
Abstract
Background:
The incidence and etiology of prosthetic services utilization is poorly understood during the first 90 days post-delivery of the initial lower limb prosthesis. This period is of critical importance, as prevailing policy dictates limits on the reimbursement for certain services provided during this time period. The first step in understanding the financial ramifications of such policy is to examine the taxonomy behind clinical encounters during this tenuous time period.
Objectives:
Quantify and categorize clinical encounters by incidence and etiology.
Study design:
Retrospective chart review.
Methods:
A central database containing data on prosthetic services was examined. Incidence and etiology were extracted through independent review of each patient chart.
Results:
A total of 537 unique patients were identified, with 109 meeting the inclusion criteria. Chi-square testing showed that comfort (p < 0.05), cosmesis (p < 0.01), and mechanical failure (p < 0.001) yielded statistical significance in scheduled versus unscheduled visits. Stepwise regression analysis demonstrated that both sex and K-level were important predictors of unscheduled visits.
Conclusion:
Taxonomization of clinical encounters experienced during the first 90 days provides a framework for future studies to be conducted. The data provided can serve as a basis for informing reimbursement policy, workforce planning, and advocacy.
Clinical relevance
Comfort is the most frequent reason for a clinical encounter during the first 90 days after delivering a lower limb prosthesis. The data on the taxonomy behind the clinical encounters can be used to guide workforce planning and advocate for just reimbursement policy that better reflect patient’s needs.
Background
Prosthetics services performed annually number in the millions, a volume that is only expected to grow in the future.1–6 While Medicare does not report separately on the proportion of services categorized as post-delivery, nor their cost, estimates may be conjured from the literature: lifetime costs of clinical services for lower limb amputees is projected between US$300K and US$1.5M; adjusted for inflation, these costs are substantially front-loaded. 7 Given the sheer cost and the ever-increasing interest in better understanding the machinations of clinical encounters—most especially their relationship with reimbursement—there is urgency in refining scientific inquiry into clinical services.7–11
Of critical relevance here is the prevailing policy that during the first few months following initial prosthesis delivery, many services related to adjusting or repairing the prosthesis are not billable by Medicare. The current Center for Medical Services (CMS) 12 Local Coverage Determination (LCD) for lower limb prostheses (L33787) stipulates that repairs due to normal wear and tear or adjustments of the prosthesis not necessitated by changes in the residual limb, medical status, or functional status will be denied as separate claims if billed within 90 days of delivery. Nevertheless, patient needs in this 90-day window can be intensive and highly variable. This places the prosthetist in the unfortunate position of balancing the inherent volatility of service demands versus the rigid single-bolus reimbursement structure for a period of 3 months.
Standard of care in follow-up of patients receiving a prosthesis will typically include visits related to patient comfort, assessing compliance with the wearing protocol, and to allow the prosthetist an opportunity to assess the efficacy of their treatment plan. By contrast, unscheduled visits are precipitated by an emergent and unforeseen issue. 13 However, the incidence and etiology of clinical encounters related to prosthetic services has never been studied, and thus it remains unknown the frequency and nature of visits comprising the post-delivery caseload.
Being able to describe the number of visits experienced in the first 90 days following the first lower limb prosthesis delivery, provides a first and highly needed glimpse into the potential financial ramifications of policy decisions. Therefore, the purpose of this study was to examine the incidence and etiology of clinical visits during the first 90 days post initial prosthesis delivery to new prosthesis wearers.
Methods
Chart review
After receiving ethics approval from the hosting clinics to access data, a retrospective chart review was performed between November 2016 and January 2017 within a centralized database of 16 prosthetic clinics and 28 individual prosthetists spanning five states in the Northeastern United States. Only de-identified data were extracted. Charts were reviewed using OPIE software (Gainesville, FL) and a standardized extraction template. For encounters to be included in the study they needed to meet the following criteria: (1) have received their first transtibial or trans-femoral prosthesis and (2) have at least two follow-ups within 90 days post-delivery. To be included, the documentation must show that the subject received a letter of delivery along with documentation of the prosthesis being delivered. Cases were excluded if (1) the patient had prior experience managing a prosthesis, (2) the charts were incomplete (missing multiple notes or demographic variables), (3) patient was younger than 18 years of age, or (4) a medical event interrupted normal care during the first 90 days. A report of viable candidates for inclusion was provided to the researchers prior to beginning the search by a staff member familiar with the database and who was blinded to the purpose of the study. Prior to chart review, demographic variables of interest and etiological categories for clinical encounters were drafted based on expert opinion of two prosthetists (mean experience 17 years), supported by a literature review for common reasons for visiting the prosthetist.14–17 Descriptions classifying each of the etiologies can be found in Table 1.
