
Abstract
Background:
Partial-thickness subscapularis (SSC) tears are frequently underdiagnosed due to subtle clinical presentation and the limited sensitivity of routine imaging modalities, particularly magnetic resonance imaging (MRI). Dynamic ultrasonography (USG) and structured test combinations may improve early detection.
Purpose/Hypothesis:
The purpose of this study is to compare the diagnostic accuracy of individual SSC-specific clinical tests, systematic 3-test combinations, USG, and MRI in detecting partial-thickness SSC tears, using arthroscopy as the reference standard. It was hypothesized that structured 3-test combinations and dynamic USG would outperform MRI in detecting partial SSC tears.
Study Design:
Cohort Study (diagnosis); Level of evidence, 2.
Methods:
A total of 46 patients undergoing arthroscopy for rotator cuff pathology were prospectively assessed using 6 SSC-specific clinical tests, dynamic USG, and standardized MRI sequences. Two independent, blinded observers evaluated all diagnostic modalities. All clinically relevant 3-test combinations were systematically analyzed and considered positive when ≥2 tests were positive. Diagnostic performance metrics—including sensitivity, specificity, accuracy, area under the curve (AUC), and interobserver agreement—were compared with arthroscopic findings.
Results:
The triads of Bear Hug + Napoleon + internal rotation lag sign and Bear Hug + Belly Press + Napoleon demonstrated the highest clinical diagnostic accuracy (sensitivity, 83.9% [95% CI, 67.4-92.9]; specificity, 100% [95% CI, 79.6-100.0]; AUC, 0.92 [95% CI, 0.85-0.98]). USG outperformed MRI across all diagnostic metrics (sensitivity, ≤96.8% [95% CI, 83.8-99.4]; AUC, 0.92 [95% CI, 0.83-1.00]), whereas MRI showed limited sensitivity (ranging from 61.3% [95% CI, 43.8-76.3] to 67.7% [95% CI, 50.1-81.4]). Interobserver agreement was almost perfect for MRI (κ≈ 0.91) and substantial for USG (κ≈ 0.68). Diagnostic accuracy was higher for Lafosse type 2 tears, although USG and the top-performing clinical triad remained effective across both tear subtypes.
Conclusion:
Dynamic USG and structured SSC-specific clinical test combinations offer superior diagnostic accuracy compared with MRI for partial SSC tears.
Keywords
The subscapularis (SSC) tendon plays a critical role in shoulder stability and function, contributing to internal rotation strength and anterior glenohumeral stability.30,38 Despite its biomechanical importance, partial-thickness SSC tears remain underrecognized and frequently missed during preoperative and even intraoperative evaluation.29,34 These lesions often present with subtle or nonspecific symptoms—such as anterior shoulder pain or internal rotation weakness—and may be masked by concomitant rotator cuff pathology.23,44 Untreated partial SSC tears may progress over time, alter shoulder biomechanics, and negatively influence postoperative outcomes, underscoring the importance of accurate early diagnosis.10,13
Magnetic resonance imaging (MRI) is commonly regarded as the reference standard for assessing rotator cuff pathology. 49 However, multiple studies have demonstrated that MRI has limited sensitivity in detecting partial-thickness SSC tears, with false-negative rates reported up to 40% in arthroscopically confirmed cases.2,12 This limitation is especially pronounced in Lafosse type 1 and type 2 tears, where the tendon may appear structurally intact on static imaging despite functional compromise. 25 Furthermore, MRI accuracy is influenced by radiologist expertise, slice orientation, and resolution constraints, contributing to variability in diagnostic performance.19,45
Physical examination remains a fundamental component of SSC assessment, with several maneuvers—including the Bear Hug, Lift-Off, Belly Press, Belly Off, and internal rotation lag sign—proposed to evaluate tendon integrity.4,6,18,21,31,36 However, the diagnostic performance of these tests varies considerably across studies, and most investigations have assessed them in isolation. Evaluating tests individually fails to account for the potential additive diagnostic value of combined maneuvers that challenge the SSC through different biomechanical pathways. 11 Additionally, few studies have directly compared clinical examination with ultrasonography (USG) and MRI using arthroscopy as the reference standard.12,31,32,49
Dynamic USG has gained attention as a cost-effective and accessible modality for evaluating rotator cuff pathology.9,15,33 It allows real-time visualization of tendon structure during active and passive movement, providing functional information not available on static MRI. Nonetheless, USG is often criticized for operator dependence and variability in reporting standards.32,33,41 The relative diagnostic performance of dynamic USG compared with MRI—and its potential role in a multimodal diagnostic algorithm for partial SSC tears—remains an important area of investigation.
Given the clinical effect of undiagnosed partial-thickness SSC tears and the limitations of MRI and isolated clinical tests, there is a need for a comprehensive diagnostic framework that integrates clinical examination, USG, and MRI. To our knowledge, no previous study has systematically evaluated all clinically relevant 3-test SSC combinations or compared these combinations directly with USG and MRI in a blinded, prospective design using arthroscopy as the gold standard.
