
Abstract
Background:
Traumatic anterior shoulder dislocations in young adults often result in Bankart lesions, which contribute to recurrent instability. Arthroscopic Bankart repair is a commonly utilized and well-established treatment option that employs either knot-tying or knotless suture anchors. While knot-tying suture anchors allow for customizable tensioning and have demonstrated strong fixation, they require technical expertise and may be associated with complications related to knots. Knotless anchors offer a simplified technique and eliminate knot-related issues, although they may provide less intraoperative adjustability.
Purpose:
To compare the clinical outcomes of knot-tying and knotless suture anchors in arthroscopic Bankart repair for anterior shoulder instability.
Study Design:
Systematic review and meta-analysis; Level of evidence, 3.
Methods:
PubMed, Scopus, and Ovid Medline databases were searched up to January 2025. The inclusion criteria encompassed comparative studies (levels 1-3) reporting redislocation rates, revision rates, patient-reported outcomes, or range of motion. Data were independently extracted and quality assessed using the Methodological Index for Non-Randomized Studies and the Modified Coleman Methodology Score criteria. Statistical analyses utilized fixed- or random-effects models based on heterogeneity.
Results:
Ten studies comprising 793 patients—415 in the knot-tying group and 378 in the knotless group (mean age, 21.1-32.6 years)—met the inclusion criteria. Redislocation rates were 9.5% and 10.6% for knot-tying and knotless anchors, respectively, with no significant difference (odds ratio [OR], 0.95; P = .83). Revision rates (7.8% vs 6.7%) and Rowe scores (mean difference [MD], 2.09 [95% CI, –0.72 to 4.90]; P = .14) showed no statistical disparity. Knot-tying anchors demonstrated lower visual analog scale pain scores (MD, –0.31; P = .001). Range of motion, including external rotation and forward flexion, was comparable between groups.
Conclusion:
Knot-tying and knotless suture anchors yield similar outcomes for arthroscopic Bankart repair regarding redislocation, revision rates, and functional recovery. Knot-tying anchors may slightly reduce pain; however, the magnitude of this difference appears to be below the threshold for clinical importance. Both techniques are viable, allowing surgeons to base their choice on preference and case specifics.
Traumatic anterior shoulder dislocations are particularly prevalent in young, active individuals, with incidence rates ranging from 23.9 per 100,000 person-years in the general population to as high as 435 per 100,000 in military cadets, highlighting a significantly greater burden in high-risk populations such as athletes and military personnel. 4 Traumatic anterior shoulder dislocation is typically associated with structural injuries such as anteroinferior labral tears (Bankart lesions), anterior glenoid rim fractures, bone defects, capsular tears, inferior glenohumeral ligament injuries, and Hill-Sachs lesions, with Bankart lesions reported in up to 97% of cases and representing the most prevalent pathology.26,27,30 The treatment of choice for anterior shoulder instability, particularly in cases at high risk for recurrence, is surgical stabilization, commonly referred to as Bankart repair. Historically, this procedure was performed through open surgery. 7 However, the arthroscopic approach has become the most commonly employed technique for Bankart repair in modern clinical practice. 1 Suture anchors are the preferred implants for reattaching the anteroinferior labrum or Bankart lesion to the anterior glenoid, ensuring optimal stabilization.
