
Abstract
Background:
Decreases in Medicare reimbursement have been noted among many medical specialties. An in-depth analysis of the subspecialty of orthopaedic sports medicine is needed to determine changes in Medicare reimbursement in this field.
Purpose/Hypothesis:
The purpose was to elucidate the trends in inflation-adjusted Medicare reimbursement for orthopaedic sports medicine procedures between 2000 and 2020. It was hypothesized that Medicare reimbursement decreased substantially during the study period.
Study Design:
Economic decision and analysis; Level of evidence, 4.
Methods:
The Physician Fee Schedule Look-up Tool was used to extract Medicare reimbursement information between 2000 and 2020 for 67 procedures related to orthopaedic sports medicine. These values were adjusted for inflation using the Consumer Price Index. The compound annual growth rate (CAGR) was calculated to measure the annual rate of change, and descriptive analyses were performed using the Student t test.
Results:
Between 2000 and 2020, inflation-adjusted Medicare reimbursement for the 67 included procedures decreased by an average of 33% (CAGR = –2.2%; R 2 = 0.78). Reimbursement decreased for procedures related to the shoulder and elbow by 34% (CAGR = –2.3%; R 2 = 0.80), for hip-related procedures by 23% (CAGR = –1.4%; R 2 = 0.77), for knee-related procedures by 31% (CAGR = –2.0%; R 2 = 0.81), and for procedures relating to the foot and ankle by 38% (CAGR = –2.5%; R 2 = 0.79).
Conclusion:
Study findings indicated that inflation-adjusted Medicare reimbursement decreased substantially between 2000 and 2020 for orthopaedic sports medicine procedures, ranging from a 23% decrease for hip-related procedures to a 38% decrease for foot and ankle–related procedures. The results of this study could be used to provide further context for health care policy decisions and help ensure sustainable financial environments for orthopaedic sports medicine surgeon.
Medicare was established in the United States to provide medical coverage for those aged >65 years and others with qualifying health conditions. It is currently the largest insurer in the United States. 6,8 Since its inception, Medicare has been rapidly expanding alongside the growing elderly population. 16 When Medicare was established in 1965, the median life expectancy in the United States was 70.11 years, whereas it is currently estimated to be 78.81 years. 38 The increasing proportion of patients covered by Medicare provides an impetus for economic study.
Within Medicare, orthopaedic surgeons are reimbursed a professional procedural fee based on the specific service performed. Each procedure carries a corresponding Current Procedural Terminology (CPT) code that is specific to each medical procedure and service. Each CPT code has an assigned physician reimbursement according to the valuation of the relative value units (RVUs) determined by the relative value update committee (RUC). 15 These payments are also adjusted by geographic region.
Decreasing Medicare reimbursement has been noted among many specialties. 13,18,20,21,32,33 Furthermore, many orthopaedic surgery subspecialties including total joint replacement, trauma, hand and wrist, and shoulder have reported decreases. 17,19,28,36,40 While these subspecialties have been well defined, there is a paucity of literature regarding Medicare reimbursement in orthopaedic sports medicine. One such applicable study by Moore et al 29 examined arthroscopic procedures and reported a 30% decrease in reimbursement for the included 20 procedures. Notwithstanding, Moore et al 29 examined a limited number of specific arthroscopic procedures.
The purpose of this study was to further elucidate the trends in inflation-adjusted Medicare reimbursement in the field of orthopaedic sports medicine between 2000 and 2020 and to provide subanalysis by anatomic location. The authors hypothesized that Medicare reimbursement for orthopaedic sports medicine procedures decreased by at least 20% across all anatomic locations during the study period.
Methods
Institutional review board approval was not required for this study, as only publicly available data were used in this analysis. The methods of this study were adapted from similar studies examining Medicare reimbursement trends. 13,18,29 Orthopaedic sports medicine–specific procedures were obtained from the orthopaedic sports medicine Accreditation Council for Graduate Medical Education (ACGME) case log guidelines, which contain a comprehensive and categorized list of orthopaedic procedures and CPT codes related to orthopaedic sports medicine. 1 Services not existing in 2000 or 2020 were excluded from this analysis (n = 13) (Table 1).