Clinical encounter etiology classifications.
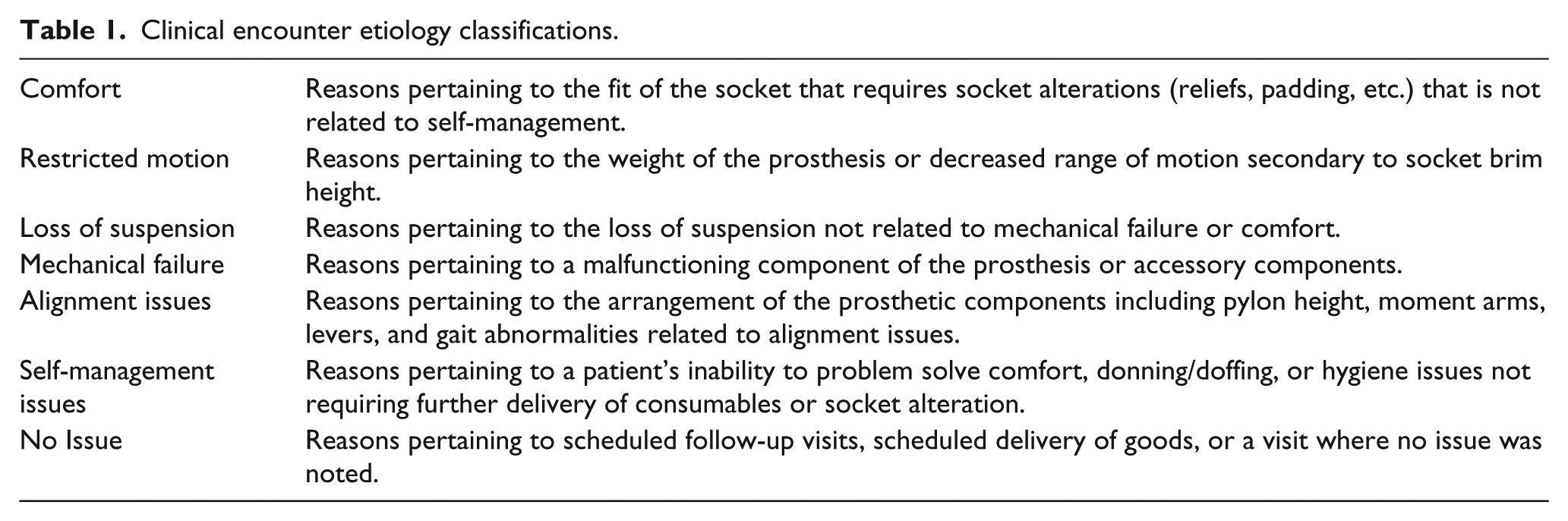
Only those encounters within 90 days following delivery of the initial prosthesis were included in the analysis. Each chart was individually reviewed for study inclusion criteria by one of the authors. The note for each individual clinical encounter was read with an interest in extracting the etiology, as well whether the encounter was scheduled or unscheduled. Encounters were considered unscheduled if the prior notes indicated no further need for scheduled visits, or the note indicated an urgent matter requiring attention. In the case of any difficulty interpreting the note, a second reviewer, a certified prosthetist with over 10 years of experience, provided consultation and a decision was reached on how to categorize the encounter. Following data collection, a random audit of 10% of the clinical encounters dataset was performed by a trained prosthetics resident unfamiliar with the objectives of the study. We set the a priori criteria that if <20% of the random sample yielded disagreement between the coder and the auditor, then the complete dataset would be considered valid for analysis.18–20
Analysis by etiology
Our primary objective was to test whether any etiology was disproportionately prevalent among unscheduled visits. For each etiology, we conducted a small-sample adaptation to the chi-square test of proportions, that is, Fisher’s exact test; the contingency table was devised to compare four quantities: the number of scheduled and unscheduled visits associated with a given etiology and the number of scheduled and unscheduled visits of all other etiologies. Fisher’s exact test was justified because some etiologies occurred only rarely (and subdividing into unscheduled vs scheduled would diminish the elements in the contingency matrix even further). Significance was assessed via unadjusted p values. 21
Analysis by demography
A secondary objective was to assess whether there were factors that associated significantly with unscheduled visits. This was conducted via an iterative backward variable selection on the following 10 variables: age, sex, insurance, marital status, mental status, prosthesis type, patient weight, IPOP, suspension type, and K-level. Regression involving categorical variables was performed in consideration of established best practices (Regression for Categorical Data by Gerhard Tutz). Two simple linear regressions were constructed with (1) the total number of unscheduled visits (τ) and (2) the proportion of unscheduled visits, relative to total number of follow-up visits (π). This analysis carries three variables treated as continuous (age, K-level, and weight), five factors as binary factors (sex, marital status, mental status, prosthesis type, and IPOP), and two multilevel categorical variables (insurance and suspension type); in total, the models have 14 degrees of freedom.