The 2 primary types of suture anchors are those with a knot-tying mechanism and those with a knotless mechanism (Figure 1), each with distinct advantages and disadvantages. Knot-tying suture anchors are advantageous because of their familiarity among surgeons. However, their use requires advanced technical proficiency for secure knot tying, as the construct’s strength heavily depends on the quality of the knots. 21 Furthermore, the presence of knots poses a risk of cartilage irritation, 29 which may lead to postoperative complications. On the other hand, knotless suture anchors offer an easier surgical technique and feature a knotless design that minimizes the risk of cartilage irritation. The strength of the construct in knotless systems is determined by the anchor itself rather than by the quality of knots, potentially providing a more consistent repair with a different technical approach for the surgeon. 25
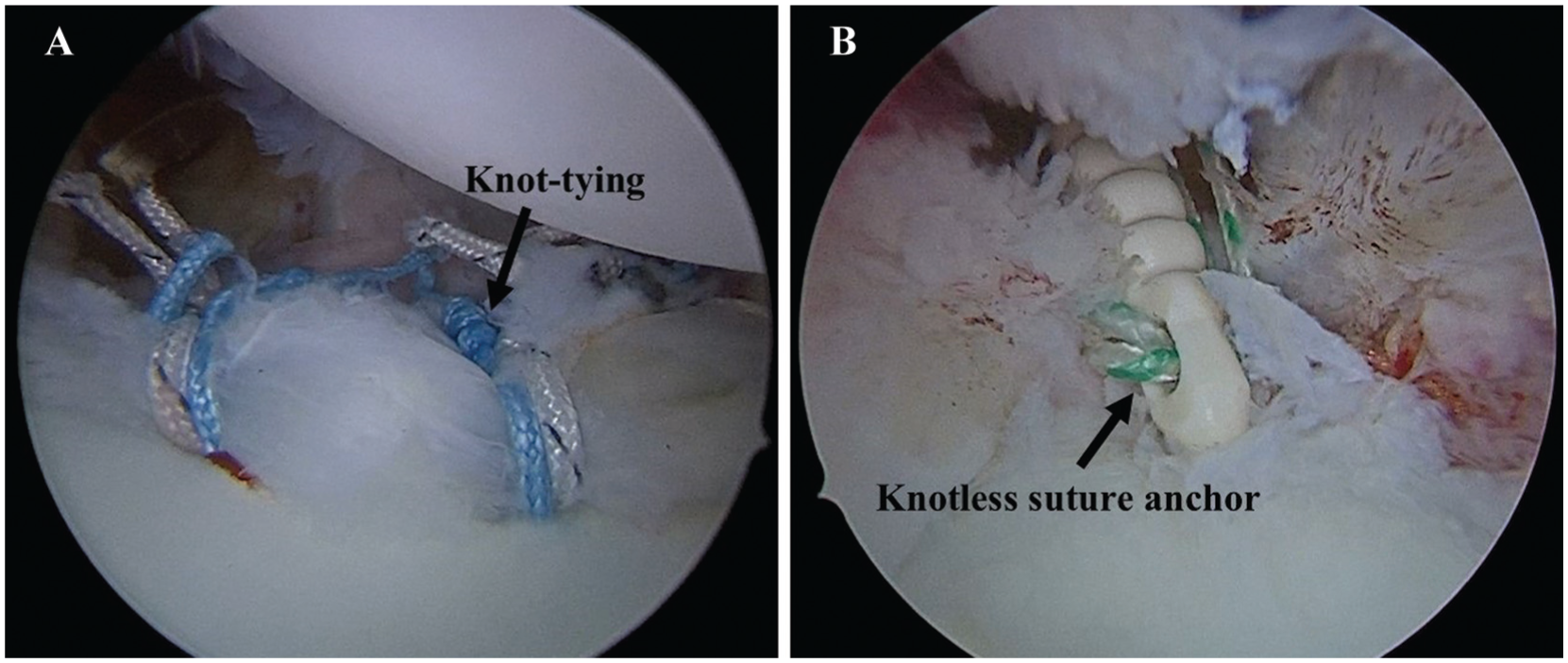
Right shoulder, lateral decubitus position. Arthroscopic view from the posterior portal showing (A) Bankart repair performed using the knot-tying technique with all-suture anchors (Y-Knot Flex, Conmed), and (B) Bankart repair performed using the knotless technique with knotless suture anchors (MINI-VIM PK, Biotek).
A biomechanical study has demonstrated that knot-tying and knotless suture anchors exhibit similar stiffness and load-to-failure properties. 19 Failure in both knot-tying and knotless suture anchors is more frequently attributed to cut-through at the suture-tissue interface rather than anchor pull-out from the bone.9,20 Clinical studies have reported varying results regarding the use of knot-tying and knotless suture anchors in arthroscopic Bankart repair. Some studies have shown a higher rate of recurrent dislocations with knotless anchors, while others have found a higher redislocation rate with knot-tying anchors.5,15 However, some studies report similar outcomes between the 2 techniques.2,11,18,22,23,31 To date, there is no definitive consensus on the superiority of either method.
This study aimed to compare the clinical outcomes of knot-tying and knotless suture anchors in arthroscopic Bankart repair for anterior shoulder instability. The primary outcome was the redislocation rate, with secondary outcomes including the revision rate, patient-reported outcome scores, and range of motion. The authors hypothesized that knot-tying and knotless suture anchors may yield similar redislocation rates, revision rates, and clinical outcomes.
Methods
Search Strategies
This systematic review was conducted in accordance with the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and registered with PROSPERO (International Prospective Register of Systematic Reviews) (registration No. CRD42025632395). Two authors (N.T. and T.I.) independently performed a search of the Scopus, PubMed, and Ovid Medline databases in January 2025. Studies from inception to January 2025 that reported redislocation rates, revision rates, patient-reported outcome scores, or postoperative range of motion were included. The search terms used in Scopus and PubMed were as follows: ("knotted" OR "knot-tying") AND ("knotless" OR “Pushlock”) AND ("Bankart" OR "labrum" OR “shoulder instability” OR “shoulder dislocation”). For Ovid Medline, the same search terms were used, along with additional filters, to limit the results to studies in English, full-text articles, and research focused on human subjects.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows:
Clinical comparative studies with evidence levels of 1 to 3.
