
Abstract
Background:
Limited knowledge exists on the role of advanced academic degrees within faculty positions in orthopaedic sports medicine.
Purpose:
To 1) provide an assessment of the baseline demographics of advanced degrees among orthopaedic sports medicine faculty and 2) examine the impact of advanced degrees on research productivity and career attainment of orthopaedic sports medicine faculty.
Study Design:
Cross-sectional study; Level of evidence, 4.
Methods:
Orthopaedic sports medicine academics were identified using faculty listings on websites of the 200 orthopaedic surgery residency programs during the 2020-2021 academic year. Advanced degrees were defined as those additional to the primary medical degree (Doctor of Medicine [MD] or Doctor of Osteopathic Medicine [DO]). Outcome measures included timing of advanced degree obtainment, residency program rankings, research productivity, and current academic rank and leadership roles. Statistical analysis was performed using chi-square and Mann-Whitney U tests to determine the association of advanced degrees on outcome measures.
Results:
In total, 911 orthopaedic sports medicine faculty members were identified, of whom 100 had an advanced degree. The most common advanced degrees were Master of Science (MS/MSc; 38%), Doctor of Philosophy (PhD; 23%), and Master of Business Administration (MBA; 13%). The presence of an advanced degree was associated with greater research productivity, including higher h-index and number of publications, as well as more editorial board positions on orthopaedics journals (P < .001). Advanced degrees were not significantly associated with attending a higher ranked orthopaedic surgery residency program, current academic rank, or leadership roles. At the institutional level, orthopaedic sports medicine programs that employed faculty with an advanced degree had a higher residency program ranking and the presence of a sports medicine fellowship was more likely (P < .05).
Conclusion:
Advanced degrees in orthopaedic sports medicine were associated with greater faculty research engagement and employment at a higher ranked institution; they were not associated with matching to a highly ranked orthopaedic surgery residency program, higher faculty rank, or academic leadership roles.
Advanced medical degrees (ie, academic qualifications additional to the primary medical degree) have become increasingly common, with many physicians seeking additional education to enhance clinical expertise and broaden knowledge of health care administration and policy. 1,36 Although formal medical education often incorporates basic coursework in research design, public health, and epidemiology, coverage of these topics is often superficial and inadequate. 28 Furthermore, as modern health care is becoming increasingly multidisciplinary, with opportunities in translational research, hospital administration, and industry innovation, additional education has become an attractive option for the modern physician in order to meet these changing demands. 26
Studies 32,40 have shown that career advancement may be the motivation for obtaining advanced degrees. Surveys among physicians have determined that individual reasons for obtaining additional education include avoiding burnout, obtaining a new job, and increasing the amount of financial compensation. 32 In other medical specialties, such as plastic surgery, general surgery, and neurosurgery, the presence of an additional degree is associated with academic career advancement, including greater research productivity, access to funding from the US National Institutes of Health (NIH), higher academic ranking, and improvements in residency program placement. 5,15,22,28 In general, there may be a competitive edge over their peers conferred on physicians who pursue an advanced degree. 40
Orthopaedic sports medicine is among the most competitive and innovative fields in health care. Attaining an orthopaedic surgery residency position has become increasingly difficult over the past decade, and the match rate for orthopaedic surgery is among the lowest of all medical specialties. 9,23 Similarly, there has been an increase in the number of orthopaedic surgeons pursuing subspecialized fellowship training, and sports medicine fellowships are among the most competitive and popular. 6,17 As a specialty, orthopaedic sports medicine relies on cutting-edge translational research and industry innovation in the forms of implantable technologies, imaging devices, and biologics to appropriately advance the surgical care of its patients. 33 Orthopaedic sports medicine surgeons serve as leaders and interface with not just patients but also hospital administration, financial executives, and the general public. 41 Owing to the competitiveness and innovation of the field, advanced degrees may play a unique role in the skillset and career enhancement of modern orthopaedic sports medicine faculty.
Although studies in other surgical subspecialties have examined the role of advanced degrees among their faculty, there have been no studies examining the demographics and role of these advanced degrees in orthopaedic surgery. Therefore, the aims of the present study were to (1) provide an assessment of the baseline demographics of advanced degrees among orthopaedic sports medicine faculty and (2) examine the impact of advanced degrees on research productivity and career attainment of orthopaedic sports medicine faculty.
