
Abstract
Background:
Both knotted and knotless single-anchor repair techniques are used to repair transmural ruptures of the upper subscapularis (SSC) tendon. However, it is still unclear which technique provides better clinical and radiological results.
Purpose/Hypothesis:
To compare the clinical and magnetic resonance imaging (MRI) outcomes of knotless and knotted single-anchor repair techniques in patients with a transmural rupture of the upper SSC tendon at 2-year follow-up. It was hypothesized that the 2 techniques would not differ significantly in outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Forty patients with a transmural tear of the upper SSC tendon (grade 2 or 3 according to Fox and Romeo) were retrospectively enrolled. Depending on the repair technique, patients were assigned to either the knotless single-anchor or knotted single-anchor group. After a mean follow-up of 2.33 ± 0.43 years, patients were assessed by the ASES, WORC, OSS, CS, and SSV. A clinical examination that included the bear-hug, the lift-off, and the belly-press tests was performed, in which the force exerted by the subjects was measured. In addition, all patients underwent MRI of the affected shoulder to assess repair integrity, tendon width, fatty infiltration, signal-to-signal ratio of the upper and lower SSC muscle, and atrophy of the SSC muscle.
Results:
No significant difference was found between the 2 groups on any of the clinical scores [ASES (P = .272), WORC (P = .523), OSS (P = .401), CS (P = .328), SSV (P = .540)] or on the range-of-motion or force measurements. Apart from a higher signal-to-signal ratio of the lower SSC muscle in the knotless group (P = .017), no significant difference on imaging outcomes was found between the 2 groups.
Conclusion:
Both techniques can be used in surgical practice, as neither was found to be superior to the other in terms of clinical or imaging outcomes at 2-year follow-up.
The key role of the subscapularis (SSC) muscle as internal rotator and anterior stabilizer of the humeral head and the consequences of its dysfunction have been described extensively in the literature. 5,8,16 Ruptures of the SSC tendon are estimated to account for 27.4% of the total number of rotator cuff ruptures. 33,35 As the result of the SSC muscle’s crucial biomechanical importance, the repair of SSC tears has been described as fundamental for shoulder function restitution. 1,7,34 Degenerative tears of the SSC tendon usually begin at the superior margin and continue inferiorly. 26,29,44 Therefore, the vast majority of degenerative SSC ruptures diagnosed during arthroscopy involve the upper half of the tendon. 18,26,41
Repairing the ruptured SSC into the footprint is crucial for the restoration of shoulder function. 9,22,37 Tears of the upper part of the SSC are often repaired with a single-anchor technique. 9,25,47,48 In this regard, both knotted and knotless single-anchor repair techniques have been proposed depending on the size and morphology of the tear. 9,14,48 In these 2 techniques, the different tension of the sutures and the resulting different distribution of the tensile force on the SSC could influence tendon healing and postoperative range of motion (ROM), especially external rotation. This phenomenon has already been observed in studies investigating supraspinatus tendon reconstruction or Bankart repair. 4,11,12 However, little is known about the outcomes of patients undergoing knotted versus knotless single-anchor techniques for the repair of the upper half of the SSC tendon. 16,46 To date, in routine clinical practice, the decision whether to use the knotted or knotless technique has not been evidence-based but has instead depended on surgeon experience.
The aim of the present study was to compare the 2-year clinical and magnetic resonance imaging (MRI) outcomes of knotless and knotted single-anchor repair techniques in patients with a transmural rupture of the SSC tendon. The null hypothesis was that the knotted and knotless repair techniques will not have significant differences in outcomes.
Methods
Patient Recruitment and Study Design
The protocol for this study received institutional review board approval. In total, 54 patients who had undergone SSC tendon repair at our department were retrospectively included in the present study. The following inclusion criteria were applied: (1) transmural upper SSC tendon tear (grade 2 or 3 according to Fox et al
17
) verified by preoperative MRI and arthroscopically confirmed at the time of surgery, (2) the application of a single-anchor technique for SSC tendon repair, (3) use of BioComposite knotted or knotless suture anchor implants composed exclusively of poly-
Fourteen patients were excluded from the study: 10 patients matched the exclusion criteria (8 underwent double-row repair or needed more than a single anchor and 2 had previously undergone surgery), and 4 patients were lost to follow-up (7.4%). Thus, 40 patients with a mean follow-up of 2.33 ± 0.43 years were included in the present study (Figure 1).