Published in English.
Directly evaluated outcomes of knot-tying versus knotless suture anchors for arthroscopic Bankart repair.
Reported postoperative redislocation rates, revision rates, patient-reported outcome scores, or range of motion.
Full-text articles were accessible.
The exclusion criteria were as follows:
Case series, case reports, or review articles.
Basic science or biomechanics research.
Data Extraction
Two authors (N.T. and T.I.) independently extracted data based on the study protocol, focusing on study design, patient characteristics, surgical techniques, and implants used, as well as postoperative outcomes. In studies with a parallel design involving multiple arms, only data from the arm where patients underwent anterior labral repair were included.
Methodological Quality Assessment
Two independent authors (N.T. and T.I.) assessed the methodological quality of the included studies using the Methodological Index for Non-Randomized Studies (MINORS) criteria, which has an ideal score of 24 points for nonrandomized comparative studies, and the Modified Coleman Methodology Score (MCMS), which has a maximum score of 100 points. In cases of disagreement, the 2 authors discussed the issue, and if necessary, a third author (D.L.) was consulted to resolve the disagreement.
Statistical Analysis
Statistical analysis was conducted using RevMan software Version 5.4.1. A meta-analysis was performed if ≥3 studies evaluated the same outcome. Heterogeneity was assessed using the I2 statistic test, and P < 0.1 indicated significant heterogeneity. When heterogeneity was present, a random-effect model was applied; otherwise, a fixed-effect model was used. For continuous outcomes, the mean difference (MD) and its corresponding 95% CI were calculated. For dichotomous outcomes, the odds ratio (OR) and its corresponding 95% CI were calculated. The forest plot was used to illustrate the pooled estimates and their corresponding CIs for each study, providing a visual representation of the effect sizes and the overall meta-analysis results.
Results
Included Studies
The initial search identified 319 articles. After removing duplicates, 228 unique articles remained and were independently screened for titles and abstracts by 2 authors (N.T. and T.I.). Of these, 214 records were excluded. The full texts of the remaining 14 articles were reviewed, resulting in the exclusion of 4 additional records. Consequently, 10 studies met the inclusion criteria and were deemed eligible for meta-analysis. These included 2 studies classified as level 1 evidence, 3 as level 2 evidence, and 5 as level 3 evidence. The selection process is comprehensively outlined in the accompanying PRISMA flowchart (Figure 2)

The PRISMA flowchart of the selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
A total of 793 patients were included in the analysis. The sample size of individual studies ranged from 11 38 to 10 122 patients with anterior shoulder instability. The mean age of patients varied from 18 21.1 to 12 32.6 years. The mean follow-up duration ranged from 12 months 3 to 4.8 years. 31 The methodological quality of the included studies, as assessed by the MINORS score (ranging from 3 12 to15,18 21) and the MCMS score (ranging from 3 58 to12,18,22 82), indicated that the overall quality was fair to good (Table 1 and Appendix Table A1).
Details of the Included Studies a

ASES, American Shoulder and Elbow Surgeons; DASH, Disabilities of the arm, shoulder, and hand; ER, external rotation; FF, forward flexion; FU, Follow-up; IR, internal rotation; LOE, level of evidence; MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-randomized Studies; NR, not reported; Preop, preoperative; RAND 12 Item Health Survey; SANE, Single Assessment Numeric Evaluation; UCLA, University of California-Los Angeles; UEFS, Upper Extremity Functional Score; VAS, visual analog scale; VR-12, Veterans; WOSI, Western Ontario Shoulder Instability Index.
Redislocation Rates
Nine studies5,10-12,15,18,22,23,31 examined redislocation rates in the knot-tying and knotless groups. The overall redislocation rates were 9.5% (36/380 patients) in the knot-tying group and 10.6% (37/349 patients) in the knotless group. The I2 test showed a P-value of 0.29 and an I2 of 17%, indicating no statistically significant heterogeneity; therefore, the fixed-effect model was used. The pooled meta-analysis demonstrated no statistically significant difference in the overall redislocation rates between the 2 groups (OR, 0.95 [95% CI, 0.57 to 1.57]; P = .83) (Figure 3A).

The forest plot shows the pooled meta-analysis of (A) redislocation rates and (B) revision rates for knot-tying and knotless suture anchors in arthroscopic Bankart repair. M-H, Mantel-Haenszel.
Revision Rates
Seven studies5,10,11,15,18,22,31 examined revision rates in the knot-tying and knotless groups. The overall revision rates were 7.8% (23/295 patients) in the knot-tying group and 6.7% (18/268 patients) in the knotless group. The I2 test showed a P value of 0.10 and an I2 of 44%, indicating statistically significant heterogeneity; therefore, the random-effect model was used. The pooled meta-analysis revealed no statistically significant difference in overall revision rates between the 2 groups (OR, 1.09 [95% CI, 0.35-3.37]; P = .88) (Figure 3B).