Methods
In March 2021, the American Medical Association’s FREIDA residency database was queried to identify orthopaedic surgery residency programs. 14 Publicly available websites for orthopaedic surgery residency programs were used to identify academic orthopaedic sports medicine faculty. Faculty with a primary departmental listing of sports medicine or with fellowship training in sports medicine were included for analysis. Faculty with nonphysician degrees (eg, Doctor of Philosophy [PhD], Doctor of Physical Therapy [DPT], etc), a nonoperative sports medicine practice (eg, primary care sports medicine, physiatry, etc), and affiliated faculty were excluded from analysis. In total, 911 academic orthopaedic sports medicine faculty were identified across 175 of 200 (87.5%) orthopaedic surgery residency programs.
We defined the primary medical degree as the Doctor of Medicine (MD) or Doctor of Osteopathic Medicine (DO). Advanced degrees included additional training in the arts, business, public health, and sciences, such as PhD, Master of Business Administration (MBA), Master of Science (MS/MSc), Master of Public Health (MPH), and Master of Arts (MA). In all, information collected on advanced degrees included type of degree, year of degree obtainment, and timing of advanced degree relative to medical school and residency.
Background and demographic information were recorded for each surgeon, including sex, race, medical school attended, and residency program attended. In accordance with previous studies, race was defined as White and non-White. Faculty members were classified as an international medical graduate (IMG) if they attended a medical school not accredited in the United States. Further academic information collected included faculty rank (instructor, assistant professor, associate professor, and full professor) and departmental leadership roles (residency program director, fellowship program director, and chair).
Research productivity was determined through a faculty member’s h-index and number of publications, number of editorial board positions, and the presence of NIH research funding. The h-index, 16 which is a number that approximates an author’s research productivity and citation impact, as well as number of publications were obtained through the online Scopus Database. 37 We obtained the editorial board positions for 8 major general orthopaedic and sports medicine journals (Journal of Bone and Joint Surgery; American Journal of Sports Medicine; Arthroscopy; Journal of Shoulder and Elbow Surgery; Knee Surgery, Sports Traumatology, and Arthroscopy; Clinical Orthopaedics and Related Research; Journal of American Academy of Orthopaedic Surgeons; and the Orthopaedic Journal of Sports Medicine) through the journals' websites. 2,4,11,18,19,21,25,31 NIH research funding in the fiscal year 2020 was determined using the NIH website. 29
Residency program rankings were determined through both the Doximity orthopaedic surgery reputation rank and the Jones et al 20 orthopaedic surgery residency research rank. For each ranking system, orthopaedic surgery residency programs were divided from highest to lowest into 5 tiers (1-25, 26-50, 51-75, 76-100, and ≥101), similar to previous studies. 35,39 Tier 1 is the highest tier and Tier 5 is the lowest tier. Only orthopaedic surgery residency programs within the United States were included in the rankings. Accredited operative sports medicine fellowship programs were determined through the American Orthopaedic Society for Sports Medicine's website. 3
The following variables were compared statistically between faculty members with advanced degrees and those without: demographic characteristics, academic rank, academic leadership, ranking of residency program attended, and research productivity. This was done with the chi-square test for categorical variables; the Mann-Whitney U test or the Kruskal-Wallis rank test was used for continuous variables owing to the nonnormality of the data. Similarly, we used the chi-square test to make statistical comparisons between institutions that did versus did not employ at least 1 faculty member with an advanced degree with respect to residency program ranking as well as the presence of a sports medicine fellowship. In addition, the number and percentage of advanced degrees among faculty in each residency program were compared with respect to a residency program's tier (using the Kruskal-Wallis rank test) and the presence of a sports medicine fellowship (using the Mann-Whitney U test because of the nonnormality of the data).
Among faculty comparisons, between-group differences in the demographic variables at a threshold of P < .10 were selected for multivariate analysis. To assess for independent associations between advanced degrees and outcome measures while adjusting for IMG status, binomial logistic regression was performed for dichotomous dependent variables and multiple linear regression for continuous dependent variables. These multivariate models were fixed and did not consider random effects. 24 All statistical analysis was performed using Stata version 16.1 (StataCorp) with significance set at a probability value of P < .05.
Results
Comparisons by Faculty
In total, 911 orthopaedic sports medicine faculty were identified, of whom 100 (11.0%) had an advanced degree and 811 did not (89.0%) (Table 1). There were no significant differences in the faculty groups with respect to sex, race, or type of medical degree (MD vs DO). There was a significantly higher proportion of advanced degrees among IMGs compared with graduates of US medical schools (24.4% vs 10.3%, respectively; P = .005). In terms of timing, 30.4% of advanced degrees were obtained before medical school, 28.3% were obtained during medical school, 14.1% were obtained during residency, and 27.2% were obtained after residency (Table 1).