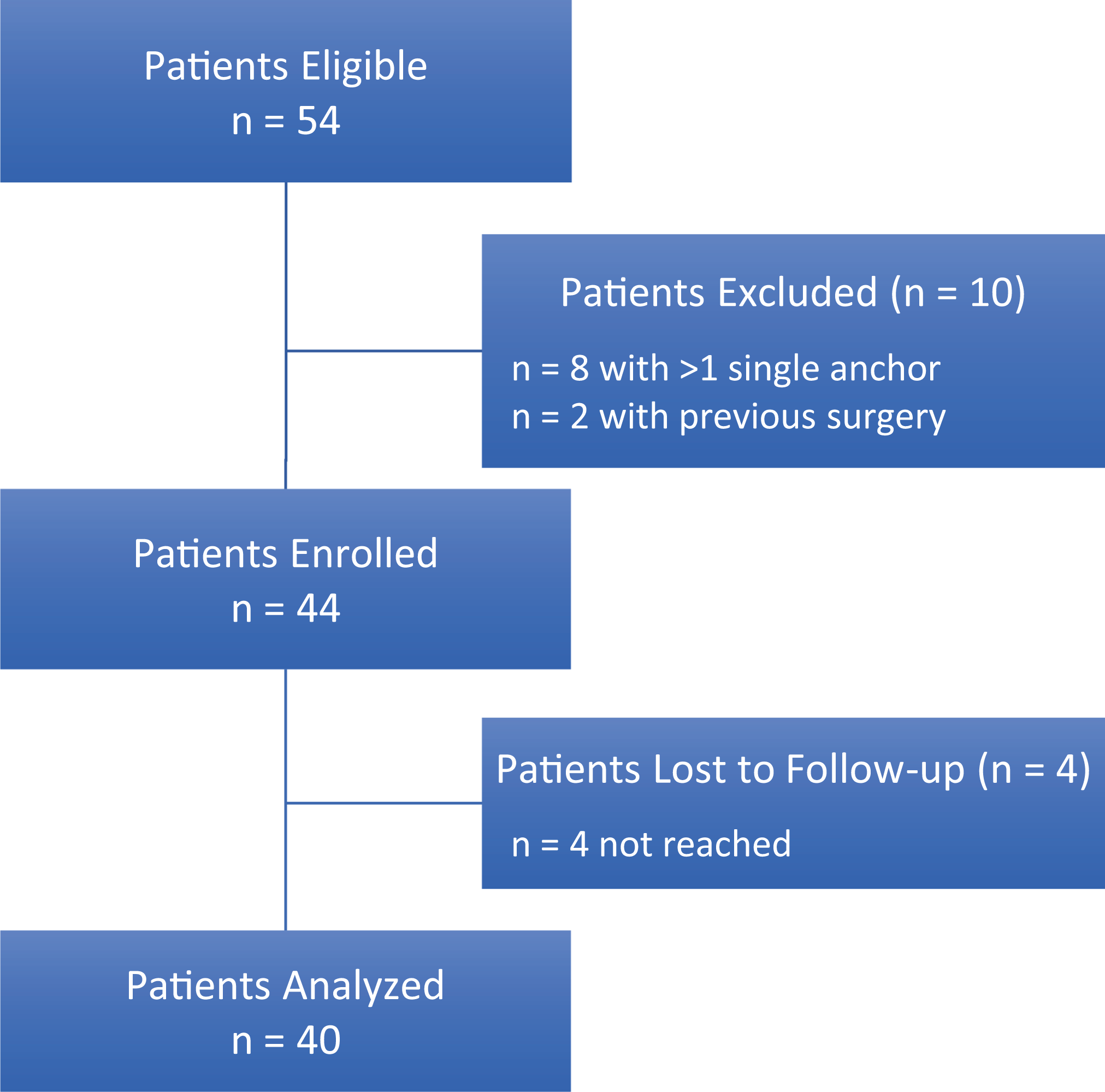
Flowchart of the present study.