Therefore, the aim of this study was to compare the diagnostic performance of SSC-specific clinical test combinations and USG evaluation with MRI in identifying partial-thickness SSC tears, using arthroscopic findings as the reference standard. A secondary aim was to assess interobserver agreement across modalities and to determine whether integrating clinical and imaging data could improve diagnostic accuracy and preoperative planning. We hypothesized that structured three-test clinical combinations and dynamic USG would demonstrate higher diagnostic accuracy than MRI for partial-thickness SSC tears.
Methods
Study Design
Between August 2019 and June 2024, patients scheduled for shoulder arthroscopy because of posterosuperior rotator cuff tears were prospectively evaluated at a single academic institution. This population was selected because patients with symptomatic posterosuperior cuff tears routinely undergo arthroscopy in our center, ensuring a consistent surgical cohort and allowing standardized intraoperative assessment of the SSC tendon.
All patients underwent independent clinical evaluation by 2 fellowship-trained orthopaedic surgeons, who performed 6 SSC-specific physical examination tests: Bear Hug, 5 Belly Press, 13 Belly Off, 35 Lift-Off, 14 Napoleon, 7 and the internal rotation lag sign. 16 To ensure clarity and reproducibility, all clinically relevant 3-test combinations were systematically generated from these 6 maneuvers and analyzed separately. A combination was considered positive when ≥2 of the 3 tests were positive.
Following clinical assessment, dynamic USG was independently performed by 2 experienced observers—one musculoskeletal radiologist and one orthopaedic surgeon—each blinded to clinical findings. USG was performed using a standardized scanning protocol with real-time dynamic assessment during passive and active external rotation.
Subsequently, the same 2 observers jointly interpreted the MRI studies while blinded to clinical and USG results. All patients then underwent diagnostic and therapeutic shoulder arthroscopy performed by a single senior shoulder surgeon, ensuring a consistent intraoperative assessment protocol. The operating surgeon remained blinded to all preoperative evaluations.
Each diagnostic modality—including individual tests, 3-test combinations, USG, and MRI—was compared with arthroscopy, the reference standard. Interobserver agreement was calculated for all methods using blinded, independent assessments.
Patients were excluded if they had full-thickness SSC tendon tears, were <18 years of age, declined to participate or refused repeated USG evaluation, had a history of revision surgery on the same shoulder, were diagnosed with secondary adhesive capsulitis, or presented with pseudoparalysis.
Power Analysis
A formal a priori power analysis was conducted using G*Power (Version 3.1.9.7; University of Düsseldorf) to determine the required sample size for the Wilcoxon signed-rank test. Assuming a moderate effect size (d = 0.5), a 2-tailed α of .05, and a power of 0.80, the minimum required sample size was calculated to be 35 patients. This effect size was selected based on previously published diagnostic accuracy studies involving shoulder imaging and physical examination. The final study cohort of 46 patients exceeded this requirement.
Study Population and Data Analysis
A total of 46 patients who metall predefined inclusion and exclusion criteria were enrolled in the final analysis. Patients were included if they were ≥18 years, had a clinical indication for shoulder arthroscopy, demonstrated a posterosuperior (supraspinatus [SSP] ± infraspinatus [ISP]) rotator cuff tear on preoperative evaluation, and completed all standardized SSC-specific physical examination tests, USG, and MRI protocols. This population was selected because posterosuperior cuff tears represented the standard arthroscopy cohort in which SSC evaluation was routinely and systematically performed; in contrast, isolated anterosuperior tears or traumatic lesions would introduce a heterogeneous population with different diagnostic pathways and indications for surgery. Importantly, the presence of a low-grade SSC tear alone did not constitute an indication for surgery in any patient. All surgical indications were based solely on symptomatic posterosuperior (SSP ± ISP) cuff pathology that had failed nonoperative management. The SSC evaluation was performed concurrently during arthroscopy as part of the standard intraoperative protocol.
Demographic and clinical variables—including age, sex, side of involvement, primary symptoms (pain and/or stiffness), trauma history, previous physical therapy, and medical comorbidities such as diabetes or smoking—were prospectively recorded using a standardized clinical form. No missing clinical or imaging data were present.
USG assessments 28 were performed using a high-resolution 10 to 15 MHz linear transducer (LOGIQ P9; GE Healthcare) with the patient seated and the arm positioned in the modified Crass posture. The SSC tendon was evaluated dynamically during passive and active external rotation, allowing real-time visualization of tendon excursion and footprint continuity. Partial-thickness tears were identified based on objective USG features, including focal hypoechogenicity at the footprint, partial fiber discontinuity without complete detachment, loss of the normal fibrillar architecture, and reduced tendon excursion during dynamic motion. Tendon integrity was categorized as intact, partial thickness, or full thickness.15,33,37
MRI examinations 1 were performed using a 3.0-Tesla scanner (Magnetom Skyra; Siemens Healthcare) following standardized shoulder protocols, including axial, oblique coronal, and oblique sagittal proton-density fat-suppressed (PD-FS) sequences. Partial-thickness SSC tears were defined using established MRI criteria, such as increased intratendinous signal on PD-FS images, focal thinning or partial fiber discontinuity, minor retraction without complete disruption, and preservation of the deep tendon layer. MRI findings were similarly classified as intact, partial-thickness tear, or full-thickness tear. 1
The diagnostic results of each individual clinical test, all systematically generated 3-test combinations (considered positive if ≥2 of the 3 tests were positive), USG, and MRI were recorded for each patient and compared with arthroscopic findings.
