
Abstract
Background:
Historically, tendon-to-bone fixation has relied on knot tying. However, considerable variability exists in knot-tying strength among surgeons.
Purpose/Hypothesis:
The purpose of this study was to compare the biomechanical properties of knotted and knotless fixation and to evaluate variability among surgeons. The hypothesis was that knotless constructs would be stronger and have less variability as compared with knotted constructs.
Study Design:
Controlled laboratory study.
Methods:
A total of 34 orthopaedic surgeons participated in a laboratory study to compare knotted and knotless constructs, where 104 knotted constructs were performed with No. 2 suture, 21 knotless constructs with No. 2 suture (K2 group), and 79 knotless constructs with suture tape (KT group). Mechanical testing was performed to compare load at 3 mm of displacement, load to failure, and stiffness of each construct.
Results:
The mean load at 3 mm of displacement was greatest in the KT group, with significant differences among all 3 groups (P < .001). Load to failure was significantly greater in the KT group as compared with the K2 group and the knotted group (P < .001), but there was no difference between the K2 and knotted groups (P ≥ .999). Stiffness and displacement were also greatest in the KT group. Based on the F test, the variance in load to failure was significantly different between the knotted and knotless constructs, with the knotted group demonstrating greater variability (SD, 94 N) than the KT (SD, 38 N) and K2 (SD, 17 N) groups (P < .001).
Conclusion:
Knotless fixation with suture tape had improved biomechanical performance as compared with knots or knotless fixation with No. 2 suture. In addition, knotless fixation had less variability in biomechanical properties among multiple surgeons.
Clinical Relevance:
This study may be relevant for surgeons choosing between knotted and knotless constructs as well as for considerations in the design of rotator cuff repair constructs.
The goal of rotator cuff repair from a biomechanical perspective is to maximize fixation at time zero to encourage tendon-to-bone healing. 7,16 Historically, fixation has relied on knot tying to achieve tendon-to-bone fixation. A variety of knots have been proposed—from simple to complex and from static to sliding. To maximize fixation strength and reduce slipping, knot security (ie, ability of knot to resist slippage) and loop security (ie, ability to maintain a tight suture loop without slippage to minimize gap formation) should be maximized. 2,13 However, a recent study demonstrated that there is considerable variability in knot strength among arthroscopic surgeons. 9
The advent of knotless fixation technology has provided an alternative for tendon-to-bone fixation. Such devices rely on fixation between the suture and the anchor at the bone-anchor interface or via a mechanism within the anchor itself. In addition to the advantages of saving time 20 and reducing the potential for knot impingement, 18 these constructs may be stronger and more reproducible than knotted constructs. While a variety of factors relate to rotator cuff healing, improved strength and reliability may help improve rotator cuff healing. 8,19
The purpose of this study was to compare the biomechanical properties of knotted and knotless fixation and to evaluate variability among surgeons. The hypothesis was that knotless constructs would be stronger and have less variability than knotted constructs.
Methods
Study Design
A laboratory study was performed to compare knotted and knotless constructs. Orthopaedic surgeons taking part in a surgical training event were invited to participate. All surgeons chosen to participate in the study were actively practicing, board-certified, expert-level arthroscopists who routinely perform rotator cuff repair. A total of 34 surgeons agreed to participate.
Knotted and Knotless Constructs
The model used rigid polyurethane blocks composed of 2 layers: the top layer had a density of 20 lb/ft3 and a height of 3 mm, and the main layer had a density of 10 lb/ft3 and a height of 40 mm (Sawbones). After being introduced to the study via a presentation, each surgeon immediately performed 3 knotted and 3 knotless constructs. For the knotted constructs, each surgeon was asked to tie his or her preferred knot to simulate a typical knot seen in clinical practice.
