
Abstract
Background:
It has been estimated that only 6.5% of practicing orthopaedic surgeons are female. However, with the number of women in orthopaedic surgery increasing over the past 2 decades as more female medical students are applying to orthopaedic surgery residency, it is important for trainees, mentors, and all stakeholders in the field to understand what variables affect opportunities for career advancement.
Purpose/Hypothesis:
The purpose of this study was to evaluate gender diversity among instructional course lecture (ICL) faculty at recent orthopaedic sports medicine meetings and to determine whether factors such as moderator gender affect selection of ICL panelists. It was hypothesized that there would be more female representation at orthopaedic sports medicine meetings overall compared with previous years, as well as more female faculty on ICLs with female moderators.
Study Design:
Cross-sectional study.
Methods:
Demographic data on ICL moderators and panelists were collected in September 2023 from annual meeting programs for the Arthroscopy Association of North America from 2016 to 2023 and the American Orthopaedic Society for Sports Medicine from 2018 to 2023 via an internet search.
Results:
ICLs with female moderators were more likely to include female panelists (OR, 4.6; 95% CI, 2.5-8.6; P < .0001). Male moderators had more years in practice (16.8 vs 7.2; P = .0002). Among panelists, men had higher H-indices (36 vs 23; P < .0001), a number used to describe a researcher’s productivity and impact, and years in practice (19 vs 16; P = .02). Academic ranks were significantly different between male and female moderators (P < .00001 for professor and associate professor categories). There was no significant difference in departmental leadership between male and female moderators.
Conclusion:
Female faculty were predominantly in academic practices yet were less likely to be in academic or departmental leadership roles. ICLs with a female moderator were more likely to have female panelists. Sports medicine societies should take this into account when considering ways to increase diversity among faculty on ICLs at annual meetings.
It has been well documented that more diverse health care teams lead to improvements in innovation, communication, and risk assessment as well as better patient outcomes. 7 The need for diversity has been recognized by the medical community, and efforts have been made to be more inclusive. Despite the increased female presence in medicine and the creation of pipeline programs for underrepresented minorities, some specialties, such as orthopaedic surgery, continue to lag behind, with merely 7.4% of orthopaedic surgeons in the United States reporting to be female between 2015 and 2022.6,16 Based on Association of American Colleges (AAMC) and American Academy of Orthopaedic Surgeons (AAOS) data from 2016 and 2017, it has been estimated that only 6.5% of practicing orthopaedic surgeons are female. 3 Only 11% of orthopaedic sports medicine fellowship graduates from 2016 to 2021 were female. 11 Furthermore, professional recognition and advancement have been shown to occur more slowly for women in orthopaedic surgery than in other surgical subspecialties.5,15
Medical society annual meetings are important platforms for physicians’ recognition and visibility and can be a tool for career advancement for female orthopaedic surgeons. 8 A particularly useful leadership platform at these meetings is instructional course lectures (ICLs), where faculty can be invited as moderators or panelists to discuss various topics in the field. 2 An analysis of 24 national orthopaedic surgery societies from 2020 to 2021 found both society leadership and membership to consist of homogeneously White men. 1 A study evaluating the 2012-2019 American Association of Hip and Knee Surgeons (AAHKS) annual meeting attendance demonstrated that only 2.4% of speakers were female orthopaedic surgeons. 5 Additionally, a study of gender diversity within AOSSM annual meetings found that women only represented 5.9% of moderators and course instructors from 2015 to 2019. 18 However, recognizing the importance of gender diversity at society meetings has led to efforts aimed at increasing female participation. In 2022, Wessel et al 22 evaluated faculty at American Society for Surgery of the Hand (ASSH) annual meetings and found a decrease in all-male panels from 74% in 2011 to 46% in 2021.
There have also been increasing trends of women entering the field of orthopaedic surgery. In a 2023 study by Pinpin et al, 17 there was a near doubling in the percentage of female medical students applying to orthopaedic surgery residency within the past 15 years. To strengthen this trend and create space for these upcoming female surgeons, more research is needed to assess what variables affect opportunities for career advancement, including serving as ICL faculty.14,15 The purpose of this study was to evaluate gender diversity among ICL faculty at recent orthopaedic sports medicine meetings and to determine whether factors such as moderator gender affect selection of ICL panelists. We hypothesized that there would be more female representation at AOSSM and AANA annual meetings overall compared with previous years, as well as more female faculty on ICLs with female moderators.