All surgical procedures were performed by the single senior shoulder surgeon, ensuring consistency in intraoperative evaluation. Arthroscopy was carried out in the beach-chair position. Visualization of the SSC tendon and its footprint was optimized using a 70° arthroscope with the shoulder positioned in flexion, internal rotation, and posterior translation. A routine diagnostic anterior portal was used in all cases. When indicated, a biceps tenotomy or tenodesis was performed before SSC inspection and repair.
SSC tears were classified intraoperatively using the Lafosse classification. 22 Type 1 tears were treated with debridement, whereas types 2 to 5 were repaired using a single- or double-row technique. Although Lafosse type 5 tears are generally managed with salvage surgical techniques, the type 5 tear in our cohort represented an acute, reparable injury with adequate tendon quality and excursion; therefore, primary repair was performed. For study purposes, Lafosse types 1 to 3 were considered partial-thickness tears, and types 4 to 5 were considered full-thickness tears. Full-thickness SSC tears were excluded based solely on arthroscopic confirmation, the definitive diagnostic method (Figure 1).

Lafosse partial tear classification. (A) Shoulder ultrasonography (USG), with visualization of the subscapularis tendon with USG (blue star), observation of the tear, and degeneration starting at the insertion site of the tendon (yellow arrows). (B) Magnetic resonance imaging, and (C) arthroscopic evaluation of the same patient and observation of the tear. Tub. Minus, lesser tuberosity.
Statistical Analysis
All statistical analyses were performed using Python programming language (Version 3.11; Python Software Foundation) with open-source packages including SciPy, Pandas, NumPy, and Scikit-learn. Continuous variables were summarized as mean ± SD, and categorical variables were presented as count and percentage.
Diagnostic performance metrics—including sensitivity, specificity, positive predictive value, negative predictive value, accuracy, F1 score, and their corresponding 95% CIs—were calculated for each individual clinical test, all systematically generated 3-test combinations, USG, and MRI, with arthroscopy serving as the reference standard. Receiver operating characteristic (ROC) curves and the area under the curve (AUC) with 95% CIs were computed to assess discriminative ability.
The Wilcoxon signed-rank test was used to compare paired diagnostic modalities. Interobserver agreement between examiners for clinical tests, USG, and MRI was evaluated using Cohen kappa coefficient, with 95% CIs calculated for all kappa values. Kappa statistics were interpreted according to the Landis-Koch classification system.
Agreement between each diagnostic modality and the arthroscopic reference standard was further examined using kappa analysis with associated P values. Diagnostic methods were compared and ranked using AUC, F1 score, and agreement statistics. All statistical tests were 2-tailed with a significance threshold of P < .05. Multiple comparisons were adjusted using the Holm-Bonferroni method, which did not alter the overall significance of the findings.
Results
Demographics
Of the 209 patients who underwent shoulder arthroscopic surgery between August 2019 and June 2024, 33 were excluded because of declining or missing USG evaluation and 21 were under the age of 18. Among the remaining 155 patients, 34 had previous surgery on the same shoulder, 28 had secondary adhesive capsulitis, 31 had pseudoparalysis, and 16 had full-thickness SSC tears, resulting in a final cohort of 46 patients included in the analysis (Figure 2).