Results
Descriptive statistics
A total of 537 unique patients were identified by the facilitator, with 109 meeting the inclusion criteria. Reasoning for exclusion included: no follow-up data available (n = 110), incomplete notes (n = 65), prior prosthesis experience (n = 205), 90 days have not elapsed since delivery (n = 29), medical compromise (n = 15), and less than 18 years of age (n = 4). Demographic information is presented in Table 2.
Demographic and descriptive statistics included data. 109 unique subjects; 438 total visits.
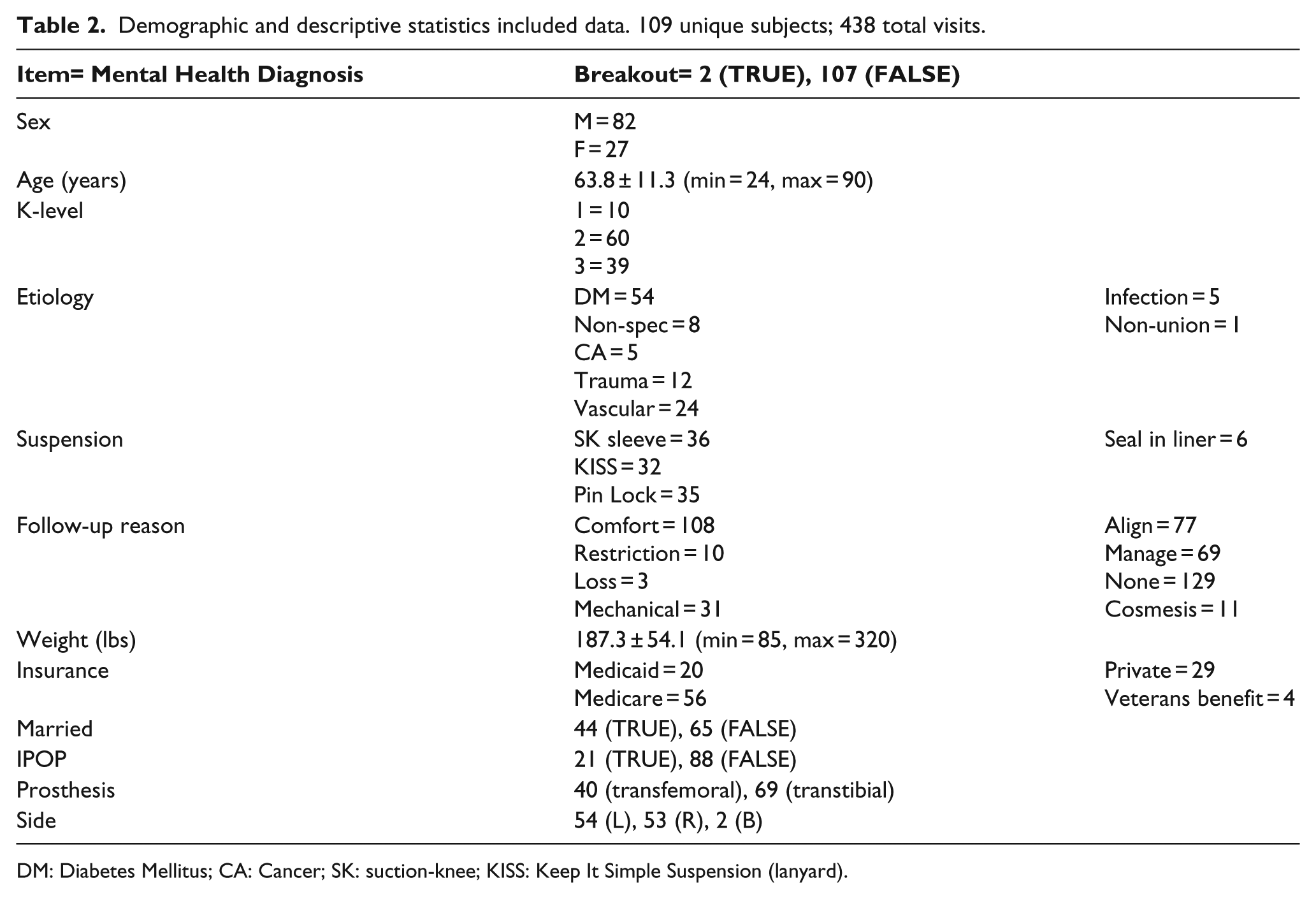
DM: Diabetes Mellitus; CA: Cancer; SK: suction-knee; KISS: Keep It Simple Suspension (lanyard).