Reasons for Exclusion of 13 Procedures From This Study a

a CPT, Current Procedural Terminology; SLAP, superior labrum anterior and posterior.
Reimbursement data for each of the included CPT codes from the Centers for Medicare and Medicaid Services (CMS) website were obtained by 3 authors (J.R.P., E.H.R., B.I.E.) using the Physician Fee Schedule Look-Up Tool. 9 The pricing information for each geographic Medicare Administrative Contractor locality across the country between 2000 and 2020 was averaged to obtain a national average reimbursement for each code for each year. To adjust for substantial inflation between 2000 and 2020, the reimbursement averages for each CPT code were adjusted according to the change in Consumer Price Index from the US Department of Labor, Bureau of Labor Statistics website. 41 We adjusted for inflation by multiplying the 2000 reimbursement of each code by the 2000 January inflation multiplier. This process was repeated for each year and each code. The average annual change and total percentage change between 2000 and 2020 were calculated after adjusting for inflation for each procedure and on average across all procedures. These same analyses were performed for each category of sports procedures according to their designation in the ACGME case log. These categories were shoulder and elbow, hip, knee, and foot and ankle.
The compound annual growth rate (CAGR) was calculated using the inflation-adjusted monetary data from 2020 and 2000. The CAGR is a common economic measure that is utilized to control for variability over stretches of time. CAGR also provides a more realistic and precise measure of annual rate of change. 14 CAGR is calculated using the following formula:

An R 2 regression value was also calculated to estimate the goodness of fit of the changing reimbursement values to a linear model.
Additionally, a subanalysis was performed to compare the average change in reimbursement among all included procedures between 2000-2010 and 2011-2020. This subanalysis was carried out using a 2-tailed t test comparison of means. All statistics and calculations were performed using Microsoft Excel for Office 365 (Microsoft Corp). Alpha level was set at < 0.05.
Results
Overall, inflation-adjusted mean Medicare reimbursement for the included 67 CPT codes decreased from $1171 on average in 2000 to $783 on average in 2020. Additionally, the median inflation-adjusted reimbursement of all codes between 2000 and 2020 decreased by 33% (range, –15% to –84%). This analysis included 67 CPT codes after excluding 13 codes that did not exist in either 2000 or 2020 (Table 2).
Differences in Inflation-Adjusted Medicare Reimbursement Between Sports Medicine Procedures a

a CPT, Current Procedural Terminology; USD, US dollars.
Foot and ankle sports medicine procedures had the lowest average reimbursement for all 20 years between 2000 and 2020, while knee procedures had the highest average Medicare reimbursement for all years. All categories experienced a similar downward trend in reimbursement from year to year, ranging from a mean decrease of 23% for hip to 38% for foot and ankle (Figure 1).

Summary of differences among orthopaedic sports medicine procedures between 2000 and 2020. USD, US dollars.
The reimbursement for each individual code is shown in Appendix Table A1. Overall, the mean R 2 regression value for the 67 included orthopaedic sports medicine procedures was 0.78, which was reflective of a moderately strong constant linear decline in reimbursement between 2000 and 2020. The mean CAGR for all included procedures was –2.2%, which was also indicative of a consistent yearly decline in reimbursement between 2000 and 2020 (Appendix Table A1).
Inflation-adjusted Medicare reimbursement for the 21 shoulder and elbow procedures decreased from $1190 in 2000 to $777 in 2020 (34% decrease). The largest decrease (84% decrease) was seen for CPT code 29826, which represents subacromial space decompression with partial acromioplasty and coracoacromial release. The smallest decrease (25% decrease) was seen for CPT code 23120, which represents partial claviculectomy (Table 3).
Inflation-Adjusted Medicare Reimbursement Between 2000 and 2020 by Orthopaedic Sports Medicine–Related Shoulder and Elbow CPT Code a

a CAGR, compound annual growth rate; CPT, Current Procedural Terminology; USD, US dollars.
Inflation-adjusted Medicare reimbursement for the 4 hip procedures decreased from $1043 in 2000 to $793 in 2020 (23% decrease). The largest decrease (29% decrease) was seen for CPT code 29861, which is hip arthroscopy with removal of loose body or foreign body. The smallest decrease (15% decrease) was seen for CPT code 29860, which is diagnostic hip arthroscopy with or without synovial biopsy (Table 4).