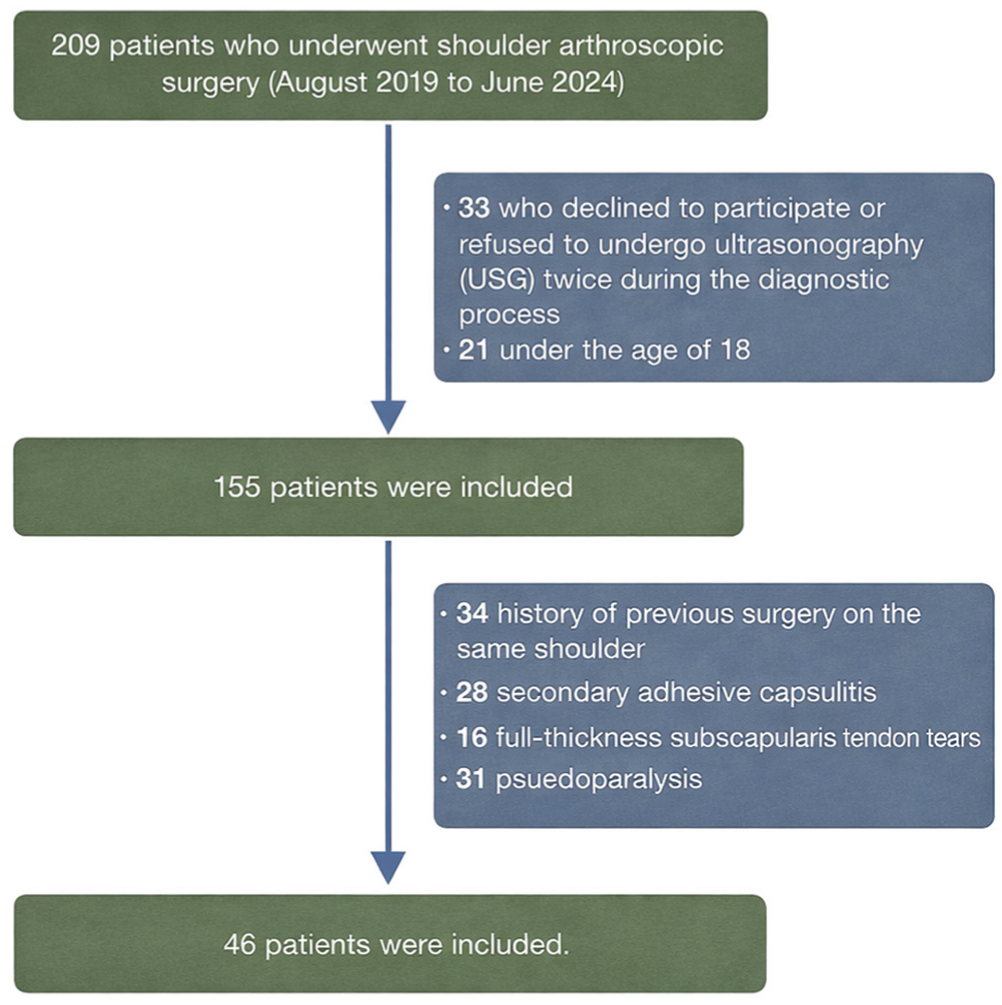
Diagram of the patient selection process.
A total of 46 patients were included in the study, consisting of 35 women (76.1%) and 11 men (23.9%). The mean age of the cohort was 55.7 ± 8.7 years (range, 39-71 years). The right shoulder was involved in 34 patients (73.9%), and the left in 12 patients (26.1%). Most patients had pain and/or functional limitation as the primary complaint. Nearly half of the patients had a history of physical therapy before surgery. Comorbid conditions included diabetes mellitus and smoking.
SSC tendon pathology was classified arthroscopically according to the Lafosse classification. Among the 46 patients, 15 (32.6%) had no tear (type 0), 13 (28.3%) were classified as type 1, and 18 (39.1%) as type 2, all of which represented partial-thickness tears (Table 1).
Demographics and Range of Motion by Tear Type a

Data are presented as n or mean ± SD. AH, acromiohumeral distance.
Individual Test Performance
Among the 6 individual physical examination tests evaluated, the Bear Hug test demonstrated the strongest overall diagnostic performance. It exhibited the highest sensitivity (90.3% [95% CI, 73.6-97.1]) and a favorable negative predictive value (78.6% [95% CI, 52.4-92.4]), indicating strong ability to exclude SSC tears when negative. Its agreement with arthroscopic findings was substantial (κ = 0.648).
Napoleon and Belly Off also showed favorable diagnostic profiles, characterized by high positive predictive values (values presented for observer 1 and observer 2, respectively: Napoleon, 92.9% [95% CI, 77.4%-98.0%] 93.3% [95% CI, 78.7%-98.2%]; Belly Off, 92.3% [95% CI, 75.9%-97.9%] – 92.9% [95% CI, 77.4%-98.0%]) and balanced accuracy. However, their sensitivities (Napoleon, 83.9% [95% CI, 67.4%-92.9%]; Belly Off, 77.4% [95% CI, 60.2%-88.6%]) were lower than those of Bear Hug, and their specificities were identical and relatively high for both tests (86.7% [95% CI, 62.1%-96.3%]).
In contrast, the Belly Press and Lift-Off tests demonstrated more limited diagnostic reliability when assessed individually. Belly Press showed high specificity (86.7% [95% CI, 62.1%-96.3%]) but low sensitivity (51.6% [95% CI, 34.8%-68.0%]) and a modest negative predictive value (46.4% [95% CI, 29.5%-64.2%]). Conversely, Lift-Off demonstrated very high sensitivity (96.8% [95% CI, 83.8%-99.4%]) but markedly poor specificity (46.7% [95% CI, 24.8%-69.9%]), resulting in suboptimal balance across diagnostic metrics. Despite achieving statistical significance (all P < .05), these findings suggest that Belly Press and Lift-Off should be interpreted cautiously when used as standalone assessments.