Among these 109 patients, a total of 438 follow-up visits were documented (median: 5, range: 2–15). Per protocol, a randomly selected 10% data subset was independently reviewed for agreement by a trained specialist naïve to the study objectives, whereupon concordance with the primary adjudicator was measured within this subsample. Visit etiology was concordant in 47 of the 58 encounters (81%), thus the dataset was considered valid and viable as a substrate for analysis. All analyses reported here were performed using the R numerical computing environment, v3.1.0.
Analysis by etiology
In the serial chi-square test, comfort (p < 0.05), cosmesis (p < 0.01), and mechanical failure (p < 0.001) all yielded statistical significance, meaning that the proportion of unscheduled visits associated with these etiologies was significantly different than the proportion of scheduled visits, relative to the ratio of unscheduled-to-scheduled for all other etiologies combined in a 7-versus-1 analysis. Visits with no attributed reason (“None”) were also significantly over-represented in unscheduled visits (p < 0.001). All other etiologies (restriction, loss, alignment, and management) failed to reach significance at the p < 0.05 level.
Analysis by demography
Two different analyses tested the impact of various patient-specific factors on the total (τ) and proportion (π) of unscheduled visits in a backward feature selection. The results are shown in Table 3.
Regression designs indexed by number of terms.
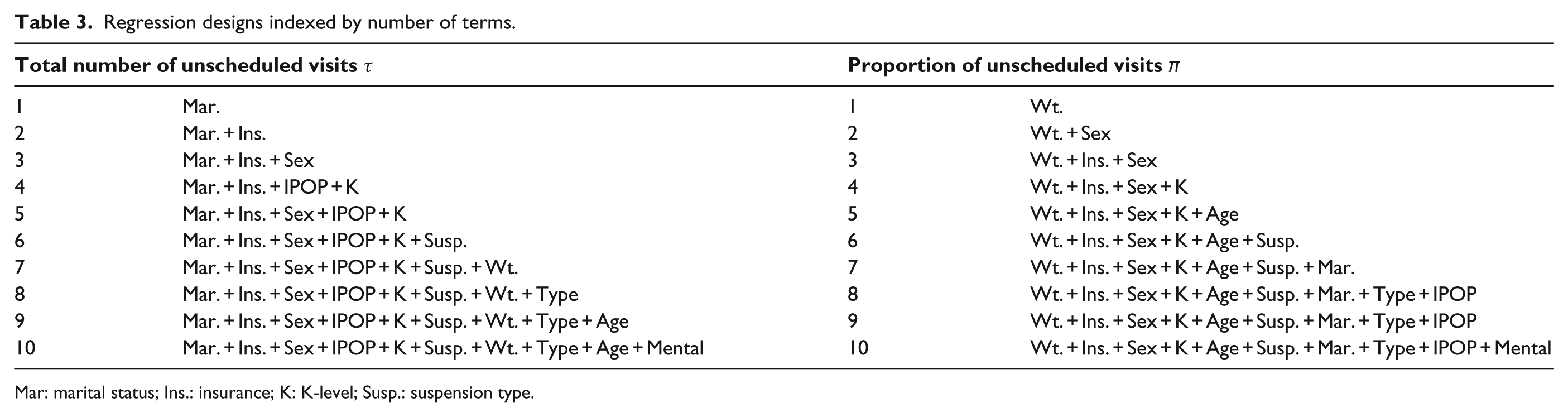
Mar: marital status; Ins.: insurance; K: K-level; Susp.: suspension type.