After 2 years of follow-up, patients were asked to complete 5 clinical scores. In addition, clinical examination with force measurement was performed. Furthermore, to assess the integrity of the SSC tendon, all patients underwent an MRI scan of the affected shoulder. No difference was found between the 2 groups in terms of tendon quality (i.e., fatty infiltration, atrophy) on preoperative MRI.
Surgical Technique
All arthroscopies were completed under brachial plexus block and general anesthesia. The patients were placed in the beach-chair position. To stabilize the affected arm, a trimano hydraulic support (Maquet) was used. All surgical procedures were performed by a single orthopaedic surgeon
Group 1: Knotted technique using a 5.5 BioComposite Corkscrew (Arthrex).
Group 2: Knotless technique using a 5.5 BioComposite SwiveLock (Arthrex).
Knotted Technique
Following preparation of the bone bed with the punch supplied by the manufacturer, a double-loaded BioComposite 5.5 Corkscrew (Arthrex) was screwed into the bone until flush with the bone surface. The 2 no. 2 FiberWires (Arthrex) were subsequently passed through the SSC tendon and were tied with 6 half-hitches.
Knotless Technique
A FiberTape (Arthrex) was passed through the SSC tendon. Following preparation of the bone bed with the punch supplied by the implant manufacturer. The ends of the FiberTape were passed through the eyelet of a BioComposite 5.5 SwiveLock (Arthrex). The anchor was subsequently screwed into the bone until flush with the bone surface.
All concomitant pathologies encountered during the procedure were treated/repaired in both groups. All long head of biceps tendon (LHB) tenodesis were performed in the proximal portion of the bicipital groove using an interference screw technique. The indication for LHB tenodesis were instability of the LHB, superior labrum anterior and posterior lesions (SLAP > 1°), or partial rupture.
Postoperative Rehabilitation
To allow healing of the SSC tendon into the footprint, following surgery, the operated arm was held in an abduction pillow (Ultra Sling III, DJO, Ormed) for 6 weeks. Passive flexion and abduction to 90° were allowed for 6 weeks. Through the first 6 weeks, patients completed passive exercises. External rotation with the arm at the side was limited to 0° for 3 weeks and to 20° for another 3 weeks. At 7 weeks, patients deposed the abduction pillow and started active mobilization without strain. At 13 weeks, patients began strengthening exercises.
Clinical Assessment at Follow-up
Assessment of all patients took place at 2.33 ± 0.43 years of follow-up by a single clinician
The clinical examination was performed by an orthopaedic surgeon blinded to the performed intervention. The clinical examination included ROM and force measurements. Force was measured with a digital force gauge for different starting positions. In addition, 3 clinical tests specific for the SSC tendon with force measurement were performed:
MRI Examination at Follow-up
An MRI was performed at final follow-up using a 1.5-T MRI scanner (Magnetom TIM-Symphony, Siemens). The patients were positioned supine with the arm in neutral rotation at the side of the body. A dedicated standard shoulder coil was placed over the shoulder. The following protocol was developed and applied in the present study for all MRI scans.
Localizer sequence in all 3 directions of space. Parasagittal proton-density turbo spin-echo with fat saturation. T2-weighted multiple echo data image combination (MEDIC) 2D sequence (TR, 1.090 ms; TE, 21 ms; ST, 3 mm; FoV, 180 × 180 mm2; IM, 448 × 448 cm2). Paracoronal T1-weighted sequence (TR, 555 ms; TE, 11 ms; ST, 3 mm; FoV, 180 × 180 mm2; IM, 384 × 384 mm2). Transversal T1-weighted spin-echo sequence (TR, 530 ms; TE, 16 ms; ST, 3 mm; FoV, 160 × 160 mm2; IM: 512 × 512 mm2). Paracoronal double echo steady state (DESS) 3D with water excitation (TR, 23.2 ms; TE, 8.1 ms; ST, 1.5 mm; FoV, 160 × 160 mm2; IM, 256 × 256 mm2).