Patient-Reported Outcome Scores
The outcome measures included the Rowe score, visual analog scale (VAS) for pain, Constant score, American Shoulder and Elbow Surgeons score, Single Assessment Numeric Evaluation, Disabilities of the Arm, Shoulder, and Hand score, University of California–Los Angeles score, Western Ontario Shoulder Instability Index, and Upper Extremity Functional Score. Only the Rowe score and VAS for pain were reported in ≥3; thus, the authors included these 2 patient-reported outcome scores in the pooled meta-analysis. Six studies5,11,12,22,23,31 reported the Rowe score at the final follow-up, and 6 studies3,5,12,18,23,31 reported the VAS for pain.
Six studies5,11,12,22,23,31 reported the Rowe score at the final follow-up for both the knot-tying and knotless groups. The I2 test showed a P value of 0.36 and an I2 of 7%, indicating no statistically significant heterogeneity; therefore, a fixed-effect model was used. The pooled meta-analysis revealed no statistically significant difference in the Rowe score at the final follow-up between the 2 groups (MD, 2.09 [95% CI, –0.72 to 4.90]; P = .14) (Figure 4A).
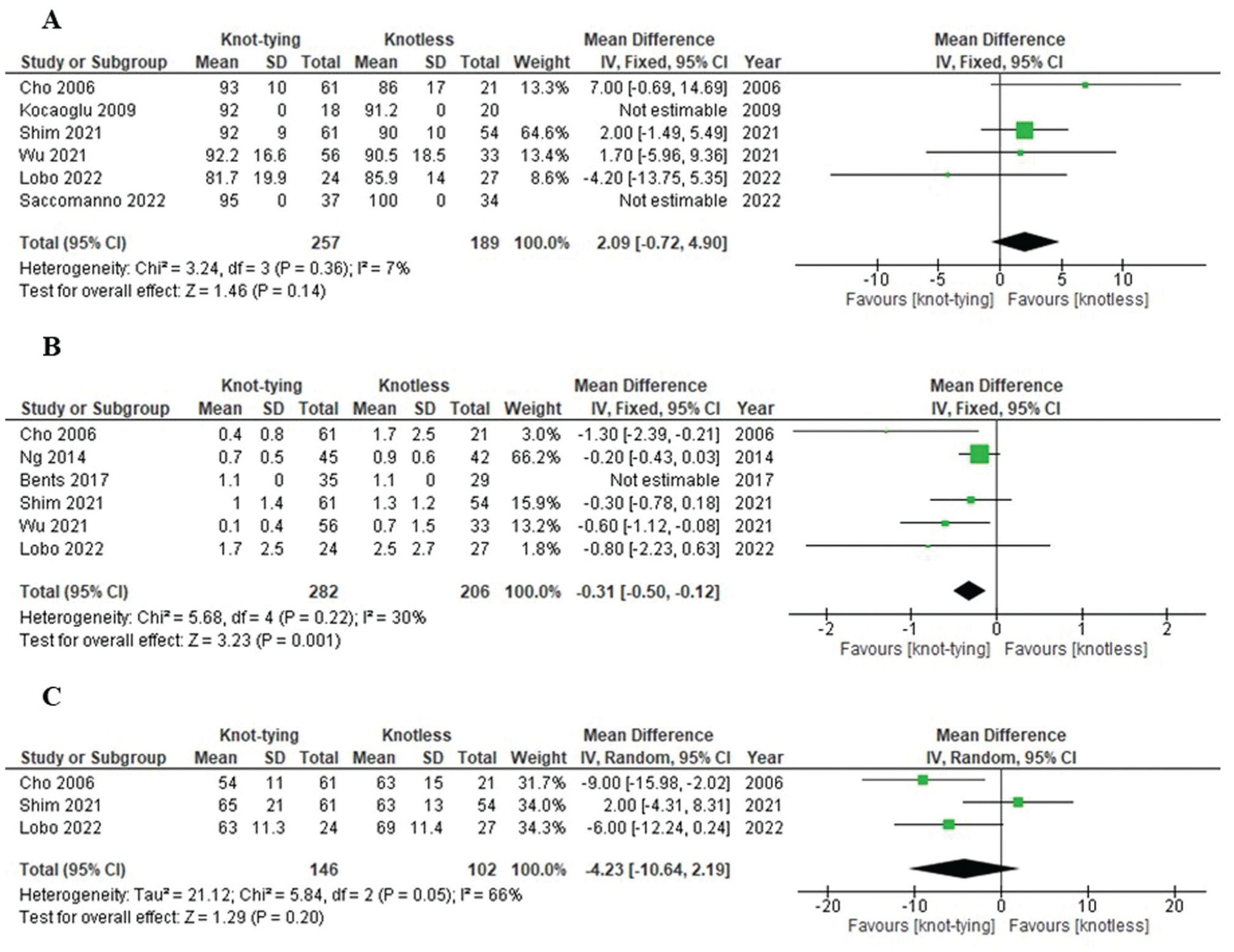
The forest plot shows the pooled meta-analyses of (A) the Rowe score, (B) the VAS for pain, and (C) external rotation for knot-tying and knotless suture anchors in arthroscopic Bankart repair. IV, inverse variance; VAS, visual analog scale.