Methods
This was an observational study of ICL moderator and faculty demographics at annual meetings for the Arthroscopy Association of North America (AANA) and the American Orthopaedic Society for Sports Medicine (AOSSM) over the past several years. Data on ICL faculty were collected from meeting programs for AANA from 2016 to 2023 and for AOSSM from 2018 to 2023, including the 2021 AOSSM-AANA combined annual meeting. Each society was contacted to provide final programs for these meetings. The 2018 AANA meeting was excluded from the study due to an archive issue making the program unavailable. Neither association had an annual meeting in 2020 due to the COVID-19 pandemic. Data were collected in September 2023 on ICL faculty for all ICLs held at the annual meetings included in this study. Names and roles (moderator or panelist) were extracted from the meeting programs, with the first name listed for each ICL considered to be the moderator. Roundtable discussions were excluded given the lack of a clear moderator and variance from the traditional ICL format. The following data were collected for each faculty member: gender, institutional association, region of institution, practice type (academic, private practice, hospital employed, or government employed), years in practice, department leadership role (department chair, vice chair, division chief, or residency/fellowship program director or assistant director), academic rank (professor, associate professor, assistant/adjunct professor, or clinical professor), and Hirsch index (H-index). The H-index is a number used to describe a researcher’s productivity and impact based on their number of publications and how often those publications have been cited. All data were identified through publicly available information via an internet search, including university and private practice websites, personal websites, and LinkedIn profiles. Some individuals did not have a department leadership role or academic rank. ICL faculty who were not orthopaedic surgeons were excluded from the study. H-index values were gathered from Scopus, one of several databases that calculate H-indices. For those with multiple profiles identified, the highest H-index was recorded.
Statistical Analysis
To confirm appropriateness of parametric statistics for continuous data, each data set was analyzed for normality via visual inspection of histograms; secondarily, skewness and kurtosis values were calculated for each data set to confirm normality of data. Two sets of analyses were carried out on the data. First, data collected on ICL faculty from the AANA and AOSSM annual meetings were compared to determine if there was a significant difference in diversity factors between the 2 societies. The 2021 AOSSM-AANA combined annual meeting was excluded because the meeting program did not indicate that ICLs were separated by society. Chi-square analyses were performed to compare the distribution of practice type, geographic region, and title between female and male moderators and between female and male panelists. Student t tests were used to compare mean years in practice and mean H-index for female versus male moderators and panelists.
In the second set of analyses, all data collected on ICL faculty on AANA ICLs, AOSSM ICLs, and the 2021 AOSSM-AANA combined annual meeting ICLs were pooled, and the same chi-square analyses and Student t tests were performed to compare demographic factors between male and female faculty. The Z test was used to calculate the odds of including a female panelist given the gender of the moderator. The percentages of panelists with the same practice type, institution, or geographic region as their moderator were also calculated.
Results
A total of 214 ICLs conducted between 2016 and 2023 were included in the study, yielding 214 moderators and 755 panelists. This included 101 AOSSM ICLs, 90 AANA ICLs, and 23 ICLs from the 2021 AOSSM-AANA combined annual meeting. Overall, 33.6% (n = 72) of ICLs had a female faculty member (moderator or panelist); 18 moderators (8.4%) and 70 panelists (9.3%) were female. Seven AOSSM ICLs (6.9%), 8 AANA ICLs (8.9%), and 3 ICLs (13%) at the 2021 AOSSM-AANA combined annual meeting had female moderators. There were 36 (9.7%) female panelists on AOSSM ICLs, 24 (8.2%) female panelists on AANA ICLs, and 10 (9.8%) female panelists at the 2021 AOSSM-AANA combined annual meeting (Figure 1).

Female representation among moderators and panelists at Arthroscopy Association of North America (AANA), American Orthopaedic Society for Sports Medicine (AOSSM), and 2021 AOSSM-AANA combined annual meeting instructional course lectures (ICLs).
AOSSM Versus AANA
There was no significant difference in gender makeup between AOSSM and AANA ICL moderators over the study period (P = .61) (Table 1). There was also no significant difference in geographic region distribution, academic rank, departmental leadership, or mean years in practice between the ICL moderators of the 2 societies. The distribution of practice types among moderators was significantly different between AOSSM and AANA ICLs (P = .009), with AOSSM ICL moderators being mostly in academic (n = 84; 83.2%) and hospital-based (n = 12; 11.9%) practices, while AANA ICL moderators were mostly in academic (n = 66; 73.3%) and private (n = 17; 18.9%) practices. AOSSM moderators had a higher mean H-index than AANA moderators (34.1 vs 28.8; P = .04), and this difference was still observed when comparing just female moderators between the 2 societies (31.1 vs 24.5; P = .005). There was no difference in mean H-index between male moderators in AOSSM ICLs compared with those in AANA ICLs. Female AOSSM ICL moderators were more likely than female AANA ICL moderators to have female panelists (11 vs 5; P < .0001).