Demographics Among Orthopaedic Sports Medicine Faculty Groups (N = 911) a
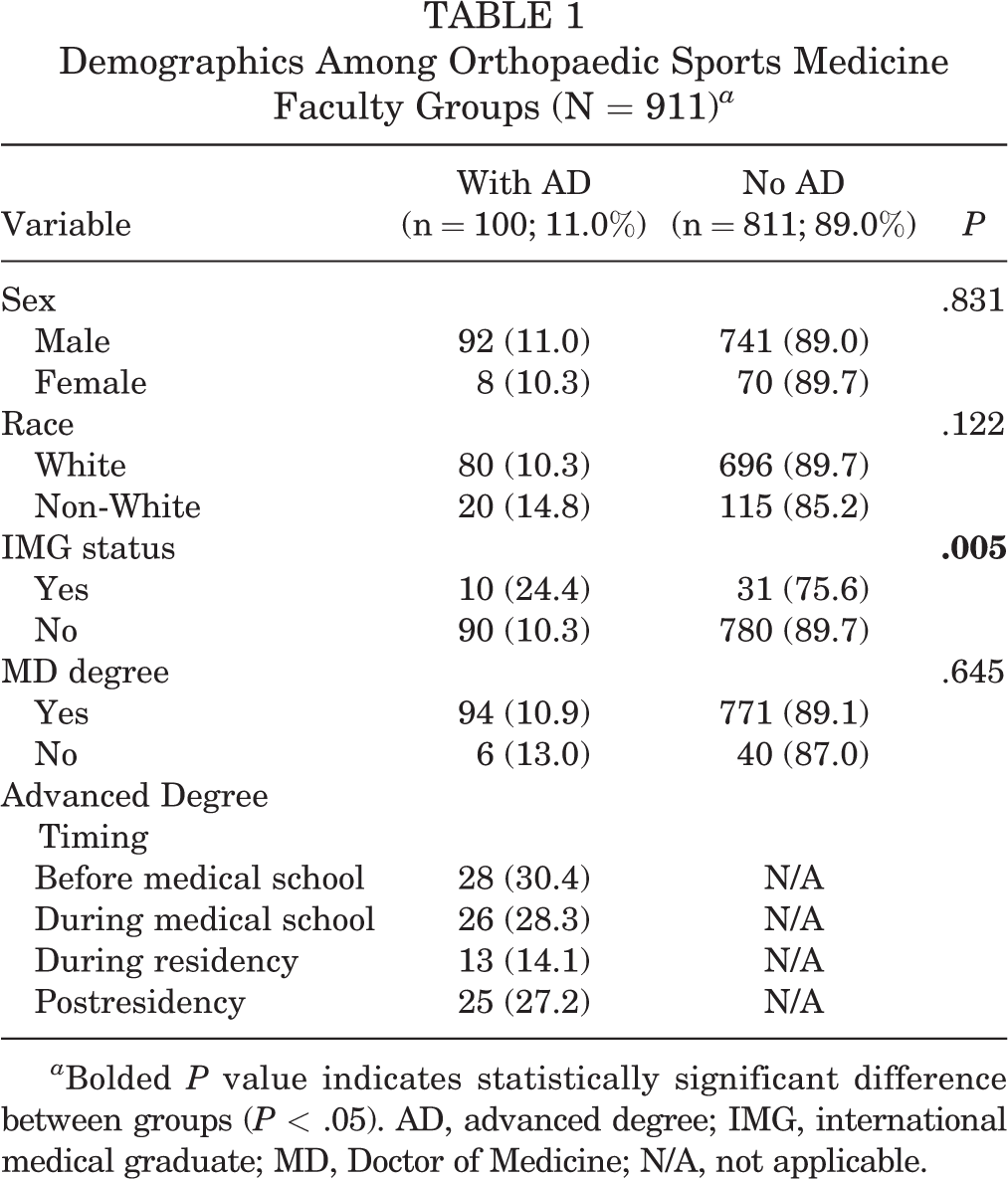
a Bolded P value indicates statistically significant difference between groups (P < .05). AD, advanced degree; IMG, international medical graduate; MD, Doctor of Medicine; N/A, not applicable.
We found an increase in advanced degrees obtained per decade, with the greatest number of advanced degrees obtained between 2000 and 2009 (33%), followed by 2010 to 2019 (31%) (Figure 1). The most popular advanced degrees among orthopaedic sports medicine faculty were MS/MSc (38%), PhD (23%), and MBA (13%) (Figure 2).