Combination Superiority
The use of 3-test combinations substantially improved diagnostic performance compared with individual physical examination maneuvers. All combinations demonstrated statistically significant agreement with arthroscopic findings (P < .01), and several achieved high discriminatory capacity as reflected by their AUC values. Based on AUC—the most robust measure of diagnostic discrimination—the 2 highest-performing combinations were (1) Bear Hug + Napoleon + internal rotation lag sign and (2) Bear Hug + Belly Press + Napoleon. Both triads achieved the highest AUC values (0.92 [95% CI, 0.85-0.98]) and identical overall accuracies (89.1% [95% CI, 77.0%-95.3%]), with balanced sensitivity and specificity profiles (both: sensitivity 83.9% [95% CI, 67.4%-92.9%], specificity 100% [95% CI, 79.6%-100.0%]).
Although its AUC was slightly lower, the triad of Bear Hug + Belly Off + Napoleon (AUC, 0.85 [95% CI, 0.75-0.95]) demonstrated comparably high diagnostic accuracy (84.8% [95% CI, 71.8%-92.4%]) with strong sensitivity (83.9% [95% CI, 67.4%-92.9%]) and robust specificity (86.7% [95% CI, 62.1%-96.3%]). This reproducibility highlights its reliability as a clinically useful diagnostic option.
Other high-performing combinations included Bear Hug + Belly Off + Lift-Off and Bear Hug + Belly Press + internal rotation lag sign, both demonstrating high accuracies and balanced diagnostic performance, although their AUC values were lower than those of the top-performing triads. Across all analyses, combinations incorporating the Bear Hug test consistently ranked among the strongest performers, underscoring its central role in enhancing clinical diagnostic accuracy for partial SSC tears (Table 2 and Supplemental Material Table S1, available separately).
Summary of Diagnostic Performance Patterns by Observer a
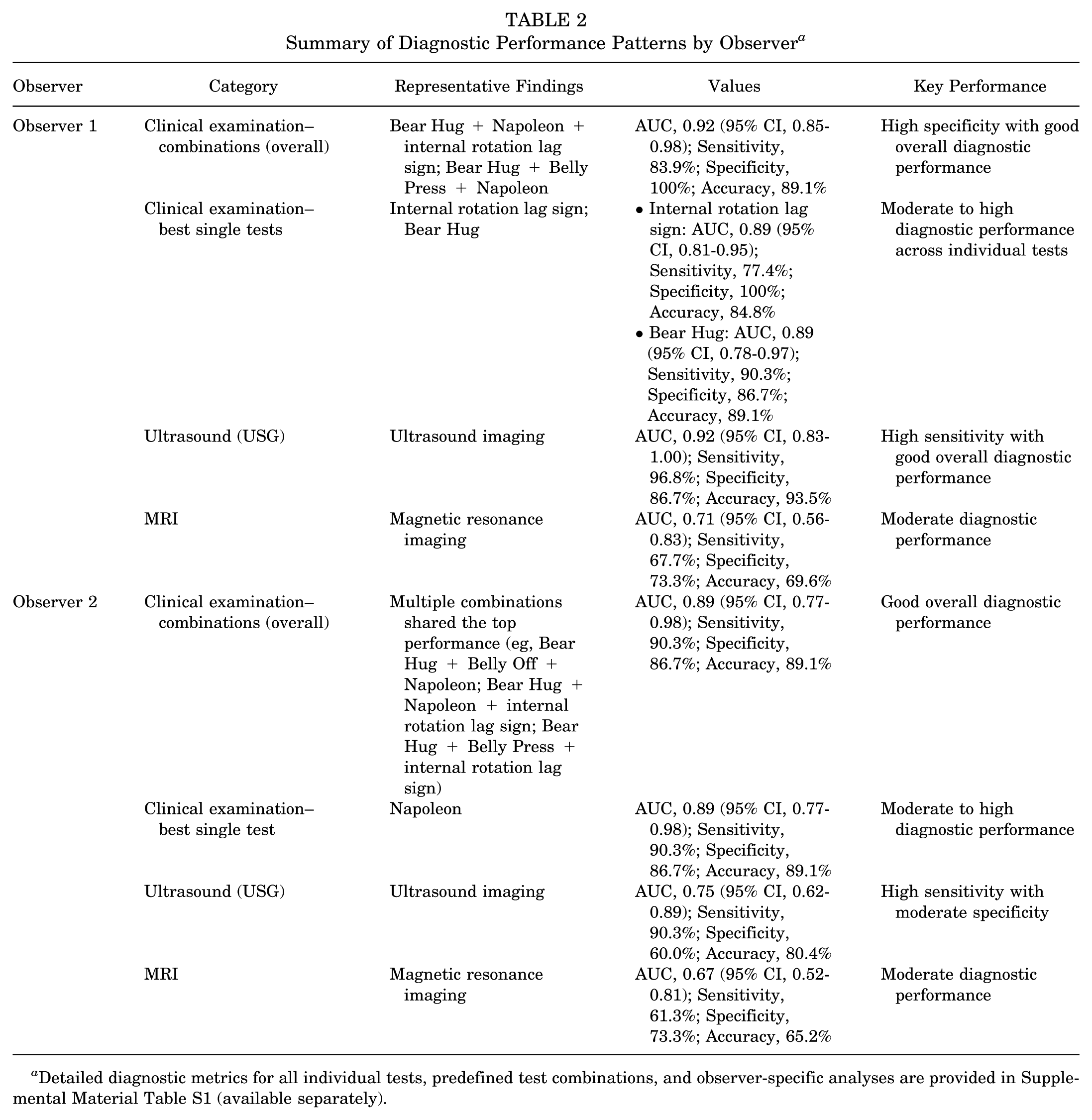
Detailed diagnostic metrics for all individual tests, predefined test combinations, and observer-specific analyses are provided in Supplemental Material Table S1 (available separately).