For the knotted technique, a 5.5-mm fully threaded anchor (BioComposite Corkscrew; Arthrex Inc) loaded with No. 2 nonabsorbable braided suture made of ultrahigh–molecular weight polyethylene (UHMWPE; FiberWire; Arthrex Inc) was placed in the foam block. A 35-mm steel tube was then placed directly over the anchor, and the surgeon tied his or her preferred arthroscopic knot (Figure 1). To mimic the real world, neither the type of knot nor the usage of a suture pusher was controlled. A total of 104 knotted constructs were performed: 32 surgeons performed 3 knots; 1 surgeon, 6 knots; and 1 surgeon, 2 knots.

Examples of a knotless suture tape construct (left) and knotted suture construct (right) performed in a foam block.
In the knotless technique, either No. 2 FiberWire suture or a 2-mm suture tape composed of UHMWPE and polyester yarns over a core of FiberWire (FiberTape; Arthrex Inc) was preplaced around the steel tube. Then the suture was threaded through the eyelet of a 5.5-mm knotless anchor (BioComposite SwiveLock; Arthrex Inc), and the anchor was secured into the Sawbone socket. The surgeon was instructed to remove slack in the construct prior to placement of the anchor (Figure 1). Each surgeon used the same suture for 3 attempts (eg, if No. 2 FiberWire was used, it was used for all 3 tries), but the choice of which of the 2 suture materials to use was up to the surgeon. The knotless constructs were divided into 2 groups based on the suture material. Group K2 consisted of 21 cases based on No. 2 FiberWire; 7 surgeons performed 3 attempts each. Group KT consisted of 79 attempts with suture tape; 25 surgeons performed 3 attempts each, and 2 surgeons performed 2 attempts each.
Mechanical Testing
Following fixation, the steel tube was removed, and the constructs were subjected to mechanical testing. The foam blocks were secured to a dynamic tensile testing system (ElectroPuls E10000; Instron) with the sutures attached to a hook on a metal rod (Figure 2). Specimens were each preloaded at 5 N at 1 mm/s to remove any initial slack. 9

Testing setup. pcf, pounds per cubic foot.
After preloading, each specimen was pulled to failure at a constant displacement rate of 1 mm/s. Data were collected at 500 Hz. Maximum load (Fmax) was defined as the ultimate failure load at which the suture or anchor failed. The mechanism of failure was noted. Load over displacement was recorded for each specimen and was used to calculate load at 3 mm (termed clinical failure 4 ), maximum load, and stiffness. 4 Stiffness was calculated by measuring the slope of the linear portion of the load-displacement curve by using a best-fit line that would provide an R 2 value ≥0.99. Stiffness of each specimen was compared with the average construct stiffness evaluated from Burkhart et al 3 of 70 N/mm.
Statistical Analysis
Statistical analysis was performed with Sigma Plot Statistics for Windows (v 13.0; Systat Software Inc). The 3 groups were compared with a Kruskal-Wallis test to analyze differences in load at 3 mm, maximum load, stiffness, and displacement. Differences in maximum load within each group were also compared among attempts 1, 2, and 3 for each construct. An F test was performed to compare SDs to determine variance in load to failure among the groups. The significance level was set at P = .05.
Results
Table 1 summarizes the results for load to 3 mm of displacement, load to failure, displacement, and stiffness. The mean load to 3 mm of displacement was highest in the KT group, with significant differences among all 3 groups (Figure 3). Load to failure was significantly higher in the KT group as compared with the K2 group and the knotted group (P < .001), but there was no difference between the K2 and knotted groups (P ≥ .999) (Figure 4). Stiffness was highest in the KT group, and there were significant differences among all 3 groups. Displacement was higher in the KT group than the knotted group (P < .001), but there was no difference between the knotted and K2 groups (P = .552) or between the K2 and KT groups (P = .270).
Means Among the 3 Constructs (1 Knotted and 2 Knotless)

a All values expressed as mean ± SD. K2, knotless No. 2 suture; KT, knotless tape.

Load at 3 mm of displacement among constructs: knotted vs knotless No. 2 suture vs knotless suture tape. There were significant differences among all 3 groups. Values are presented as mean (line), SD (box), 95% CI (error bars), and outliers (circles).