The MRI measurements were performed using the Osirix medical imaging viewer (Pixmeo SARL). To detect tears of the SSC on MRI, a standardized systematic approach was applied. The analysis consisted of the structured examination of the following morphological changes: rupture of the SSC tendon on an axial slice, subluxation of the long head of biceps tendon from the sulcus on axial slices, atrophy of the SSC muscle on sagittal images, and a bony avulsion of the SSC tendon including the minus tuberosity on sagittal slices. 2 The following parameters were determined using the MRI scans:
SSC tendon width (mm) 24
Fatty infiltration of the SSC muscle (degree) 20
Signal-to-signal ratio of the upper and lower SSC muscle (ratio) 42,43
Vertical, upper, and lower horizontal diameters of the SSC muscle (mm) 42,43
Sugaya Classification
To evaluate the SSC tendon healing in the footprint, the Sugaya classification for the SSC tendon was applied. The classification was defined in the following fashion: grade 1, sufficient thickness, homogeneous signal within the tendon; grade 2, sufficient thickness, heterogeneous signal within the tendon; grade 3, insufficient thickness without discontinuity; grade 4, minor discontinuity on more than 1 slice; and grade 5, major discontinuity. 45
SSC Tendon Width
To avoid bias, tendon width was measured in the transverse plane 1 mm medial to the bicipital sulcus with a line perpendicular to the tendon in all patients. 24
Fatty Infiltration of the SSC Muscle
The fatty infiltration of the SSC muscle was determined according to Goutallier et al 20 : grade 0, no fatty infiltration; grade 1, few fatty streaks within the muscle; grade 2, less fat than muscle within the muscle belly; grade 3, equal amounts of fat and muscle within the muscle belly; and grade 4, more fat than muscle within the muscle belly.
Signal-to-Signal Ratio of the SSC Muscle
To measure the quality of the SSC muscle, the signal-to-signal ratio was measured according to Scheibel et al. 42,43 On the Y-shaped position of the parasagittal sequences, the signal intensities of the superior and inferior SSC muscle, the infraspinatus muscle, and the background were determined. For this purpose, 5 identical circles (regions of interest) were respectively placed on the superior and inferior half of SSC muscles, in the infraspinatus muscle, and in the background (Figure 2). In this manner, using the imaging program, the minimum, maximum, and mean signal intensities, as well as the standard deviation, were determined for each region of interest. The formula proposed by Hendrick 40 was then used to determine the signal-to-signal ratio of the upper and lower SSC muscle.
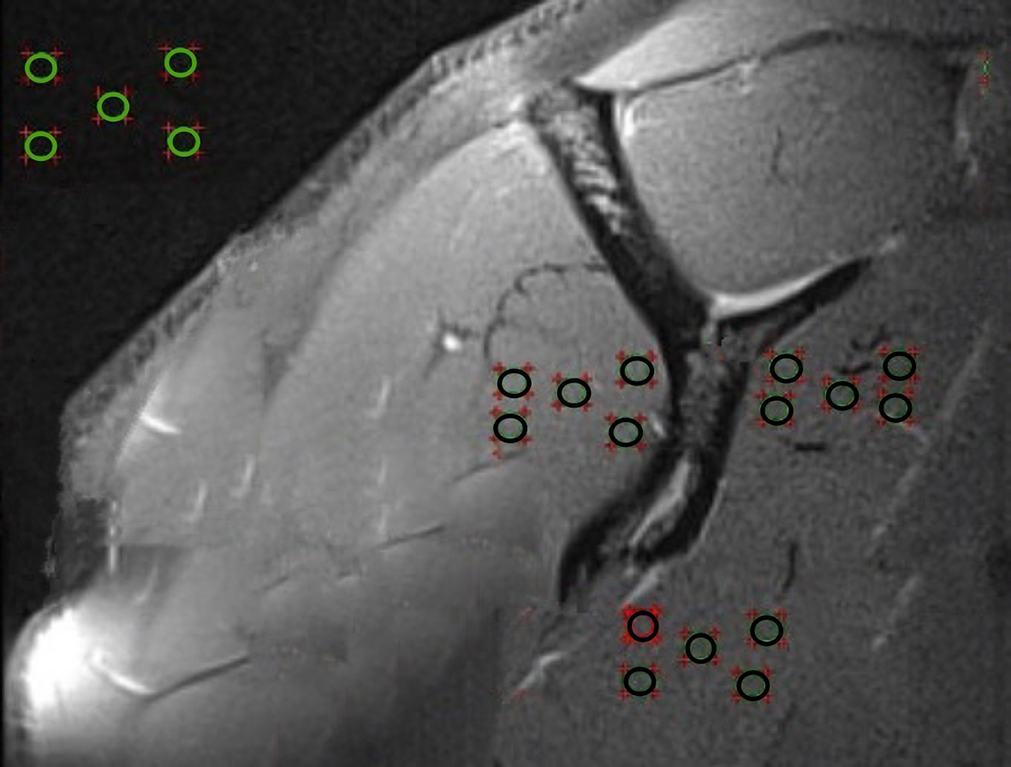
Determination of the signal-to-signal ratio of the subscapularis muscle on magnetic resonance imaging.