Number of obtained advanced degrees by decade.

Types of advanced degrees in orthopaedic sports medicine faculty. MA, Master of Arts; MBA, Master of Business Administration; MHS/MHA/MHSA, Master of Health Science/Master of Health Administration/Master of Science in Health Administration; MPH, Master of Public Health; MS/MSc, Master of Science; PhD, Doctor of Philosophy.
Associations between advanced degrees and outcome measures were determined after controlling for IMG status. In terms of individual faculty academic rank, there was no association between faculty having an advanced degree and professorship status (Table 2). Similarly, there were no associations between advanced degrees and status as a residency program director, fellowship program director, or chair. With respect to research productivity, faculty with advanced degrees had a significantly greater mean h-index (19.86 vs 11.55; adjusted P < .001) and more publications (80.82 vs 42.52; adjusted P < .001) than faculty without advanced degrees. In terms of editorial board positions, faculty with advanced degrees were more likely to hold at least 1 editorial board position than faculty without advanced degrees (28% vs 11.3%, respectively; adjusted P < .001). There were no associations between advanced degrees and whether the faculty member received NIH funding (Table 2).
Analysis of Faculty Members With Advanced Degrees a

a Data are reported as n (%) or mean (range). Bolded P values indicate statistically significant difference between groups (P < .05). AD, advanced degree; Adj, adjusted; NIH, National Institutes of Health.
Faculty with advanced degrees before medical school graduation were then compared with all other faculty, with the ranking of the residency program as the primary outcome. There were no significant differences in tier of residency program attended with respect to Doximity reputation ranking or Jones et al 20 research ranking among faculty who obtained an advanced degree before medical school graduation and faculty who did not have an advanced degree at medical school graduation (Table 3). Further, there were no significant associations between degree type (ie, MS/MSc, PhD, or MBA) and research outcome measures (Table 4).
Analysis of Faculty With Advanced Degrees Obtained Before Medical School Graduation a

a Data are reported as n (%). AD, advanced degree.
Subgroup Analysis by Advanced Degree Type a
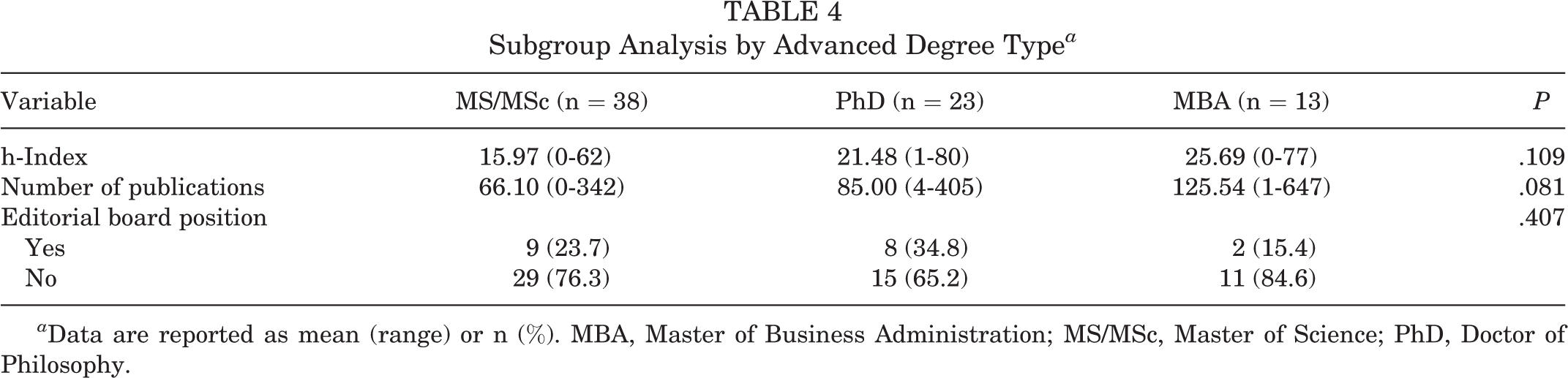
a Data are reported as mean (range) or n (%). MBA, Master of Business Administration; MS/MSc, Master of Science; PhD, Doctor of Philosophy.