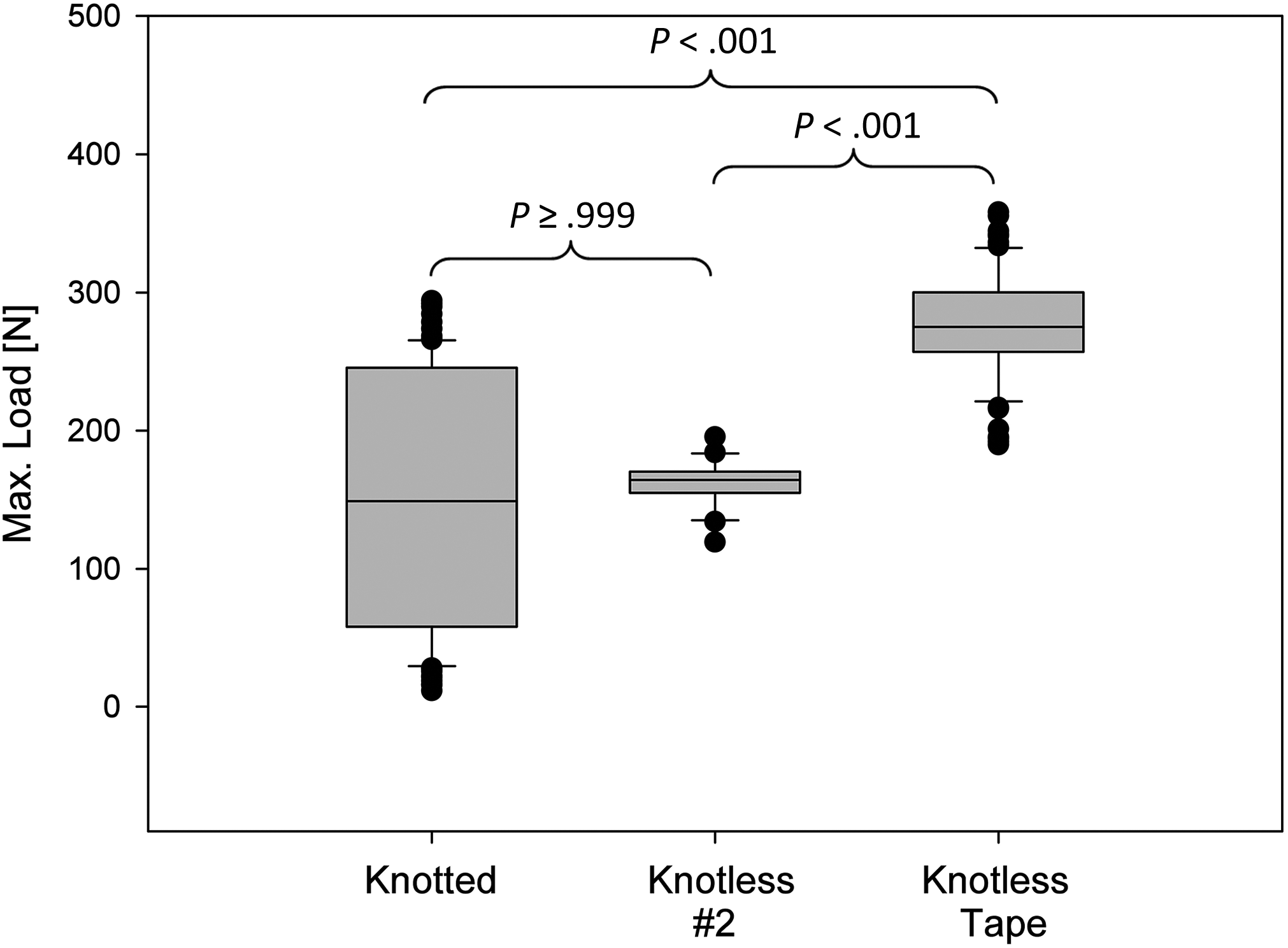
Maximum load to failure among constructs: knotted vs knotless No. 2 suture vs knotless suture tape. There were significant differences among all groups. Values are presented as mean (line), SD (box), 95% CI (error bars), and outliers (circles).