Vertical, Upper, and Lower Horizontal Diameter of the SSC Muscle
The atrophy of the SSC muscle was measured as proposed by Scheibel et al. 42,43 On the Y-shaped position of the scapula using the parasagittal sequences, the vertical diameter of the SSC muscle was first measured. Then, using a line perpendicular to the vertical diameter of the SSC tendon, the upper and lower diameters of the SSC muscle were determined.
The analysis of the MRI scans was completed for all measurements by a single clinician (M.K.)who was blinded to the intervention; the intraobserver reliability was 0.943 (95% confidence interval [CI], 0.906-0.965; P < .001), indicating excellent reliability.
Statistical Analysis
The collected data were analyzed using the Student t test for interval-scaled variables. Differences were considered significant for P values less than .05. The intraobserver reliability was evaluated using the intraclass correlation coefficient (ICC). The post hoc sample size was calculated assuming a power of 95%, with a level of significance of .05, hypothesizing an estimated between-group difference in mean WORC score of 3.0% and a standard deviation of 2.5%. Statistical analysis was performed with SPSS (Version 26, IBM).
Results
A total of 17 and 23 patients were included in the knotted and knotless group, respectively. Table 1 presents the demographic data of the knotted and knotless groups. No significance differences in demographic data were found between the 2 groups.
Demographic Data of the Knotted and Knotless Groups a

a Data are reported as mean ± standard deviation or percentage. ASA, American Society of Anesthesiologists classification; BMI, body mass index.
Table 2 identifies the additional surgical procedures performed on both groups. In this regard, no significant differences were observed between the 2 groups.
Additional Treatments Performed on the Knotted and Knotless Groups a
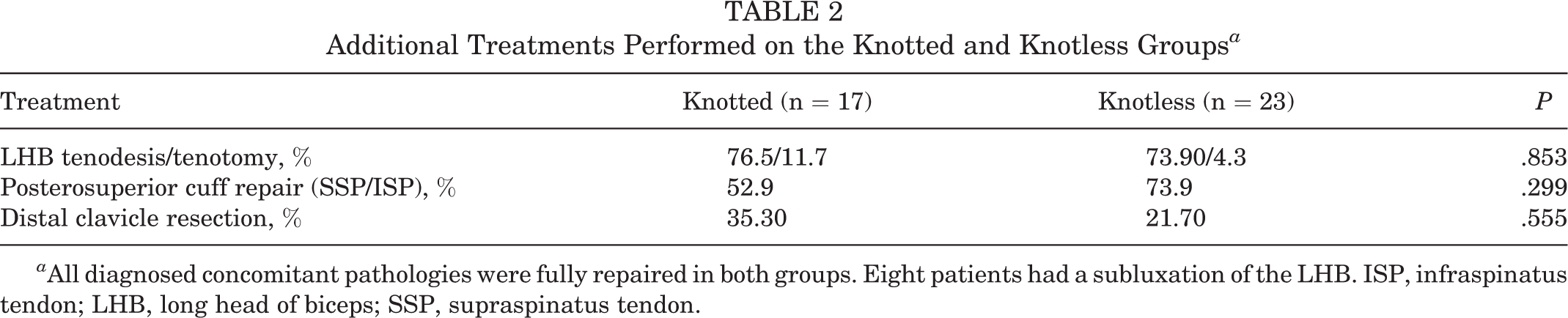
a All diagnosed concomitant pathologies were fully repaired in both groups. Eight patients had a subluxation of the LHB. ISP, infraspinatus tendon; LHB, long head of biceps; SSP, supraspinatus tendon.