Six studies3,5,12,18,23,31 reported the VAS for pain at the final follow-up for both the knot-tying and knotless groups. The I2 test showed a P value of 0.22 and an I2 of 30%, indicating no statistically significant heterogeneity; therefore, a fixed-effect model was used. The pooled meta-analysis demonstrated a statistically significant difference in the VAS for pain at the final follow-up, with the knot-tying group reporting lower pain scores compared with the knotless group (MD, –0.31 [95% CI, –0.50 to −0.12]; P = .001) (Figure 4B).
Two studies12,15 reported Western Ontario Shoulder Instability Index (WOSI) scores at the 24-month follow-up. Lobo et al 12 found mean WOSI scores of 509.2 ± 480.1 in the knotted anchor group and 555.9 ± 393.6 in the knotless group, with no statistically significant difference between groups (P = .533). In contrast, Minkus et al 15 reported a significantly higher median WOSI score in the knotless anchor group (95%) compared with the all-suture anchor group (81%), with adjusted regression analysis confirming a significant difference favoring the knotless technique. These findings suggest a potential variation in WOSI score depending on the anchor type, although pooled analysis was not feasible due to the limited number of studies.
Range of Motion
The range of motion measures included external rotation, internal rotation, and forward flexion. Only external rotation was reported in ≥3 studies; thus, the authors included it in the pooled meta-analysis. Three studies5,12,23 reported external rotation at the final follow-up for both the knot-tying and knotless groups. The I2 test showed a P value of .05 and an I2 of 66%, indicating statistically significant heterogeneity; therefore, a random-effects model was used. The pooled meta-analysis revealed no statistically significant difference in external rotation at the final follow-up between the 2 groups (MD, –4.23 [95% CI, –10.64 to 2.19]; P = .20) (Figure 4C).
Two studies5,23 evaluated postoperative forward flexion at the final follow-up, both finding no statistically significant differences between techniques. Cho et al 5 reported forward flexion of 172°± 5° for the knot-tying technique and 174°± 5° for the knotless technique. Similarly, Shim et al 23 observed forward flexion of 164°± 8° with knot-tying and 165°± 8° with knotless.
Two studies12,23 assessed postoperative internal rotation at the side (0° abduction) at the final follow-up. Shim et al 23 reported internal rotation of 12.2°± 2.3° for the knot-tying technique and 11.8°± 2° for the knotless technique, with no statistically significant difference. Similarly, Lobo et al 12 observed internal rotation of 8°± 1.9° for knot-tying and 7°± 2.2° for knotless, also showing no statistically significant difference.
Discussion
The primary outcome of this study, redislocation rates, was similar between the knot-tying and knotless groups, at 9.5% and 10.6%, respectively, with no statistically significant difference. Similarly, secondary outcomes, including revision rates, Rowe scores, and external rotation at the final follow-up, showed no statistically significant differences between the groups. However, the knot-tying group demonstrated a statistically significant reduction in VAS pain scores, with an MD of 0.31. Nevertheless, this difference is marginal and may lack clinical significance.
The redislocation rate after surgery is a critical outcome, as recurrent shoulder dislocation is the primary indication for surgical intervention. Reports in the literature6,28 indicated that postsurgical redislocation rates ranged between 6.7% and 9.6%. Some studies have reported high rates of redislocation after the use of knotless suture anchors in arthroscopic Bankart repairs. Nattfogel and Ranebo 17 reported a study investigating redislocation rates after arthroscopic Bankart repair using a knotless anchor technique in patients with anterior shoulder instability. Among 73 shoulders (from 70 patients) observed for a mean of 7.5 years, a redislocation rate of 15% was noted. Cho et al 5 reported a study comparing redislocation rates after arthroscopic Bankart repair using knot-tying versus knotless suture anchors. Among 61 patients in the knot-tying group, the redislocation rate was 4.9%, whereas it was statistically significantly higher at 23.8% among 21 patients in the knotless group. However, Minkus et al 15 reported that the redislocation rate was higher in the knot-tying group at 16.7%, compared with a statistically significantly lower rate of 3.2% in the knotless group. 15 Nevertheless, multiple studies have reported that redislocation rates are similar between knot-tying and knotless methods.2,11,18,22,23,31 In this study, a pooled meta-analysis of 9 studies was conducted, revealing redislocation rates at mid-term follow-up of 9.5% in the knot-tying group and 10.6% in the knotless group, with no statistically significant difference between the 2. These findings align with biomechanical studies indicating that both knotless and knot-tying anchors predominantly fail due to cut-through at the suture-tissue interface rather than anchor pull-out from the bone. 20 Thus, the anchor type may not play a significant role in failures.