AOSSM and AANA ICL Moderator Demographics, Categorized by Society—Excluding 2021 Combined Meeting a

Data are presented as n (%) unless otherwise indicated. Bold P values indicate statistical significance. Dashes indicate 0 value or no P-value calculated. AANA, Arthroscopy Association of North America; AOSSM, American Orthopaedic Society for Sports Medicine; ICL, instructional course lecture.
H-index obtained per Scopus.
There was no significant difference in gender makeup between AOSSM and AANA ICL panelists over the study period (P = .5), nor were there differences in practice type, academic rank, or departmental leadership between the ICL panelists of the 2 societies (Table 2). The distribution of geographic region among panelists was significantly different between AOSSM and AANA ICL faculty (P = .014). AOSSM panelists had the most representation from the Northeast (n = 111; 29.8%) and the Midwest (n = 87; 23.4%), while AANA panelists were mostly from the Northeast (n = 90; 30.9%) and the West (n = 73; 25.1%). There was no difference in mean years in practice between panelists overall in AOSSM ICLs compared with AANA ICLs; however, female AOSSM panelists had more years in practice compared with their AANA counterparts (17 vs 13 years; P < .0001). AOSSM panelists had a higher mean H-index than AANA panelists (38 vs 32.1; P < .001).
AOSSM and AANA ICL Panelist Demographics, Categorized by Society—Excluding 2021 Combined Meeting a
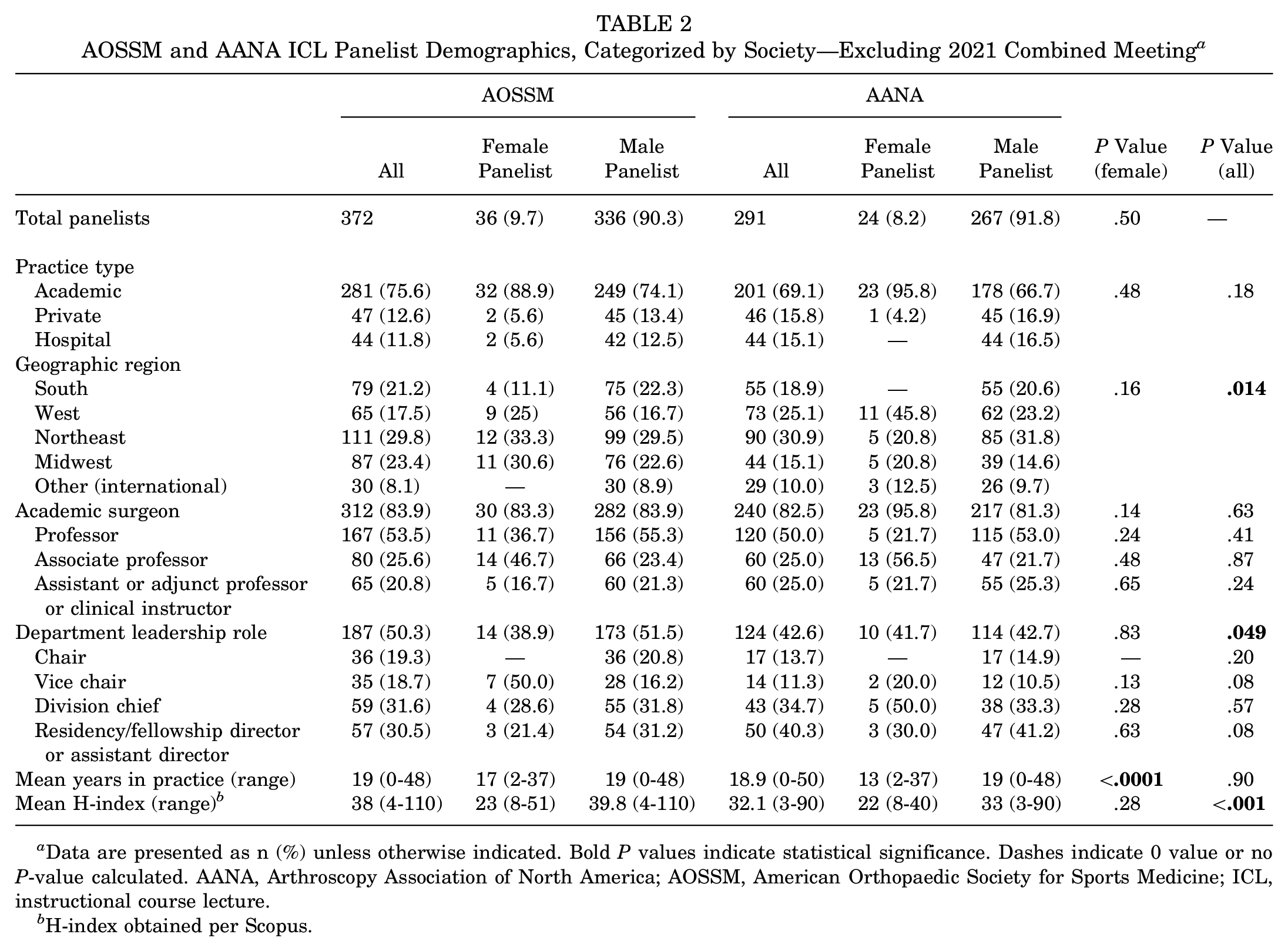
Data are presented as n (%) unless otherwise indicated. Bold P values indicate statistical significance. Dashes indicate 0 value or no P-value calculated. AANA, Arthroscopy Association of North America; AOSSM, American Orthopaedic Society for Sports Medicine; ICL, instructional course lecture.
H-index obtained per Scopus.
Pooled Data
The congruence of panelist demographics with moderator demographics was compared. ICLs with female moderators were more likely to have female panelists (OR, 4.6; 95% CI, 2.5-8.6; P < .0001) (Figure 2). A mean of 6.7% (n = 45; range, 0%-75%) of panelists in a given ICL were from the same institution as their moderator, a mean of 32.9% (n = 237; range, 0%-100%) of panelists were from the same geographic region as the moderator, and a mean of 63.8% (n = 488; range, 0%-100%) of panelists were from the same practice type as the moderator.

Gender makeup of panelists for American Orthopaedic Society for Sports Medicine and Arthroscopy Association of North America instructional course lectures with male versus female moderators.