The scores for the postoperative clinical assessments are presented in Table 3. No significant differences were found between the knotted and knotless technique groups in terms of clinical postoperative outcomes.
Scores for the Postoperative Clinical Assessments a
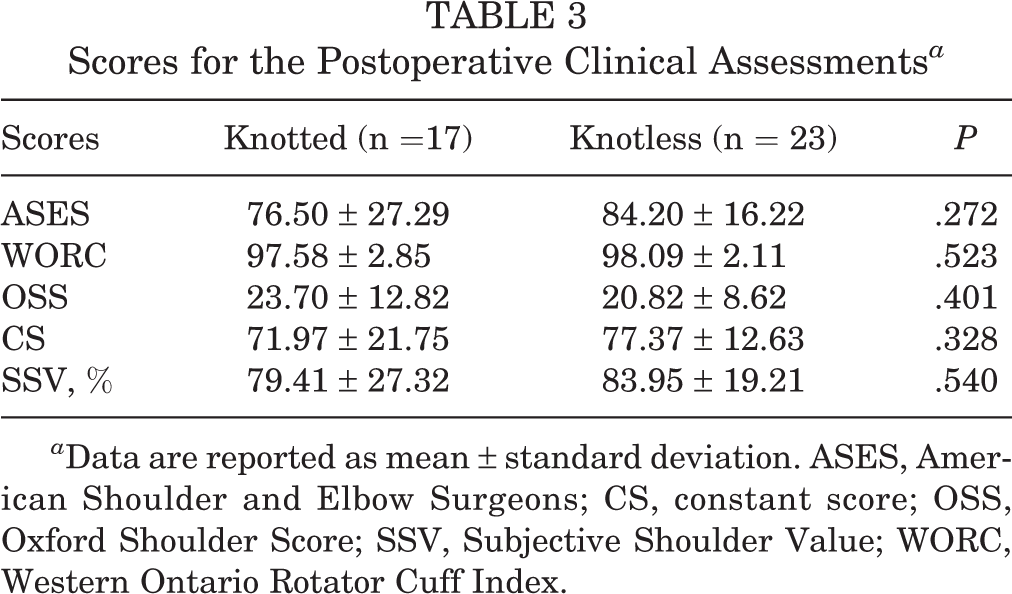
a Data are reported as mean ± standard deviation. ASES, American Shoulder and Elbow Surgeons; CS, constant score; OSS, Oxford Shoulder Score; SSV, Subjective Shoulder Value; WORC, Western Ontario Rotator Cuff Index.
The results of the clinical examination regarding the ROM in both groups are presented in Table 4. No significant differences were found between the 2 repair techniques.
Range of Motion of the Knotted and Knotless Groups a
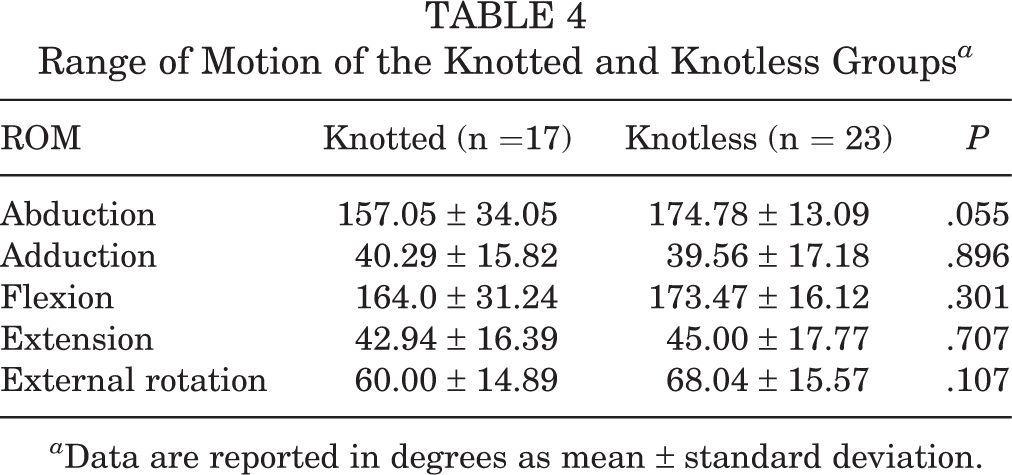
a Data are reported in degrees as mean ± standard deviation.