In terms of revision rates, some cases of clinical instability may not require revision surgery. 32 However, severe cases, multiple redislocations, or additional indications such as a painful or stiff shoulder often necessitate surgical intervention.14,33 The outcomes reported in previously published studies have been mixed. For example, Cho et al 5 found that patients in the knotless group were more likely to require revision surgery (2% in the knot-tying group vs 19% in the knotless group). In contrast, Wu et al 31 reported higher revision rates in the knot-tying group (18%) compared with the knotless group (3%). In the present study, the revision rates between the 2 groups were not statistically different, with 7.8% (23/295 patients) in the knot-tying group and 6.7% (18/268 patients) in the knotless group. These findings suggest that the likelihood of revision surgery is similar between knot-tying and knotless techniques.
Patient-reported outcomes are critical in assessing the success of surgical interventions from the patient’s perspective.8,13 In this study, no statistically significant difference was observed in Rowe scores between the knot-tying and knotless suture anchor techniques. However, the VAS for pain revealed slightly lower scores in the knot-tying group compared with the knotless group, with an MD of 0.31. While this difference was statistically significant, it was marginal and fell far below the minimal clinically significant difference for VAS pain in shoulder conditions, previously established 24 at 2.4. This finding highlights that, even with a slight statistical advantage, the 2 techniques provide nearly the same pain relief in clinical practice. Both knot-tying and knotless methods deliver comparable levels of pain reduction and functional improvement. These results suggest that either approach can be utilized to achieve favorable, patient-reported outcomes in clinical practice.
Cho et al 5 found no statistically significant difference in external rotation between knot-tying and knotless anchors, although the knot-tying group exhibited a slight postoperative decrease. Similarly, Lobo et al 12 and Shim et al 23 reported comparable outcomes for external rotation, with both techniques demonstrating similar restoration of motion. In terms of forward flexion, Cho et al 5 observed no statistically significant difference between knot-tying (172°) and knotless (174°) anchors, while Shim et al 23 reported similar outcomes, with 164° in the knot-tying group and 165° in the knotless group. For internal rotation, Lobo et al 12 found no statistically significant difference, with the knot-tying group achieving a mean of 8° and the knotless group a mean of 7°, while Shim et al 23 reported similar results, with the knot-tying group reaching 12.2° and the knotless group reaching 11.8°. The present study found no statistically significant differences in range of motion between the knot-tying and knotless suture anchor groups. Both techniques facilitated comparable restoration of shoulder mobility, including external rotation, internal rotation, and forward flexion. Preserving range of motion is crucial for maintaining the overall functionality of the shoulder joint. 16 The equivalence between these 2 methods suggests that surgeons can confidently select either technique without compromising postoperative mobility.
Some studies have shown large differences between knot-tying and knotless anchors, which may be attributed to small sample sizes, variations in surgical technique, and patient characteristics. When combined in this meta-analysis, these factors averaged out across a larger, more diverse population, resulting in more consistent overall outcomes. Differences in surgeon experience and anchor design may also have influenced the isolated results, but had a less significant effect on the pooled analysis.
The findings of this study have important implications for clinical practice. Given the similar rates of redislocation, revision, patient-reported outcomes, and range of motion outcomes, the choice between knot-tying and knotless suture anchors can be based on surgeon preference, familiarity with the technique, and specific clinical scenarios. Knotless anchors may offer advantages in terms of reduced operative time and simplified knot management, potentially decreasing the risk of knot-related complications. Conversely, knot-tying methods may provide more tactile feedback during surgery, which some surgeons might prefer for achieving precise knots and soft tissue tension.
Limitations
Despite the comprehensive nature of this review, several limitations must be acknowledged. This study is limited by the relatively small number of available studies included in the analysis, especially concerning most secondary outcome measures. The scarcity of data on these secondary endpoints restricts the ability to perform comprehensive analyses and may limit the generalizability of the findings. The included studies varied in their methodological quality, with some presenting risks of bias that could affect the reliability of the results. Additionally, heterogeneity in surgical techniques, postoperative rehabilitation protocols, and follow-up durations across studies may have influenced the pooled outcomes. Most studies have focused on short- to medium-term results, limiting our understanding of the long-term efficacy and potential late complications associated with each anchor type. Several included studies reported follow-up periods of ≤1, which may be inadequate to capture the true incidence of redislocation. This short follow-up duration represents a significant limitation and may underestimate recurrence rates, thereby affecting the robustness of conclusions drawn regarding long-term outcomes. Furthermore, the lack of standardized reporting on certain variables, such as specific patient-reported outcome measures and a detailed range of motion assessments, hindered the ability to perform more granular analyses. However, given the limitations identified, further high-quality, randomized controlled trials with standardized protocols and long-term follow-up are necessary to confirm these results and explore potential differences in specific patient subgroups.