USG Versus MRI Comparison
Both USG and MRI demonstrated acceptable agreement with arthroscopic findings in the evaluation of Lafosse types 1 and 2 SSC tears; however, their diagnostic performances differed markedly.
USG consistently outperformed MRI across all key diagnostic parameters. For observer 1, USG achieved a sensitivity of 96.8% (95% CI, 83.8%-99.4%), specificity of 86.7% (95% CI, 62.1%-96.3%), and an overall accuracy of 93.5% (95% CI, 82.5%-97.8%), with high positive and negative predictive values. Observer 2 showed slightly lower but still strong results, with a sensitivity of 90.3% (95% CI, 75.1%-96.7%) and an accuracy of 80.4% (95% CI, 66.8%-89.3%). These data highlight the reliability of USG in both detecting and excluding partial SSC pathology.
In contrast, MRI demonstrated substantially weaker diagnostic performance. Sensitivity remained below 70% for both observers (61.3% [95% CI, 43.8%-76.3%] and 67.7% [95% CI, 50.1%-81.4%]), and negative predictive values were particularly limited (52.4% [95% CI, 32.4%-71.7%] and 47.8% [95% CI, 29.2%-67.0%]), reducing the utility of MRI in ruling out disease. Although specificity was moderate (73.3% [95% CI, 48.0%-89.1%] for both observers), MRI accuracy was lower than that of USG and most clinical test combinations.
Overall, these findings indicate that USG provides superior diagnostic accuracy and more dependable clinical performance than MRI for detecting partial SSC tendon tears.
All Tests Comparison
When all diagnostic modalities were evaluated against arthroscopy, 3-test combinations generally demonstrated superior performance compared with single clinical maneuvers. Several combinations achieved high discriminatory ability, with AUC values in the upper range of all tested methods. Based on AUC—which provides the most comprehensive measure of diagnostic discrimination—the 2 highest-performing clinical combinations were Bear Hug + Napoleon + internal rotation lag sign and Bear Hug + Belly Press + Napoleon, each achieving the highest AUC value of 0.92 (95% CI, 0.85-0.98) and an overall accuracy of 89.1% (95% CI, 77.0-95.3). These triads also demonstrated balanced sensitivity-specificity profiles, supporting their strong diagnostic capability.
Although the Bear Hug + Belly Off + Napoleon triad demonstrated a slightly lower AUC (0.89), it achieved the almost same overall accuracy with strong sensitivity and robust specificity, indicating that it remains a reliable and clinically useful diagnostic option.
Among individual maneuvers, the Bear Hug test remained the most dependable single test, demonstrating the strongest overall balance of sensitivity, specificity, and discriminative performance. In contrast, Belly Press and Lift-Off exhibited greater variability across diagnostic metrics, limiting their utility as standalone assessments.
Across imaging modalities, USG demonstrated superior diagnostic accuracy and discriminatory performance (AUC, 0.917; κ≈ 0.68) compared with MRI, which showed the lowest performance metrics (AUC, <0.71; κ < 0.40). Overall, structured clinical test combinations and USG provided the most robust diagnostic performance for partial SSC tears, clearly surpassing MRI (Figures 3 and 4).

Area under the curve (AUC), F1 score, and kappa scores of observer 1. Int.Rot.Lag.Sign, internal rotation lag sign; MR, magnetic resonance; ROC, receiver operating characteristic; USG, ultrasonography.

Area under the curve (AUC), F1 score, and kappa scores of observer 2. Int.Rot.Lag.Sign, internal rotation lag sign; MR, magnetic resonance; ROC, receiver operating characteristic; USG, ultrasonography.
Subgroup Analysis by Lafosse Classification
When stratified by Lafosse classification, diagnostic performance varied considerably between type 1 and type 2 SSC tears. Overall, tests exhibited higher ROC AUC values in Lafosse type 2 tears, reflecting greater diagnostic reliability in more extensive lesions.
Combined tests, particularly those incorporating the Bear Hug, Belly Press, and Napoleon maneuvers, demonstrated the strongest discriminative capacity, with ROC AUC values consistently exceeding 0.75 in type 2 cases. In contrast, isolated tests such as the Lift-Off or internal rotation lag sign showed diminished performance, particularly in detecting type 1 tears, where AUC values frequently remained below 0.65.