There was no difference in load at 3 mm of displacement, load to failure, stiffness, or displacement among attempts 1, 2, and 3 for each of the 3 constructs (P > .05).
Based on the F test, the variance in load to failure was significantly different between the knotted and knotless constructs. The knotted group demonstrated higher variability (SD = 94 N) than the KT (SD = 38 N) and K2 (SD = 17 N) groups (P < .001).
In the knotted group, the mode of failure was knot slippage in 56 (54%) cases, suture breakage in 30 (29%) cases, and eyelet breakage in 19 (18%) cases. In the K2 group, the mode of failure was suture slippage in 19 (90%) cases and anchor pullout in 2 (10%) cases. In the KT group, the mode of failure was suture slippage in 15 (19%) cases, anchor pullout in 63 (80%) cases, and foam block breakage in 1 (1%) case.
Discussion
The findings of this study support our hypothesis. Knotless fixation with suture tape showed higher loads to failure than a knotted or knotless No. 2 suture. Constructs with No. 2 suture were stronger in a knotless configuration. Additionally, the knotless constructs demonstrated less variability among surgeons. These findings may have important implications for maximizing fixation and reducing variability of suture constructs in rotator cuff repair.
In a bovine study, De Carli et al 6 reported that knotless fixation with tape had a significantly higher load to failure than knotted fixation with No. 2 suture. Likewise, in the current study, load to 3 mm of displacement and maximum load to failure were higher in the knotless constructs as compared with the knotted constructs. The load to 3 mm of displacement in the KT group was 220% higher than in the K2 group and 316% higher than in the knotted group. It was also interesting that the mode of failure was different among the constructs. The knotted constructs most commonly failed by knot slippage, whereas the knotless constructs failed by suture slippage in the K2 constructs and anchor slippage in the KT constructs. The latter likely reflects the greater thickness of the tape relative to the No. 2 suture, which provides improved interference fit between the bone and anchor. While this was an idealized environment that does not reflect tissue quality, the weak link in the knotless construct with tape was effectively anchor fixation.
Several studies have examined the biomechanical performance of knotless versus knotted suture bridge double-row rotator cuff repairs, and many have concluded that knots lead to greater strength. 5,12,15 However, because these double-row studies did not purely compare knotted versus knotless fixation, the comparisons were not equivalent. While both constructs were secured laterally with knotless fixation, the “knotted” constructs had additional medial fixation via mattress sutures, whereas the “knotless” constructs did not have medial fixation. In other words, the knotted constructs had additional points of fixation as compared with the knotless constructs. But when evaluation is isolated to fixation of the loop itself, as in the current study, a knotless method appears to exceed the strength of a knotted method. In addition to increased strength (knot security), a knotless construct may have improved loop security. As compared with the knotted group, the KT group had lower displacement, indicating that the KT constructs have a greater ability to maintain tissue contact, which has important implications for rotator cuff healing. 21 Based on these concepts, future suture-bridging constructs could be improved by using knotless methods to achieve additional medial fixation.