Table 5 presents the results of force measurement in different starting positions of the affected arm, including 3 for the SSC tendon-specific tests at follow-up. No significant differences were found between the 2 groups in terms of force measurement.
Force Measurement in Both Groups in Different Initial Positions of the Affected Arm a

a Data are reported in newtons as mean ± standard deviation.
The results of the radiological examination using the MRI scans are presented in Table 6. No re-rupture of the SSC tendon was detected in either group. Likewise, no significant differences with regard to SSC tendon width; fatty infiltration; or vertical, upper, or lower diameter of the SSC muscle were detected between the 2 groups. A significantly higher signal-to-signal ratio in the knotless group was found for the lower SSC muscle; however, this was not the case for the upper half.
MRI Examination of the Subscapularis Repair Integrity in Both Groups a

a Data are reported as mean ± standard deviation. Bolded P value indicates statistically significant differences between groups (P < .05, t test). SSC, subscapularis muscle.
Discussion
The most important finding of this study was that knotless and knotted single-anchor repair techniques in patients with transmural tears of the upper half of the SSC tendon corresponding to grade 2 or 3 according to the Fox and Romeo classification 17 showed, with the exception of the signal-to-signal ratio of the lower SSC muscle, no significant difference in terms of clinical and radiological outcomes at 2-year follow-up.
Transmural partial ruptures of the SSC tendon corresponding to grade 2 or 3 according to the Fox and Romeo classification 17 are frequently repaired using a single-anchor technique; however, only a few studies have investigated the value of this technique in terms of clinical and radiological outcomes. 23,25,32,38 The first clinical results following arthroscopic repair of the SSC were published by the research group of Burkhart and Tehrany 10 in 2002. In that study, 25 patients with lesions of the SSC tendon of varying degrees were analyzed 10.7 months after arthroscopic repair using a knotted technique. Ninety-two percent of the patients examined achieved good to excellent clinical results.
In 2008, Adams et al 3 studied 14 patients with rotator cuff tears involving the SSC tendon 5 years after arthroscopic repair. In 80% of the cases, good or excellent results were demonstrated. Furthermore, 88% of the patients stated that they were satisfied with the postoperative results. In addition, significant improvements in the ASES and UCLA shoulder scores were identified. In 2012, Denard et al 15 published 1 of the first studies with a longer follow-up on the results of arthroscopic knotted repair of the SSC tendon. In this study, 79 patients were examined 104 months after repair of the SSC tendon. Among other findings, increases in the UCLA score from 16.5 preoperatively to 30.1 postoperatively (P < .001) and in the ASES score from 40.8 preoperatively to 88.5 postoperatively (P < .001) were observed. Good or excellent outcomes were achieved in 83.3% of cases, and 92.4% of patients were satisfied with the postoperative outcomes.
In 2013, Lanz et al 31 presented the clinical results of 46 patients with large lesions of the SSC tendon corresponding to type III or IV according to the Lafosse classification. 30 All patients underwent arthroscopic repair and had a follow-up of 3 years. In this study, the constant score (CS) and UCLA score increased from 46.4 to 79.9 and from 15.1 to 31.5 points (P < .001), respectively. Ninety-eight percent of patients were satisfied or very satisfied. In 2017, Katthagen et al 23 studied 31 patients with isolated SSC tendon rupture type I or II according to the Lafosse classification. 30 All patients underwent arthroscopic repair of the SSC tendon using a single knotted (n = 13) or knotless (n = 15) suture anchor and were followed for 4.1 years. In this study, patients achieved significant postoperative improvement on all preoperative scores (P < .05). However, patients with type II lesions had significantly worse postoperative ASES scores than those with type I lesions. No significant difference in outcome was found between patients with the knotted and knotless technique. Lee et al 32 investigated the radiological and clinical outcomes of arthroscopic SSC repair with a knotted technique in 122 patients with massive rotator cuff ruptures. Patients were divided into 3 groups according to the size of the SSC lesion: intact SSC, less than one-third of the SSC affected, and more than one-third of the SSC affected. Significant improvement was seen in all 3 groups at a follow-up of 39.5 months, with no significant differences being identified between the groups. A re-rupture rate of 31.1% was observed, with the group with the largest SSC lesions having a significantly higher incidence of re-rupture.