Given that there were 10 patient variables, a linear regression equation with no high-order terms or specified interactions can have up to 10 predictor slope coefficients. Depending on the number of terms, some variables may be more or less explanatory. For example, sex is found in the three-term regression for the total number of unscheduled visits τ (Table 3), but not the four-term regression. While this intermittency is not unexpected, it is pleasing that the results follow an otherwise very hierarchical ordering, with fairly consistent and clear utility in modeling scheduled versus unscheduled visits.
In both comparisons, insurance type, sex, and K-level were important predictors of unscheduled visits, as seen by their inclusion in the first few regression models; mental status was a weak predictor in both the analyses. Patient weight was the best predictor of total proportion of unscheduled visits, it was only a moderately useful predictor of the total number of unscheduled visits. While the scope of this article does not permit a more comprehensive analysis, we performed a preliminary inquiry into the true potency of these factors by selecting the most impactful variables for each response variable, and performed a standard linear regression with no interactions.
We tested both response variables (τ and π) in five-term regressions. For the model on total counts, no terms showed significance in the linear model at p < 0.05; in the model on proportions, weight showed significance at p < 0.05. The model fit on total unscheduled visits was multiple R2 = 0.05 (p > 0.05); the model fit on proportion of unscheduled visits was multiple R2 = 0.15 (p < 0.05). Thus, even a reduced-scope model limited to the best features yielded poor goodness of fit. We note that models of such poor fit are not uncommon; studies attempting to associate clinical or demographic variables to outcomes often show R2 < 0.2.22–27 In contextualizing this result, it is important to consider two things: (1) a model with small R2 but significant p value (as observed with π) indicates a small but reliable relationship between predictors and outcome and (2) a model with small R2 and no significant p value (as observed with τ) suggests no substantial predictive power between predictors and outcome. Whereas this study is the first of its kind, we remark that these results are preliminary and meant to provide impetus for further exploration; model goodness in this setting is best interpreted as a first data point to describe the landscape, and not per se a definitive or conclusive outcome.
Discussion
Clinical relevance
Of the 438 clinical encounters, 282 were scheduled and 156 were unscheduled. The most common etiology for an encounter was “no reason” (29.4%), followed by comfort (24.5%), alignment issues (17.5%), self-management (15.7%), mechanical failure (7%), cosmesis (2%), restriction (2%), and loss of suspension (<1%).
Scheduled encounters comprised 64.4% of all encounters. The most common etiology for a scheduled encounter was “no reason” (44.6% of scheduled encounters), which is consistent with a follow-up visit for a client who stated an absence of issues during the appointment. These encounters may have also occurred for the purposes of mere transaction, rather than provision of clinical expertise, that is, dropping off socks, liners, or a replacement shrinker. The number of follow-up visits varied between clients, with some requiring only two scheduled follow-ups, or some as many as 15. Scheduled encounters are performed at the discretion of the individual prosthetists based on the patient’s objective and subjective findings, their medical profile, and clinical expertise. Scheduled encounters for comfort (22.6%) involved the prosthetist modifying the socket either through reliefs, additions, or any other modification requiring skilled application. Considering the dynamic nature of the residual limb during the first 90 days, 28 a certain number of encounters for comfort-related adjustments and modifications is not unreasonable and are considered in the cost of the initial prosthesis.
Alignment issues accounted for 15.2% of the etiologies for scheduled clinical encounters, and this categorizes adjustments made to prosthesis to improve stability, gait, and function. Decreasing or increasing pylon height, adjusting the friction mechanism of the componentry, or modifying the socket angle were performed during the encounter, with confirmatory gait analysis in many of the cases. Self-management issues made up a total of 10.2% of the scheduled encounters, and this included reasons like modifying the number of sock ply being worn, aligning the prosthesis properly, wearing all the necessary adjunct components, or following the prescribed hygiene protocol. Finally, all of the visits related to cosmesis were scheduled, an expected result, given the nature of the etiology being non-urgent and requiring a dedicated encounter to address the request.