Orthopaedic Sports Medicine–Related Inflation-Adjusted Medicare Reimbursement, 2000-2020: Hip Codes a
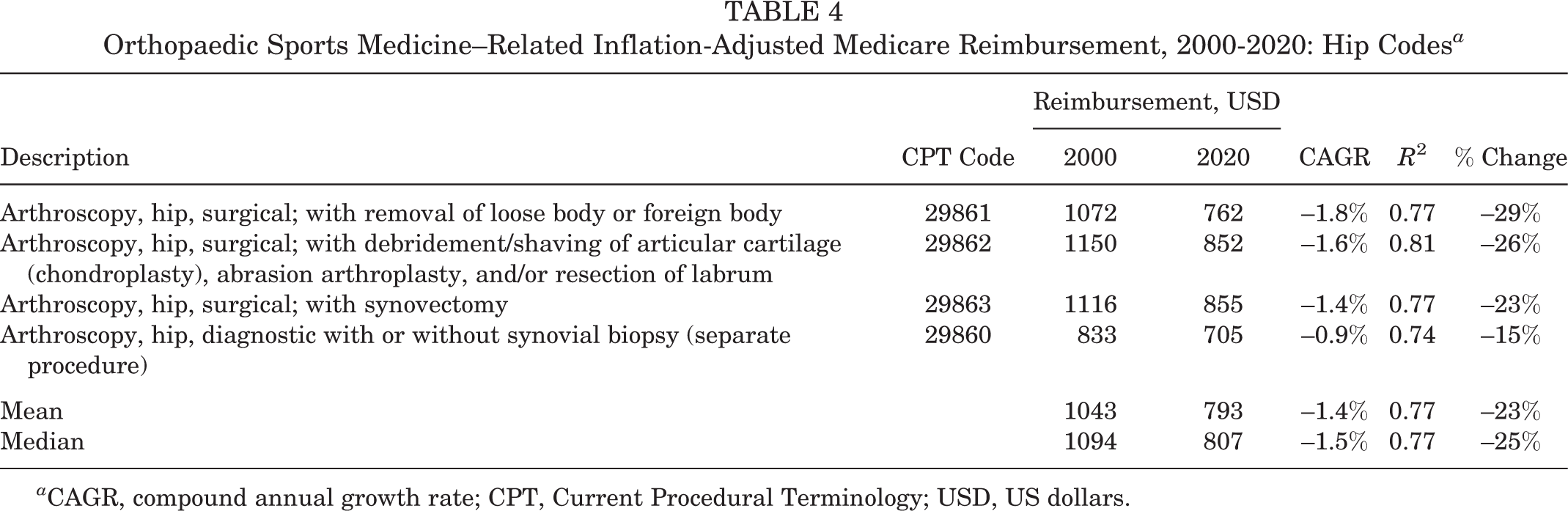
a CAGR, compound annual growth rate; CPT, Current Procedural Terminology; USD, US dollars.
Inflation-adjusted Medicare reimbursement for knee procedures decreased from $1259 in 2000 to $862 in 2020 (31% decrease). The largest decrease (43% decrease) was seen for CPT code 27556, which is open treatment of knee dislocation without primary ligamentous repair or augmentation/reconstruction. The smallest decrease (18% decrease) was seen for CPT code 27429, which is intra-articular and extra-articular ligamentous reconstruction (augmentation) of the knee (Table 5).
Orthopaedic Sports Medicine–Related Inflation-Adjusted Medicare Reimbursement, 2000-2020: Knee Codes a

a CAGR, compound annual growth rate; CPT, Current Procedural Terminology; USD, US dollars.
Inflation-adjusted Medicare reimbursement for foot and ankle procedures decreased from $984 in 2000 to $613 in 2020 (38% decrease). The largest decrease (45% decrease) was seen for CPT code 28485, which is open treatment of a metatarsal fracture. The smallest decrease (30% decrease) was seen for CPT code 29891, which is ankle arthroscopy with excision of osteochondral defect of talus and/or tibia, including drilling (Table 6).