In addition to biomechanical strength, knotless constructs may be more reproducible. Some studies have compared different types of arthroscopic knots, 1,10,13 but few have evaluated the variance among surgeons in the ability to execute knots. Hanypsiak et al 9 evaluated the strength and consistency of knots tied by 73 expert arthroscopists and noted considerable variability of knots tied by an individual surgeon and among surgeons. Each arthroscopist tied 5 of the same knot: the SD of load to failure for an individual surgeon ranged from 6 N to 133 N between attempts, and 81% of the surgeons had at least 1 knot that was <80% strength of his or her strongest knot, indicating variability between knot attempts. Interestingly, among the surgeons in the study, volume of cases performed was not a factor. Mean load to failure was 231 N but ranged from 29 N to 360 N. Only 41% of surgeons were within 20% of the overall mean; in other words, there was broad variability among surgeons in knot strength. In contrast to Hanypsiak et al, 9 we found no statistically significant differences between attempts for any of the constructs within our study, which might be due to the decreased number of attempts per surgeon (3 vs 5). However, the mean load to failure also varied widely in the knotted group (mean, 149 N; range, 12-294 N), indicating high variability among surgeons. Among knotless constructs, not only was load to failure higher, but the variability among surgeons was also significantly reduced according to the F test analysis of SD. Based on these findings, knotless constructs appear to be stronger and more reproducible than knotted constructs.
Further examination of the biomechanical performance of the knotted and knotless constructs in the current study may be helpful for estimating the clinical acceptability of each construct. The maximum force generated across a 4-cm rotator cuff tear is estimated as 302 N. 4 With 2 double-loaded anchors, there are 6 fixation points—4 sutures and 2 tendon attachments (anterior and posterior tear margin)—resulting in a force of 50 N per fixation point. In this model, 50 N is therefore the minimum threshold for each loop that would be acceptable for load at 3 mm of displacement (clinical failure). Using this model, 100% of the KT constructs, 98% (49 of 50) of the K2 constructs, and 82% (65 of 79) of the knotted constructs would have been acceptable in our study. The aforementioned 302 N is based on a maximum force per unit area of 3.5 kg/cm2. As previously published literature 11,14 has also reported higher values—including values distributed to ≤8 kg/cm2 and a mean of 9.2 kg/cm2 for men and 7.1 kg/cm2 for women—a safety factor was applied for the load-to-failure threshold of double the initial value, to 100 N. With these 2 criteria, an acceptability threshold emerges that appears to favor knotless constructs (Figure 5). While the number of fixation points can be varied via additional anchors or additional sutures per anchor, the knotless constructs appear to achieve fixation in a more technically efficient manner (ie, fewer suture passes and fewer knots).

Acceptability of the knotted and knotless constructs based on 50 N for load at 3 mm of displacement and 100 N for maximum load to failure.
The major strength of this study is the analysis of knotted versus knotless constructs among multiple surgeons. This provides a “real world” of constructs performed by most orthopaedic surgeons and allowed an assessment of variability. Nonetheless, there are several limitations. First, the study is biomechanical and does not take into account other factors that affect rotator cuff healing (eg, tendon quality), but this was not the intention of testing. With the exclusion of human factors, the results are more reproducible and the different constructs easier to compare. Second, the knots were tied in a dry environment. A previous study suggested that a wet environment, as seen in arthroscopy, improves knot properties. 17 Third, in our study (similar to Hanypsiak et al 9 ), only the initial fixation strength was examined, by applying an axial force to the construct. Both constitute further limitations to this study, as cyclic loading and angled force application may be more representative of stresses on a rotator cuff repair. Moreover, we did not assess surgeon factors that may affect knot tying, such as volume and experience, but all participants were orthopaedic shoulder surgeons who routinely perform rotator cuff repairs. Finally, we did not control the type of knots tied by the surgeons, which may have influenced the results. Differences based on knot type were previously evaluated 13 but were not part of this study.
Conclusion
Knotless fixation with suture tape had improved biomechanical performance as compared with knots or knotless fixation with No. 2 suture. In addition, knotless fixation had less variability in biomechanical properties among multiple surgeons. This study may be relevant for surgeons choosing between knotted and knotless constructs as well as for considerations in design of rotator cuff repair constructs.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded with research support from Arthrex. P.J.D. is a consultant for Arthrex and Integer, is a paid speaker/presenter for Arthrex, receives royalties from Arthrex and Lippincott Williams & Wilkins, and receives research support from Arthrex. C.R.A., N.C.F., M.P., and C.A.W. are employees of Arthrex.
Ethical approval was not sought for the present study.