Among moderators, men did not have a statistically significantly higher H-index than women (31.3 vs 28.2; P = .48), but they did have more than twice as many years in practice (16.8 vs 7.2 years; P = .0002). Practice type for male versus female moderators was not significantly different (P = .07), but it is notable that all female moderators practiced in an academic setting. The distribution of geographic region of affiliated institutions for female versus male moderators was not significantly different. Interestingly, 16 male moderators (8.2%) were from outside of the United States, while all female moderators were affiliated with institutions within the United States. Academic ranks were significantly different between male and female moderators (P < .00001 for professor and associate professor categories), with 16 female moderators (88.9%) being associate professors and the remaining 2 female moderators (11.1%) being assistant/adjunct professors. No female moderators were full professors. Most male moderators were professors (n = 80; 49.4%) or associate professors (n = 49; 30.2%). There was no significant difference in departmental leadership between male and female moderators (P = .49). However, there were no female moderators who were department chairs or vice chairs. A summaries of moderator demographics is provided in Table 3.
AOSSM and AANA ICL Moderator Demographics: Pooled Data a

Data are presented as n (%) unless otherwise indicated. Bold P values indicate statistical significance. Dashes indicate 0 value or no P-value calculated. AANA, Arthroscopy Association of North America; AOSSM, American Orthopaedic Society for Sports Medicine; ICL, instructional course lecture.
H-index obtained per Scopus.
Among panelists, men had higher H-indices (36 vs 23; P < .0001) and more years in practice (19 vs 16 years; P = .02) than their female counterparts. Practice type, geographic region, academic rank, and departmental leadership for the department chair and vice chair categories were significantly different between male and female panelists (P < .01 for all categories). Female panelists had higher representation in academia compared with male panelists (91.4% vs 69.6%; P = .0006). Most female panelists were from the West (n = 23; 32.9%), Northeast (n = 21; 30%), and Midwest (n = 18; 25.7%), with only 5 (7.1%) female panelists coming from the Southern region, whereas male panelists had more representation in the Southern region (21.9% vs 7.1%). In total, 36 (51.4%) female panelists had an academic rank versus 565 (82.5%) male panelists (P < .00001). Seventeen (47.2%) female panelists were associate professors, assistant/adjunct professors, or clinical instructors versus 259 (45.8%) male panelists, and 19 (52.8%) female panelists were full professors versus 306 (54.2%) male panelists. No female panelists were department chairs (Table 4).