Despite reduced accuracy in partial tears (Lafosse 1), certain composite maneuvers maintained moderate diagnostic value. Notably, the Bear Hug test alone yielded stable AUC values across both subgroups (types 1 and 2), indicating its potential as a standalone screening tool.
Agreement between observers was acceptable, and test ranking by AUC was largely consistent, supporting the robustness of the observed subgroup trends. Figure 5 summarizes the ROC AUC values of all evaluated tests across Lafosse subtypes, demonstrating a clear performance gradient favoring more advanced tears.

Subgroup analysis. AUC, area under the curve; Int.Rot.Lag.Sign, internal rotation lag sign; MR, magnetic resonance; ROC, receiver operating characteristic; USG, ultrasonography.
Interobserver Consistency
Interobserver agreement was assessed for all diagnostic modalities, including individual physical examination tests, multitest combinations, USG, and MRI, by calculating Cohen kappa coefficients (reported as k_consistency). All values were statistically significant (P < .05), confirming nonrandom agreement between observers across all methods.
Agreement ranged from moderate to perfect (k_consistency = 0.47-1.00). The highest reproducibility was observed for the Lift-Off test (k_consistency = 1.00). MRI also demonstrated almost perfect consistency (k_consistency ≈ 0.91), whereas USG showed lower, but still substantial agreement (k_consistency ≈ 0.68). Multitest combinations such as Bear Hug + Belly Off + Napoleon or Bear Hug + Belly Off + internal rotation lag sign reached excellent reproducibility (k_consistency ≈ 0.90). Among individual maneuvers, Bear Hug, Belly Off, and Napoleon achieved substantial to almost perfect agreement (k_consistency ≥ 0.85), while Belly Press showed only moderate reliability (k_consistency = 0.47).
These findings indicate that when performed by different experienced clinicians, most SSC-specific tests and MRI can be applied with high reproducibility, while USG—despite its superior diagnostic accuracy—displayed lower interobserver consistency (Figure 6).

Interobserver agreement. Int.Rot.Lag.Sign, internal rotation lag sign; MR, magnetic resonance.
Discussion
The principal finding of this study is that high-performing SSC-specific clinical test combinations consistently outperformed MRI and achieved diagnostic accuracy approaching that of USG. To our knowledge, this is the first blinded, prospective investigation to systematically evaluate all clinically relevant triads of SSC-specific tests and directly compare them with USG and MRI against an arthroscopic reference standard. These findings underscore the limitations of relying on imaging alone and support the use of a multimodal diagnostic strategy. Furthermore, all diagnostic assessments—clinical examination, USG, and MRI—were independently performed by 2 experienced observers, strengthening methodological rigor and enhancing generalizability.
Partial SSC tears remain diagnostically elusive due to their subtle clinical presentation and inconsistent imaging features.8,23,44 These lesions are frequently missed both preoperatively and even intraoperatively without meticulous arthroscopic evaluation.8,20,47 Increasing evidence suggests that unrecognized partial SSC tears contribute to internal rotation weakness, anterior shoulder pain, and postoperative functional decline.27,48 Thus, accurate preoperative identification is essential to optimize patient care.
Although MRI remains a routine component of rotator cuff evaluation, its sensitivity for detecting partial SSC tears varies widely (31%-73%).2,12,26,42 Previous studies have shown that MRI frequently fails to detect small or upper-third SSC lesions.2,12,25,26 These discrepancies may be explained by differences in MRI slice orientation, reader experience, and the subtle, upper-third partial lesions that are frequently underestimated on static imaging. Consistent with this literature, our results demonstrated that MRI maintained excellent interobserver agreement yet persistently low sensitivity and negative predictive value, reflecting the well-described paradox whereby MRI is reproducible between observers but insufficiently sensitive for early or subtle SSC pathology.24,45
Interestingly, although USG demonstrated markedly superior diagnostic accuracy compared with MRI in our cohort, its interobserver agreement was substantially lower. This reflects a well-described diagnostic paradox. The dynamic nature of USG—allowing real-time visualization of tendon excursion, subtle fiber defects, and functional continuity—enhances sensitivity but also increases observer-dependent variability, particularly in Lafosse type 1 tears where intratendinous defects are subtle.32,33 In contrast, MRI provides a static and standardized field of view that inherently improves reproducibility between readers, yet lacks the ability to detect early or fine partial-thickness abnormalities. These factors explain how USG can yield higher accuracy while still demonstrating lower interobserver consistency than MRI.
Physical examination, although fundamental to clinical assessment, has historically shown variable performance when maneuvers are used in isolation.5,6,13,16,39,46 In our cohort, the Bear Hug test demonstrated the strongest standalone performance, while Napoleon also showed favorable diagnostic characteristics. In contrast, Belly Press and Lift-Off exhibited imbalanced sensitivity-specificity profiles, consistent with previous studies indicating that individual tests may not reliably distinguish partial SSC lesions. 3 Importantly, diagnostic accuracy improved substantially when maneuvers were combined.