Comparisons by Institution
At the institutional level, orthopaedic programs that employed faculty members with at least 1 advanced degree were more likely to be more highly ranked in terms of Doximity reputation ranking (P = .002) and Jones et al 20 research ranking (P < .001) than programs that did not employ faculty with an advanced degree (Table 5). Similarly, programs that employed faculty members with an advanced degree were more likely to have a sports medicine fellowship (62.3%) than programs without such faculty (22.1%) (P < .001) (Table 5).
Analysis of Institutions Employing Faculty With Advanced Degrees (N = 174) a

a Bolded P values indicate statistically significant difference between groups (P < .05). AD, advanced degree.
With respect to Doximity reputation rank, there was a greater mean number (1.68) and greater percentage (14.5%) of faculty with advanced degrees in tier 1 residency programs compared with tier 5 programs (0.23 and 6.3%, respectively) (P < .001) (Table 6). Similar findings were seen with Jones et al 20 research rank; there was a greater mean number (1.76) and greater percentage (15.7%) of faculty with advanced degrees in tier 1 versus tier 5 residency programs (0.25 and 5.9%, respectively) (P < .001). Overall, there was a decreasing trend in number and percentage of advanced degrees among both reputation and research residency rankings as the tier of residency program decreased (P < .001). Lastly, programs with a sports medicine fellowship had a greater mean number of advanced degrees (1.19) and a greater percentage of advanced degrees (14.14%) than programs without a sports medicine fellowship (0.23 and 6.28%, respectively) (P < .001) (Table 6).
Analysis of Institutions by Residency Programs a

a Data are reported as mean (range). Bolded P values indicate statistically significant difference between variables (P < .05). AD, advanced degree.
Discussion
The results of the present study determined that advanced degrees are associated with greater faculty engagement in research but are not associated with academic career attainment among orthopaedic sports medicine faculty. Orthopaedic sports medicine faculty with an advanced degree had greater research productivity, as shown through a greater h-index, number of publications, and number of editorial board positions. Further, there was an association between advanced degrees and status as an IMG. Notably, the match rate into orthopaedic surgery for IMGs was 22.7% in 2020, compared with 80.2% of US MD seniors. 30 Thus, it is logical that IMGs may seek to complete an additional degree to bolster their competitiveness in the match. However, the relationship between advanced degrees and research productivity remained significant even after controlling for IMG status.
Reasons for greater research productivity among faculty with advanced degrees may be seen through the most popular types of advanced degrees obtained, which were MS/MSc (38%) and PhD (23%). These degrees appeal to individuals with a natural desire and inclination to participate in scientific research, and they offer substantial knowledge in research design, methodology, and overall scientific understanding. Thus, it is understandable that these faculty members have greater research output. Notably, a subgroup analysis examining the association of advanced degree type (ie, MS/MSc, PhD, or MBA) on research productivity showed no significant association between these metrics. In general surgery, Bell et al 7 noticed that physicians with a PhD had a greater number of publications, citations, and NIH funding compared with their colleagues without a PhD. Similarly, in plastic surgery, Morris et al 28 determined that the presence of an advanced degree was associated with a greater h-index, number of publications, editorial board positions, and NIH funding. Notably, the present study did not detect an association between advanced degrees and receiving NIH funding. However, as only 9 total orthopaedic sports medicine faculty received NIH funding, the sample size may not have been powered to detect an association.
To our knowledge, while the role of advanced degrees on academic metrics and leadership has been examined in general surgery, 7 neurosurgery, 22 and plastic surgery, 28 this study is the first in orthopaedic surgery that links the presence of an advanced degree to these metrics. In addition to showing the association of advanced degrees with research productivity, Morris et al 28 noted the presence of an advanced degree was associated with matching at a higher ranked residency program but not associated with academic leadership roles in plastic surgery. In neurosurgery, Khalafallah et al 22 determined an association of a master’s degree with employment at an academic neurosurgery program, defined as an institution with a neurosurgery residency. Orthopaedic surgery differs from these other surgical specialties in key metrics, including match rates, faculty demographics, research funding, and overall scholarly productivity. 13,30,38 Owing to these differences, there is reason to believe that advanced degrees would have different associations in orthopaedic surgery. Notably, in an analysis of program directors across 11 surgical subspecialties, Patel et al 34 did note differences in the proportion of advanced degrees among these orthopaedic surgery faculty members compared with similar faculty in other surgical specialties.
The presence of an advanced degree did not confer advantages about the ranking of a residency program attended among orthopaedic sports medicine faculty. As the orthopaedic surgery residency match has become increasingly competitive, 9,23 medical students are understandably looking at ways to enhance their applications. However, the attainment of an advanced degree before medical school was not associated with matching at a higher ranked orthopaedic surgery residency program in terms of both research and reputation. Although there are many variables that factor into the orthopaedic surgery selection process, these findings suggest that advanced degrees should be driven by an intrinsic desire to add additional knowledge or skills rather than the desire to match at a higher ranked residency program.