When only looking at the incidence and etiology of unscheduled clinical encounters (156/438 total visits; 35.6%), we see that comfort (28.2%), mechanical failure (16.6%), alignment problems (21.7%), and self-management (25.6%) issues make up 92.3% of the reasons a prosthetist was sought out. It is believed that comfort is the most common reason for requiring a prosthetist once the patient is wearing a prosthesis, 13 and this study supports that finding. Considering that fit is a key indicator of successful gait, as well as the ability to engage in vocational and recreational activities, comfort remains one of the top priorities for the client. 29 Unscheduled encounters related to comfort are potentially unavoidable, and also potentially dangerous to the client. If a patient has discomfort in their residual limb and it is a result of poorly fitting socket, they are at risk of developing preventable secondary complications such as a wound. 30 Therefore, the urgency of such request require that the client either come into the clinic immediately, cease wearing the prosthesis until they can, or have the prosthetist travel to their residence/facility.
When considering all of the variables, certain relationships emerge. First, given that sex and K-level were important predictors of unscheduled visits, it is suspected that an underlying interaction exists. We found the distribution of K-levels (K1, K2, and K3) for males was (7, 44, 31) and for females (4, 16, 7). While the ratios vary from 4.4:1 to 1.8:1, a chi-square analysis fails to show imbalance between the distribution of K-level between sexes; clearly, the dataset is highly enriched in males. Males and females had approximately the same proportion of unscheduled visits (53 ± 26% vs 55 ± 24%, p not less than 0.05 in a one-way analysis of variance (ANOVA). When adding K-level as a factor, there was also no significance, either as a direct effect, or as an interaction with sex, although the interaction term was weakly insignificant (p < 0.10); perhaps in a larger dataset, an interaction term would yield significance.
Self-management made up the second most common reason for an unscheduled visit. This category was defined by interventions the client is capable of performing at home (e.g. problem-solving the fit of their prosthesis through manipulating sock plys), efforts to reduce these issues would be beneficial to both the client and the profession. These visits additionally represent requests from other clinicians, such as physical therapists or a nurse who are either unfamiliar or untrained in managing the residual limb–prosthesis interface. This etiology in particular has the potential to be eradicated as a reason for an unscheduled visit through targeted educational interventions geared at empowering the prosthesis user (or their caretakers) in the self-management process. 31 Alignment issues were the reason for approximately one out of every five unscheduled encounters, and were generally precipitated by the clients’ complaint of feeling unbalanced during standing, seated, or when performing functional mobility. It was sometimes noted that following an initial scheduled alignment modification, several unscheduled encounters were precipitated for further adjustments. Mechanical failure was the final predominant etiology represented in this model that required a significant number of unscheduled encounters. Unscheduled encounters made up 83.9% of the total visits due to mechanical failure (n = 31 visits). In fact, when chi-square analysis was performed, only unscheduled encounters for mechanical failure were statistically significant in the analysis. This finding seems reasonable given the unpredictable nature of mechanical failure.35,36
Methodological notes
In our approach of a database review, we were substantially aided by a standardized extraction form, a structured protocol for note review, and pre-established adjudication procedure. By agreeing to an internal audit for review consistency, we added an additional measure of robustness. While not explicitly described in our methods, we regularly performed intermittent interim review of our results, with team debriefings to ensure completeness of data collection and methodological soundness. We urge that others replicating this work adopt a similar framework to ensure systemic integrity.
Study rationale and novelty
Given the ever-increasing patient population, and also the ever-maligned payer support of the comprehensive clinical care that new prosthesis wearers require, there is incumbent need to understand who is seeking follow-up from the prosthetist. While prior studies have examined the incidence and etiology of the delivery of prosthetic limbs, no study to date has examined the incidence and etiology of the ensuing clinical encounters. Notwithstanding the clear need for benchmark studies on clinical service provision, most especially for their relevance to policymaking and business operations planning, to our knowledge, no such work exists.
Demographics
The cases included were mostly male older adults classified as either a K2 or K3 level ambulatory. The most common reason for the amputation was due to vascular disease and the most commonly reported amputation level was transtibial. Four major suspension types were identified in the analysis. These findings are consistent with what is statistically observed among limb loss populations,32–34 making this sample valid for inferences to be drawn. However, as geographical, financial, and state practice acts can influence patient care and thus services delivered, it is important to consider the locale’s unique characteristics when attempting to generalize the results beyond the boundaries of the study.
Connection to literature
While there are few extant studies on which to draw parallels to our study, we find several reports that support our findings here. For instance, we have confirmed the conjecture that comfort is the most common reason for requiring a prosthetist once the patient is wearing a prosthesis. By contrast, we found that mechanical comprised predominantly unscheduled encounters (83.9%).