The design of the current study differs from the studies cited previously; however, comparable results with regard to postoperative outcomes were observed. Likewise, to the patients in the abovementioned studies, the patients who participated in the current study achieved high scores for all clinical outcomes.
It was also interesting to note that no difference was found between the 2 groups in terms of ROM in the present study. With regard to ROM, it was expected that patients who underwent a knotted anchor technique would show deficits in external rotation, but this can be excluded based on the results of the present study. Concerning the radiological examination focused on tendon healing, the findings of the present study are not in agreement with those of the studies mentioned previously. In the present study, no re-rupture of the SSC was observed. From our point of view, this finding is certainly related to the differences between the design of the current study and those of related studies. In the present study, only ruptures of the SSC of grade 2 or 3 according to the Fox and Romeo classification 17 were analyzed, whereas most of the studies mentioned previously also included more severe ruptures. In the present study, a difference between the knotless and knotted repair technique was found only with respect to the signal-to-signal ratio of the lower half of the SSC muscle; this difference was in favor of the knotless technique. As all the repairs examined involved only the upper half of the SSC, this result was unexpected. A possible explanation for this finding could be that the knotted technique could possibly place more strain on the SSC muscle, which could lead to a less-pronounced signal on the MRI scan. In contrast, no difference was found between the 2 groups in terms of atrophy or fatty infiltration in the lower half of the SSC muscle.
The current study is subject to several limitations. First, a small number of patients was analyzed; this was because the exclusion criteria were defined as strictly as possible. However, the performed sample size calculation showed sufficient power. Second, in the present study, not only were isolated tears of the SSC tendon analyzed, as the majority of the studied patients presented comorbidities in the affected shoulder. The additional pathologies could have significantly influenced the postoperative results and caused a significant bias. However, the inclusion of exclusively isolated lesions of the SSC would not have reflected everyday clinical reality. Furthermore, no significant differences were found between the 2 groups in terms of comorbidities in the present study.
A third limitation was that preoperative results were not included, as this was a retrospective study. The authors of the present study did not intend to evaluate the clinical and radiological validity of SSC tendon tear repair in general given that this topic has already been adequately studied. Rather, it was the authors’ intention to directly compare the 2 repair techniques presented in this study. A comparison with the preoperative clinical results would certainly have supported the conclusions of the present study, but because this study has a retrospective design, no preoperative proms were available. However, the lack of preoperative shoulder scores is a limitation of the present study as it cannot definitively reflect whether and to what extent patients benefited from surgery regardless of the technique used.
Moreover, in the present study, 2 different suture materials in both groups were analyzed. Although a FiberTape was used in the knotless group, 2 FiberWires were used in the other group. This might have influenced the biomechanical properties of the respective reconstruction techniques. However, the authors aimed to investigate these 2 different techniques, as both are often used to treat full-thickness tears of the superior part of the SSC tendon. The use of identical sutures would certainly have increased the reproducibility of the present study but would have failed to achieve its primary aim.
Finally, patients were not randomized in the present study as it has a retrospective design. The decision whether to treat patients with a knotted or a knotless single-anchor technique was made by the surgeon during surgery and was associated with a change in surgical technique in our clinic over time. The study-related inclusion of the patients studied was performed postoperatively and was therefore not randomized. This limitation may have influenced the results of the present study and must be considered when interpreting the conclusions.
Conclusion
The results of the present study have shown that transmural partial tears of the SSC tendon corresponding to grade 2 or 3 according to the Fox and Romeo classification 17 can be repaired with both a knotted as well as knotless single-anchor technique, with both techniques producing similar clinical and radiological outcomes. Thus, implant selection for repair of grade 2 or 3 SSC tendon rupture, which has thus far been based on expert opinion, can now also be guided by the evidenced-based data presented in the current study. Future studies should extend this research by investigating a broader sample and analyzing a wider selection of implants including all-suture anchors.
Footnotes
Final revision submitted November 27, 2021; accepted December 8, 2021.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Ulm (ref No. 104/17).