AOSSM and AANA ICL Panelist Demographics: Pooled Data a
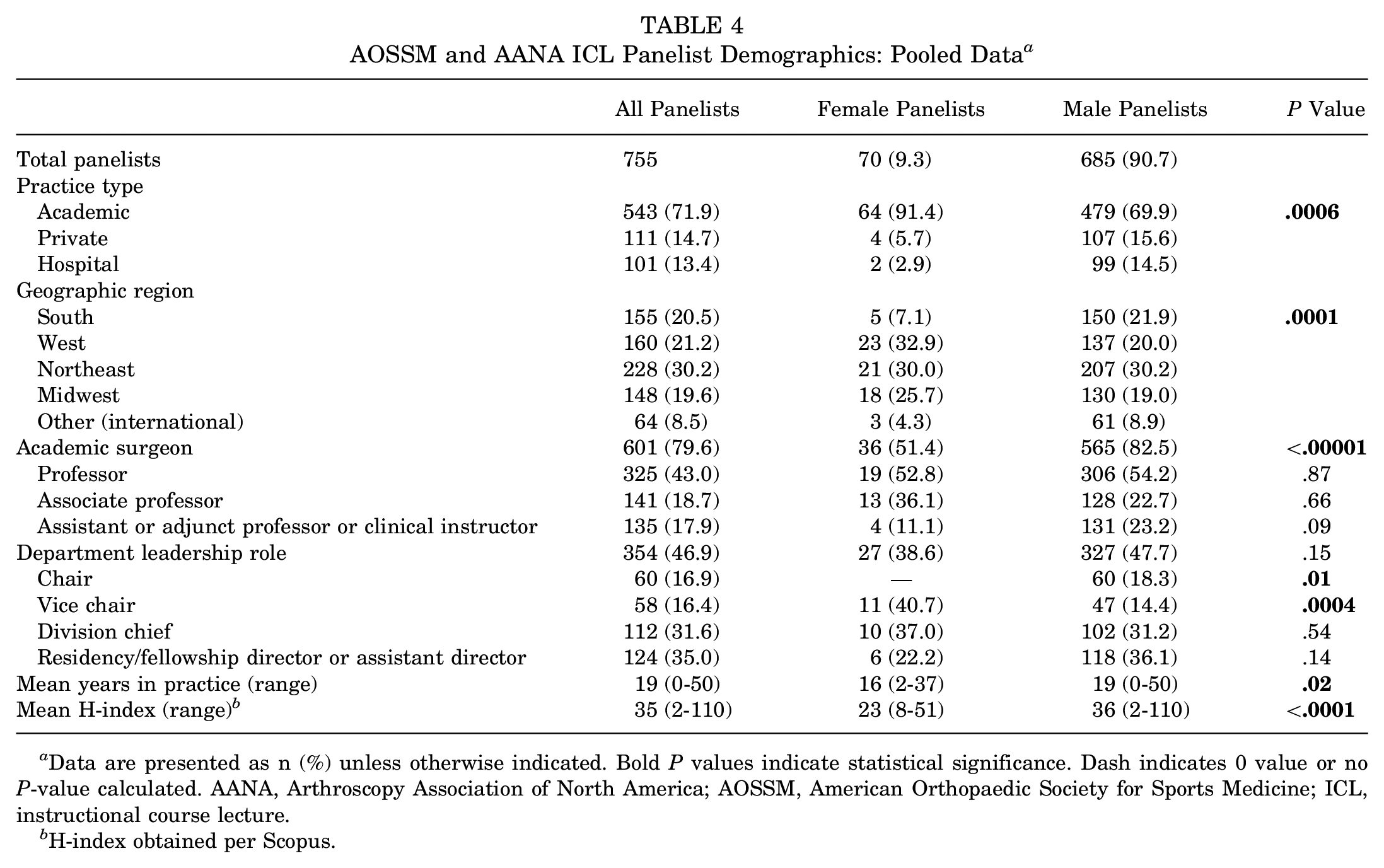
Data are presented as n (%) unless otherwise indicated. Bold P values indicate statistical significance. Dash indicates 0 value or no P-value calculated. AANA, Arthroscopy Association of North America; AOSSM, American Orthopaedic Society for Sports Medicine; ICL, instructional course lecture.