Orthopaedic Sports Medicine–Related Inflation-Adjusted Medicare Reimbursement, 2000-2020: Foot and Ankle Codes a

a CAGR, compound annual growth rate; CPT, Current Procedural Terminology; USD, US dollars.
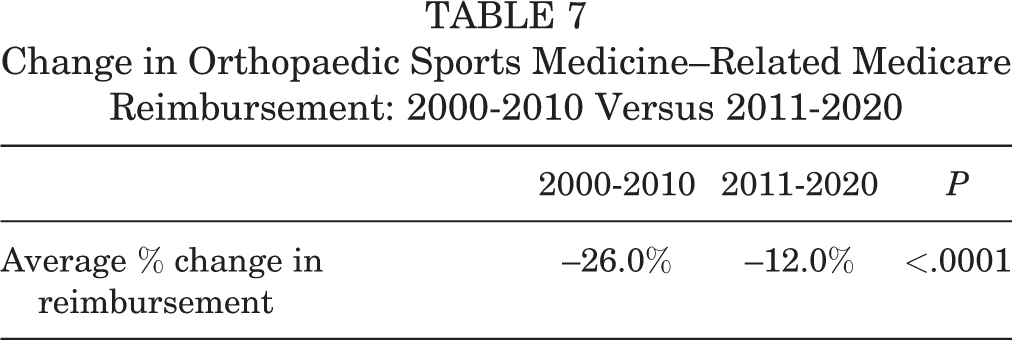
The subanalysis regarding the mean adjusted reimbursement values for all procedures between 2000-2010 and 2011-2020 revealed a statistically significant difference between the 2 time periods (P < .0001) (Table 7).
Change in Orthopaedic Sports Medicine–Related Medicare Reimbursement: 2000-2010 Versus 2011-2020
Discussion
We found that Medicare inflation-adjusted reimbursement decreased substantially between 2000 and 2020 for orthopaedic sports medicine procedures. There was a 33% mean decrease overall, ranging from a 23% decrease in reimbursement for orthopaedic sports medicine hip-related codes to 38% for orthopaedic sports medicine foot and ankle–related codes. Throughout this time period, the sports medicine codes with the highest reimbursement each year were related to knee procedures, while the codes associated with the lowest reimbursement each year were related to foot and ankle procedures. There was also evidence of a consistent yearly decline in reimbursement, which is reflected by an R 2 value of 0.78 and a CAGR of –2.2%. These decreases in reimbursement are compounded by a large increase of Medicare patients, with Medicare beneficiaries increasing from 13.5% of the US population in 2000 to nearly 18.1% in 2019. 39 While the proportion of patients covered by Medicare in sports medicine orthopaedic practices remains unclear, changes in Medicare reimbursement have been shown to substantially affect private payors, and as such, changes to Medicare reimbursement have a far-reaching effect. 10 The results of this study could be used to provide further context for health care policy decisions and help ensure sustainable financial environments for orthopaedic sports medicine surgeons.
Orthopaedic sports medicine has experienced a similar decrease in reimbursement to other fields of orthopaedic surgery, with the mean inflation-adjusted Medicare reimbursement decreasing 39% for hip and knee arthroplasty, 17 27% for shoulder and elbow surgeries, 28 22.6% for hand surgeries, 40 30% for commonly performed arthroscopy procedures, 29 and 30% for orthopaedic trauma. 19 Accordingly, this study corroborates the findings of decreasing reimbursement found in other subspecialties of orthopaedic surgery and further defines the reimbursement decrease in orthopaedic sports medicine (Appendix Table A2).
It is traditionally thought that Medicare reimbursement is significantly less than that of commercial payors. However, this difference varies by procedure. For example, the commercial payor average for “shoulder arthroscopy” in 2011 was more than double that of Medicare reimbursement, while commercial payment for “shoulder arthroscopy: capsulorrhaphy” was only 16% more than Medicare reimbursement. 12 While both commercial and Medicare payments for orthopaedic surgeries were noted to decrease markedly between 2010 and 2018, Medicare payments decreased by an average of 1.5 times faster than commercial payments. 43 This study also found that, on average, payments from Medicare for orthopaedic surgeries were 57% less than payments from commercial payors. 43 The decreasing reimbursement trends seen in this study for orthopaedic sports medicine are likely similar to decreasing reimbursement trends by commercial payors, albeit to a lesser degree. Reimbursement trends of large, commercial payors warrant future analysis to further define these trends.