Conclusion
Knot-tying and knotless suture anchors yield similar outcomes for arthroscopic Bankart repair regarding redislocation, revision rates, and functional recovery. Knot-tying anchors may slightly reduce pain; however, the magnitude of this difference appears to be below the threshold for clinical importance. Both techniques are viable, allowing surgeons to base their choice on preference and case specifics.
Footnotes
Appendix
Details of the Included Studies, Inclusion and Exclusion Criteria, Patient Characteristics, and Surgical Techniques a

| Lead Author (Year) | Inclusions | Exclusions | Patient Characteristics | Surgical Technique (Knot-Tying) | Surgical Technique (Knotless) |
|---|---|---|---|---|---|
| Cho (2006) | - Patients with a Bankart lesion with a good remaining labrum | - Bony Bankart lesion - ALPSA lesion - HAGL lesion - Associated SLAP lesion - Rotator cuff tear or rotator cuff fibrillation - Poor labrum - Hyperlaxity |
Glenoid track: NR preoperative Rowe score (knot-tying/ knotless): 45.3 ± 10.7/42.1 ± 10.3 |
Position: beach chair Anchors: mini-Revo suture anchors (Linvatec) No. of anchors: 3.12 Suture configuration: simple stitch Remplissage: NR |
Position: beach chair Anchors: metal body with 2 prongs, knotless Anchor (Mitek) No. of anchors: 3.05 Suture configuration: loop stitch Remplissage: NR |
| Kocaoglu (2009) | - Patients with traumatic anterior shoulder instability - Bankart lesion - ALPSA lesion |
- Bony Bankart lesion - HAGL lesion |
Glenoid track: on-track Preoperative Rowe score (knot-tying/ knotless): 41 (range, 38-44)/ 43 (range, 40-48) |
Position: beach chair Anchors: single-loaded suture anchor No. of anchors: NR Suture configuration: simple stitch Remplissage: not performed |
Position: beach chair Anchors: 3.5 mm PushLock anchor (Arthrex) No. of anchors: NR Suture configuration: simple stitch Remplissage: not performed |
| Ng (2014) | - Patients with traumatic anterior shoulder instability - Bankart lesion - Fail nonoperative treatment - Surgery within 6 weeks of the last dislocation |
- First-time dislocation - Bony Bankart lesion - HAGL lesion - Associated SLAP lesion - Rotator cuff tear - Off-track Hill-Sachs lesion |
Glenoid track: on-track Preoperative Rowe score (knot-tying/ knotless): NR |
Position: beach chair Anchors: single-loaded suture anchor No. of anchors: 4 (range, 3-5) Suture configuration: simple stitch Remplissage: not performed |
Position: beach chair Anchors: PushLock anchor (Arthrex No. of anchors: 4 (range, 3-5) Suture configuration: simple stitch Remplissage: not performed |
| Bents (2017) | - Underwent primary isolated arthroscopic anterior labrum repair - Minimum 1-year follow-up |
- Hybrid knotted–knotless repair - Rotator cuff tear - Revision - Open surgery - Lack of complete follow-up data |
Glenoid track: NR Preoperative Rowe score (knot-tying/ knotless): NR |
Position: NR Anchors: NR No. of anchors: 2.8 Suture configuration: NR Remplissage: NR |
Position: NR Anchors: NR No. of anchors: 3.1 Suture configuration: NR Remplissage: NR |
| Shim (2021) | - Patients with traumatic anterior shoulder instability - Bankart lesion |
- Bony Bankart lesion - Glenoid bone loss >20% - Rotator cuff tear - HAGL lesion - Revision - Follow-up <2 years |
Glenoid track: NR Preoperative Rowe score (knot-tying/ knotless): 38 ± 20/33 ± 17 |
Position: semi-lateral decubitus Anchors: double-loaded SutureTak (Arthrex) or Bio Mini-Revo (Linvatec) No. of anchors: 3.8 ± 0.6 Suture configuration: mattress stitch or simple stitch Remplissage: performed in cases (knot-tying, 21%) |
Position: semi-lateral decubitus Anchors: PushLock anchor (Arthrex) No. of anchors: 4 ±0.3 Suture configuration: simple stitch Remplissage: performed in cases (knotless, 46%) |
| Wu (2021) | - Patients with recurrent anterior shoulder instability - Underwent primary isolated arthroscopic Bankart repair |
- Revision - Open surgery - Capsular plication - Anterior capsulorrhaphy without suture anchor - Worker's compensation - Latarjet procedure - <2 dislocations |
Glenoid track: off-track knot-tying, 10%/ knotless, 15% Preoperative Rowe score (knot-tying/ knotless): NR |