While prior investigations have assessed selected combinations,4,11 the present study systematically evaluated all clinically relevant triads and demonstrated that combinations incorporating Bear Hug, Napoleon, and Belly Off consistently ranked among the top performers. For observer 1, the highest discriminative performance was achieved by Bear Hug + Napoleon + internal rotation lag sign and Bear Hug + Belly Press + Napoleon. For observer 2, several triads—including those incorporating Bear Hug, Napoleon, Belly Off, and occasionally Lift-Off—achieved similarly high AUC values (0.89) and comparable accuracy. Despite minor observer-dependent variation, combinations containing these key maneuvers repeatedly demonstrated high diagnostic performance and agreement with arthroscopy, clearly surpassing MRI across multiple parameters. These results reinforce the concept that SSC pathology is best evaluated using a structured, multimaneuver approach rather than relying on individual tests.5,18,36
A notable methodological strength of this study was the stratification of SSC tears by thickness, which is often overlooked in previous literature. This approach reduces diagnostic heterogeneity and facilitates more accurate interpretation of test performance. Nair etal 32 emphasized the importance of such stratification, whereas Jang etal 17 excluded pseudoparalysis and stiffness to minimize confounding. Similarly, in our study, patients with pseudoparalysis were excluded to ensure that test performance reflected true tendon pathology. This methodological decision likely enhanced internal validity and also aligns with reviewer recommendations regarding missing data and confounder control.
USG demonstrated superior sensitivity and diagnostic accuracy compared with MRI, achieving values close to those of the best-performing test triads. Sensitivities reached 96.8% with AUC values above 0.91, consistent with Zhu etal, 49 who reported the superiority of dynamic USG over MRI. Although operator dependence remains a recognized limitation, as highlighted in previous literature and by the reviewers,32,33,41 USG consistently outperformed MRI across both observers and offered unique advantages in visualizing tendon morphology under physiological motion and load, detecting subtle defects that may escape static MRI.40,43 Interobserver agreement for USG was moderate to substantial (κ≈ 0.68), slightly lower than MRI but still acceptable in experienced hands.
Subgroup analysis further demonstrated that diagnostic accuracy was higher for Lafosse type 2 than for type 1 tears, reflecting the greater anatomic disruption in more extensive lesions. Notably, USG maintained excellent sensitivity even in type 1 tears, while the top-performing clinical test combinations were consistent across both subgroups. These findings reinforce the evolving paradigm that USG, when integrated with structured physical examination, should be considered not merely complementary but potentially frontline in the diagnostic algorithm for partial SSC pathology.24,49
Limitations and Strengths
This study has several notable strengths. It employed a prospective and blinded design with standardized arthroscopic verification of all SSC lesions. All diagnostic modalities—physical examination, USG, and MRI were independently assessed by 2 experienced observers, which allowed for interobserver agreement analysis across all methods. The substantial agreement observed for USG and the top-performing clinical test combinations supports the reproducibility and reliability of these diagnostic strategies in clinical practice. Importantly, unlike most previous studies that assessed diagnostic tools in isolation or in pairs, our study enabled a comprehensive, head-to-head comparison of all 3 modalities within the same patient cohort, using arthroscopy as the reference standard. This integrated design allowed for a more nuanced understanding of the relative strengths and limitations of each diagnostic approach in detecting partial-thickness SSC tears.
Despite its methodological strengths, the study has several limitations. The sample size was relatively modest, which may limit the statistical power for some subgroup analyses. In addition, the clinical test combinations were determined empirically and have not been previously validated in external cohorts. Last, although observer expertise was high, the performance of USG remains inherently operator dependent, which may affect generalizability in less experienced hands. Future multicenter studies with larger cohorts are warranted to validate these findings and further refine diagnostic algorithms.
Conclusion
Dynamic USG combined with structured SSC-specific test combinations provides superior accuracy and reproducibility compared with the conventional pathway of isolated physical examination followed by MRI. This integrated approach reduces underdiagnosis of early lesions, enhances preoperative planning, and should be considered a frontline strategy in the evaluation of partial SSC tears.
Supplemental Material
sj-xlsx-1-ojs-10.1177_23259671261418678 – Supplemental material for Comparison of Clinical Examination, Ultrasonography, and Magnetic Resonance Imaging in the Diagnosis of Arthroscopically Confirmed Partial Subscapularis Tears
Supplemental material, sj-xlsx-1-ojs-10.1177_23259671261418678 for Comparison of Clinical Examination, Ultrasonography, and Magnetic Resonance Imaging in the Diagnosis of Arthroscopically Confirmed Partial Subscapularis Tears by Ali Can Koluman, Nezih Ziroglu, Tuna Demirbas and Ersin Ercin in The Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted December 4, 2025; accepted January 4, 2026.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study was approved by the Clinical Research Ethics Committee of Bakirkoy Dr. Sadi Konuk Training and Research Hospital, Istanbul, Türkiye (Approval No. 08.07.2019, 2019/181).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.