Health care policy changes over the last 2 decades further contextualize the findings of decreasing Medicare reimbursement, such as the Balanced Budget Act of 1997 (BBA), Medicare Access and Children’s Health Insurance Program Reauthorization Act of 2015 (MACRA), Merit-based Incentive Payment System (MIPS), and bundled payment programs. 7,30,31,37 The BBA was enacted in 1997 and created the sustainable growth rate (SGR), which cut payment for physicians, and by 2002, the SGR reduced overall payment rates by 4.8%. 5 After years of physician payment cuts from the SGR, the BBA was subsequently replaced by MACRA in 2015 in an attempt to focus on quality of services rather than quantity of services. 7 Under MACRA, 2 payment options were created in 2017 named Alternative Payment Models and Merit-based Incentive Payment System (MIPS). 7 These models were designed to give positive or negative payment adjustments based on certain parameters of care. 37 As a result of the changes brought about from these health care policy changes, investigations have aimed to help orthopaedic surgeons understand how to navigate these changes. 4,34 In the context of these policies, this study found a statistically significant difference between 2000-2010 and 2011-2020 reimbursement differences. The average decrease in reimbursement for orthopaedic sports procedures was 26% between 2000 and 2010 and 12% between 2011 and 2020.
Annual adjustments to CPT code pricing are made on an annual basis by the RUC, based on many factors, including physician work and time required to perform a service, practice expense, and malpractice costs. 3 This committee consists of 32 volunteer physicians from various specialties, including 1 representative orthopaedic surgeon. 3 These physicians alter the valuation of CPT codes by adjusting the associated RVUs. The 3 RVU components, which hold different weights, are work RVU, practice expense RVU, and malpractice RVU. These RVUs also have a geographic adjustment named the work geographic pricing cost index (GPCI), practice expense GPCI, and malpractice GPCI. These factors are multiplied together with the yearly conversion factor to determine physician payment.
It has been reported that the RVUs and payment determined by the RUC may not accurately reflect work effort for certain procedures. 11 A prominent example of this is septic revision total hip arthroplasty, in which the complexity and difficulty of the case are not reflected in the RVU and payments determined by the RUC. 35 As a result, surgeons may limit or avoid performing certain procedures and ultimately limit access for patients to needed procedures. 22 Additionally, it has been demonstrated that arthroscopic procedures generate more RVUs per hour than the same procedures performed using an open approach. 24 These changes could influence surgical treatment decisions unnecessarily. Our study found heterogeneity between the rate of decreasing reimbursement between different procedure categories, with foot and ankle codes exhibiting the largest decrease. Awareness of these trends is necessary to ensure equitable reimbursement between subspecialties and procedures, all of which play a critical role in providing quality orthopaedic care in the United States. Future study is needed to explore possible solutions to decreasing Medicare reimbursement in orthopaedic sports medicine surgery.
This study is not without limitations. This study only used the data from a single payor. Therefore, the trends observed in this study may not represent reimbursement by third-party payors. Further study is needed to elucidate trends in reimbursement amount from third-party payors between 2000 and 2020. The authors of this study understand that the limited number of codes included do not represent all the possible procedures and services performed by orthopaedic sports medicine surgeons. However, the authors believe that the CPT codes included in this analysis likely represent a balanced picture of a typical orthopaedic sports medicine surgical practice. Further study is needed to fully analyze the effects of decreased Medicare reimbursement in orthopaedic sports medicine on surgeons, patients, and hospitals.
Conclusion
Medicare reimbursement decreased substantially between 2000 and 2020 for orthopaedic sports medicine procedures, ranging from a 23% decrease in inflation-adjusted Medicare reimbursement for hip-related procedures to a 38% decrease for foot and ankle–related procedures. The results of this study could be used to provide further context for health care policy decisions and help ensure sustainable financial environments for orthopaedic sports medicine surgeons.
Footnotes
Final revision submitted September 12, 2021; accepted November 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.C. has received education payments from Arthrex and consulting fees from Arthrex and Zimmer Biomet. N.B.H. has received an education grant from Goode Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.