Position: beach chair Anchors: SutureTak anchor (Arthrex) No. of anchors: 2.3 ± 0.1 Suture configuration: mattress stitch Remplissage: NR |
Position: beach chair Anchors: PushLock anchor (Arthrex) No. of anchors: 3.3 ± 0.1 Suture configuration: simple stitch Remplissage: NR |
| Lobo (2022) | - Skeletal maturity - Anterior shoulder instability - Anterior labral lesions with glenoid bone defects occur up to 13.5%, rising to 20% when the ISIS is <4. |
- Epilepsy - Rotator cuff tear - Proximal humerus fracture - Multidirectional or posterior instability - Beighton score ≥ 4 - Irreparable anterior capsule damage - HAGL lesion - Concomitant procedures - Previous surgery - Advanced glenohumeral arthrosis (grades 2 and 3 by Samilson and Pietro) |
Glenoid track: off-track knot-tying, 3.7%/ knotless, 13% Preoperative Rowe score (knot-tying/ knotless): 28.1 ± 11.3/28.9 ± 10.9 |
Position: lateral decubitus Anchors: SutureTak anchor (Arthrex) No. of anchors: 3.0 ± 0.2 Suture configuration: simple stitch Remplissage: not performed |
Position: lateral decubitus Anchors: PushLock anchor (Arthrex) No. of anchors: 2.9 ± 0.3 Suture configuration: cinch stitch Remplissage: not performed |
| Saccomanno (2022) | - Aged > 18 years - Patients with recurrent anteroinferior shoulder instability |
- Instability without dislocation - Multidirectional or posterior instability - Glenoid bone loss >20% - Off-track lesion - Bony Bankart lesion - Rotator cuff tear - Previous surgery - Infection - Congenital or acquired inflammatory or neurologic diseases (systemic or local) involving the shoulder - Unwillingness to sign the informed-consent form |
Glenoid track: on-track Preoperative Rowe score (knot-tying/ knotless): median, 35/35 |
Position: lateral decubitus Anchors: Bio-FASTak anchor (Arthrex) No. of anchors: median, 3 Suture configuration: NR Remplissage: not performed |
Position: lateral decubitus Anchors: PushLock anchor (Arthrex) No. of anchors: median, 3 Suture configuration: NR Remplissage: not performed |
| Johnson (2023) | - Patients with anteroinferior labral tear - Repair with all knot-tying or all knotless anchors |
- Open surgery - Posteroinferior or SLAP repair or capsular shift only |
Glenoid track: NR Preoperative Rowe score (knot-tying/ knotless): NR |
Position: lateral decubitus Anchors: NR No. of anchors: 3 ± 0.76 Suture configuration: simple stitch Remplissage: NR |
Position: lateral decubitus Anchors: NR No. of anchors: 2.98 ± 0.61 Suture configuration: simple stitch Remplissage: NR |
| Minkus (2024) | - Aged 18- 40 years - Patients with recurrent anteroinferior shoulder instability - Fail nonoperative treatment |
- First-time dislocation - Previous surgery - Significant bony glenoid defect - Rotator cuff tear - Neuromuscular disease - Drug or alcohol abuse - Worker's compensation - Irreversible muscle damage - Inflammatory arthritis - Immunosuppressed or autoimmune disorder - Infection |
Glenoid track: off-track knot-tying, 0%/ knotless, 6.5% Preoperative Rowe score (knot-tying/ knotless): median, 15/15 |
Position: lateral decubitus Anchors: Juggerknot anchors (Zimmer Biomet) No. of anchors: 3 Suture configuration: mattress stitch Remplissage: performed in off-track cases (knot-tying, 0%) |
Position: lateral decubitus Anchors: PushLock anchor (Arthrex) No. of anchors: 3 Suture configuration: cinch stitch Additional Remplissage: in cases of off-track Hill Sachs lesions (2 patients, 6.5%) Remplissage: performed in off-track cases (knotless, 6.5%) |
ALPSA, anterior labral periosteal sleeve avulsion; HAGL, humeral avulsion of the glenohumeral ligament; ISIS, instability severity index score; NR, not reported; Preop, preoperative; SLAP, superior labrum anterior to posterior.
Acknowledgements
The authors thank the Thai Orthopedic Society for Sports Medicine for their academic support.
Correction (December 2025):
This article has been updated to correct the article type to “Review.”
Final revision submitted May 28, 2025; accepted July 15, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
The data that support the findings of this study are available on request from the corresponding author.