Implications
The data presented in this study can serve as basis for determining appropriate clinician caseloads, as well as supportive evidence for necessity of care when submitting to an insurance provider. Performing the same analysis as completed in this article for an individual clinic or corporation will allow for managing parties to distribute the caseload appropriately between clinicians based on predicted needs. Furthermore, when analyzing the productivity of a clinician, parallel comparisons with other clinicians or arbitrary benchmarks may not be the most effective option. Rather, basing the productivity standard on the clinician’s case-mix composition may be a more appropriate option.
Beyond the clinical implications, we believe that a study like this has important implications for policy. Through this study, we anticipate that future studies will be able to answer the “one size fits all” question inherent in bundled payments. We note a bundled payment system is not unique to Prosthetics, but is common (and controversial) in many corners of medicine; we believe this article will have broader impacts beyond clinical prosthetics. Moreover, through our approach, we hope to not only legitimize coarse assessment (univariate assessment, e.g. scheduled vs unscheduled), but inspire more nuanced views, for example, stratification by K-level, sex, or insurance type. At the same time, we caution that clinical practice simply does not bear discrimination. Within the United States, Title VI of the Civil Rights Act of 1964 strictly prohibits denial of services on the basis of race, color, or national origin; this foundation has been subsequently extended by the provisions of the Americans with Disabilities Act (ADA), the Hill–Burton Act, and the Health Insurance Portability and Accountability Act (HIPAA). The American Board for Certification in Orthotics, Prosthetics & Pedorthics (ABC) in its Code of Professional Responsibility), article C3.12 states “The ABC Credential Holder shall not decline to accept a patient on any basis that would constitute illegal discrimination under federal law.” This would be considered similar to the perhaps more well-known article of the American Medical Association, Ethical Rule 10.05, which prohibits refusal of care of patients “based on … any criteria that would constitute individuous discrimination.” We understand that many similar national and international agencies governing provision of care in medical and allied health settings (to include P&O) have similar ethical principles at play.
Limitations
There were several limitations to the study. While the dataset that was analyzed was a random selection of encounters from 16 clinics and 28 clinicians across 5 states, most were all located within 300 miles of each other; all clinics franchised under the aegis of a single corporation. The diversity that may be obtained by expanding the pool to include other care provider networks, in other states, and other clinics, extending beyond the studied dataset could offer a different perspective and might improve study generalizability. The study was also limited by the vagaries of medical recordkeeping: where this was a historical look-back of existing clinic notes, it was not always clearly specified whether the visit was scheduled or unscheduled; classification therefore was empiric. Missing data and data censored due to incomplete recordkeeping creates a potential for bias, although it is not immediately clear whether the consequence would be an over- or under-estimation of the proportion of unscheduled visits.
Furthermore, we acknowledge the limitations inherent in not assessing certain demographic variables (change in weight, education level, race, and ethnicity) and clinical variables (time since amputation, change of weight since last visit). But the data collected were intentionally limited for the sake of clarity and ease of interpretation in this first study. We believe that while these additional data points would add explanatory value, the main message of the manuscript remains without their inclusion, particularly with the rich covariates included here, that is, cause of amputation, age, mental status, and so on. Summarily, we believe that our findings provide insight into ramifications beyond the clinical realm and that further studies can expand off the framework established in this study.
Future work
We emphasize that this study be considered exploratory and not definitive; we urge others to replicate this work. Where our models showed significance, we encourage others to test using their own data; where our models failed to show significance, we ask that others to consider adding additional explanatory covariates, which may include merging etiologies where we were too granular (e.g. loss of suction and mechanical failure could be consolidated into a single etiology). For those intending to implement a large-scale review, our study may provide useful guideposts for estimating sample size for prospective power analyses. A future study looking at the financial ramification of clinical encounters is in preparation based on the pilot data.
Conclusion
This is the first study to date evaluating the incidence and etiology of clinical encounters following the first 90 days post lower limb prosthesis delivery. The most common reasons for a scheduled visit besides a normal follow-up was for reasons related to comfort and alignment adjustments. Comfort, alignment, self-management, and mechanical failure were the most common reasons for unscheduled clinical encounters. Geographical encounter patterns limit the generalizability to populations outside of the Northeastern United States; however, the study lays the framework for future studies.
Footnotes
Acknowledgements
The authors would like to acknowledge NEOPS for their support in this research project.
Author contribution
All the authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two of the authors were affiliated with New England Orthotics & Prosthetics Systems (NEOPS) at the time of submitting this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.