Further, the presence of advanced degrees was not associated with academic rank and academic leadership roles among orthopaedic sports medicine surgeons. Previous studies 6,12 in orthopaedic sports medicine have examined the characteristics associated with leadership in academic rank among faculty. In an analysis of sports medicine fellowship directors, Belk et al 6 determined that greater research productivity and select residency and fellowship programs were key characteristics of sports medicine fellowship directors. Similarly, Cvetanovich et al 12 found that research productivity, but not sex or a PhD degree, was associated with academic rank among all sports medicine faculty. The results of the current study expand on the previous findings in sports medicine and demonstrate that advanced degrees appear to not confer advantages in academic rank and program leadership, including title as residency and fellowship director or department chair. Thus, at the faculty level, obtainment of an advanced degree should be driven by a desire to attain additional skills in research, hospital administration and leadership, and public health rather than the enhancement of one’s academic career.
Notably, the results of the current study determined that, at the institutional level, higher ranked residency programs and programs with a sports medicine fellowship employed more faculty members with advanced degrees. The reasons for this may be multifactorial, but programs with a greater reputation and research rank often view themselves as leaders and innovators in orthopaedic surgery. Orthopaedic sports medicine faculty with advanced degrees undoubtedly offer a diversity of knowledge and innovative skillsets that enhance the mission and goals of their department. 27,32 Whether it be through business acumen and leadership skills acquired through an MBA, 32 or an in-depth understanding of research design or methodology conferred by a PhD, 7 advanced degrees offer benefits to not only the individual orthopaedic surgeon but also the department as a whole. While this finding has not been seen in orthopaedic surgery, a recent study in plastic surgery noted this same trend. 28 Altogether, faculty with advanced degrees are an attractive asset, especially to highly ranked orthopaedic surgery programs.
Limitations
The present study is not without limitations. As the findings are associative, the specific rationale for residency program selection, academic rank, and academic leadership are unknown and subject to multiple additional criteria that cannot be accounted for in the study design. This includes potential factors such as medical school performance and standardized examination scores for residency program selection, along with personal, research, or financial interests that impact the hiring and promotion of certain orthopaedic faculty members. 9,23 Recently, Bi et al 8 noted that orthopaedic surgery chairs were more likely to be men, have a longer career, and practice sports medicine or trauma surgery as an orthopaedic subspeciality. Additional factors associated with academic leadership is beyond the scope of the current investigation but should be a direction for future studies. Further, most data were gathered through publicly accessible websites, and data for this study were accessed in March 2021. As certain information was not available for specific faculty members, and websites may be subject to inaccuracies or outdated information, this limitation could have certainly affected the results. Notably, publicly available, departmental websites for data collection and analysis have been increasingly used in high-impact studies in orthopaedic surgery and other surgical subspecialties. 6,10,28 Furthermore, as the number of advanced degrees was shown to be increasing among orthopaedic sports medicine faculty, the present study may have failed to include faculty members currently in the process of obtaining an additional degree. Lastly, there is no universal method for ranking orthopaedic surgery residency programs, and rankings are often highly variable and arbitrary. Some highly ranked residency programs may be more clinically oriented while others may be more academically oriented, thus biasing the results. However, this study used 2 previously established ranking metrics in orthopaedic surgery and obtained similar findings for both, thus lending credibility to the conclusions. 35,39
Conclusion
The current study offers the first comprehensive analysis of advanced degrees in orthopaedic sports medicine and determined that advanced degrees are associated with greater faculty engagement in research, as demonstrated by greater individual research productivity and more editorial board positions. However, advanced degrees were not associated with metrics of career attainment, including matching to a higher ranked orthopaedic surgery residency program or greater academic rank or leadership.
Footnotes
Final revision submitted October 8, 2021; accepted November 10, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.S.A. has received research support from Arthrex, Major League Baseball, and Stryker; consulting and speaking fees from Arthrex; royalties from Arthrex and Lead Player; and has stock/stock options in At Peak. W.N.L. has received education payments from Gotham Surgical and hospitality payments from Zimmer. D.P.T. has received education payments from Arthrex and Smith & Nephew. T.S.L. has received education payments from Arthrex, consulting fees from KCI USA and Smith & Nephew, and speaking fees from Arthrex, Linvatec, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.