast, however, significantly more patients in the control group required pethidine rescue than did those in the parecoxib sodium group.
This meta-analysis suggested that paracoxib is significantly effective in reducing postoperative shivering with fewer side effects (e.g., sedation, nausea/vomiting). Studies of prophylactic use of paracoxib have been reported.19,20 A feasible mechanism for the effect of paracoxib on shivering may be its inhibition of COX-2 and the synthesis of prostagladins. COX-2 and PGE2 play important roles in the hypothalamus in regard to mediating fever. 21 Thus, COX-2 specific inhibitors could lower the threshold of the thermoregulatory system located in the anterior hypothalamus. Accordingly, paracoxib, a COX-2 inhibitor, may affect perioperative thermoregulation and shivering.
There have been no previously reported studies of prophylactic administration of paracoxib to prevent shivering in burned patients. It is reported that, other than skin, the lungs, liver, and intestines are affected by inflammation after a burn. 22 In the context of the gut, burn injuries may cause mesenteric vasoconstriction and induce hypoxia. 23 Studies have shown that paracoxib exhibits gastroprotective effectiveness with low cardiovascular risk. 24 Burn injuries give rise to the release of pro-inflammatory mediators, which cause local and systematic inflammation. Secondary to systematic inflammatory, severe burns may cause serious adverse reactions, such as multiple organ dysfunction, especially of the lung, the first organ to fail. 25 It has been suggested that inhibition of COX-2 decreases acute lung injury and inhibits PGE2 found in the plasma of seriously burned patients, which can significantly increase immune system dysfunction after a burn injury. 26
The potential limitations of this study should be taken into consideration. First, the small sample size may influence the results to some degree. Second, many of the included studies did not include information on simultaneous adverse reactions with their presentation data.
Footnotes
Acknowledgement
The authors are grateful to You-Jing Luo, MD for her extensive support throughout the article's process. Her contribution substantially improved the quality of the manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.