H-index obtained per Scopus.
Discussion
The purpose of this study was to evaluate gender diversity among ICL faculty at recent orthopaedic sports medicine meetings and to determine whether factors such as moderator gender or panelist practice type affect the selection of ICL panelists. In this analysis of ICLs at AOSSM and AANA annual meetings between 2016 and 2023, 18 (8.4%) moderators and 70 (9.3%) panelists were women, and ICLs with a female moderator were found to be more likely to have female panelists (P < .0001). There was a geographic component to gender representation as most female panelists were from the West, Northeast, and Midwest, with little representation from the South compared with men (7.1% vs 21.9%). Additionally, with 64 (91.4%) female panelists and all female moderators being in academia, women had stronger representation in academic practice, yet held lower academic rank and department leadership roles than their male counterparts. Male ICL faculty were found to have a greater number of years in practice (16.8 vs 7.2 years [P = .0002] for moderators; 19 vs 16 years [P = .02] for panelists).
A study of AANA and AOSSM membership and leadership between 2010 and 2020 found that there was greater female representation in 2020 compared with 2010 for both societies. 20 In AANA, female representation increased from 5% to 10%, and in AOSSM it increased from 8% to 14%. 20 A 2021 study by Potter et al 18 evaluated female representation at AOSSM annual meetings between 2015 and 2019. In their study, 21 (7.2%) moderators and 31 (5.2%) course instructors were female. The authors hypothesized that these numbers would increase based on the AAMC report indicating that 12.1% of orthopaedic surgeons on track to complete an orthopaedic sports medicine fellowship in 2018 were female. 18 When analyzing both AOSSM and AANA annual meetings, our study found increased female participation, with 18 (8.4%) female moderators and 70 (9.2%) female panelists between 2016 and 2023 compared with the 2021 study, which is an encouraging trend in accordance with the previous study’s prediction.
Other orthopaedic subspecialties have also investigated gender diversity. A study by Jacobson et al 10 compared female representation among surgeons who were invited to speak at meetings of the American Association for Hand Surgery (AAHS) and American Society for Surgery of the Hand (ASSH) in 2010 and 2020 and found that although there have been improvements in gender diversity, female surgeons remain underrepresented. An investigation of gender diversity in the American Orthopaedic Foot and Ankle Society (AOFAS) found that female leadership through committee membership has increased from 7.5% to 13% between 2012 and 2022. 4 However, an assessment of 10 subspecialty annual meetings in 2021, including the AAHKS, AAHS, American Academy of Orthopaedic Surgeons (AAOS), AOSSM, Canadian Orthopaedic Association, European Federation of National Associations of Orthopaedics and Traumatology, North American Spine Society, Orthopaedic Research Society, Orthopaedic Trauma Association, and Pediatric Orthopaedic Society of North America, found that 58.5% of panels had all male speakers and 12.6% of faculty members were women, reflecting a persistently inadequate representation of female orthopaedic surgeons at orthopaedic society meetings. 21
Our study also found that female moderators were more likely to include female panelists on their ICLs. This is corroborated by previous studies that have consistently demonstrated the role female mentorship plays in increasing gender diversity in orthopaedic surgery. In 2018, Sobel et al 19 found an increased number of female residents in orthopaedic surgery residency programs with a greater number of female faculty and more women in leadership positions. Additionally, a survey of orthopaedic surgery residents by Hill et al 9 demonstrated that female residents were more likely than male residents to be interested in orthopaedic surgery due to having mentors of the same gender. Our findings indicate that this female mentorship role could very well extend past the resident level with more senior female orthopaedic surgeons opening a space for their upcoming female peers at the faculty level in national society meetings.
A 2022 study by Peterman et al 16 described a “trailblazer effect,” in which female leadership increases female representation, when analyzing the geographical distribution of female orthopaedic surgeons in the United States. In that study, the authors found that areas of the country with higher numbers of female orthopaedic surgeons were quicker to increase female representation. Interestingly, in that geospatial analysis, there were gender diversity “hot spots” in the Northwest, Northeast, and Southwest, with relatively less diversity in the Midwest and Southern United States, which was similar to the distribution of female panelists in our study, who were primarily from the West and Northeast, with fewer from the South. This geographic trend can be attributed to a higher presence of female mentorship and leadership in those areas.
We found significant gender disparity in academic rank and division leadership. Despite 91.4% (n = 64) of female panelists and 100% (n = 18) of female moderators being in academic practice, there were no female moderators who were department chairs or vice chairs, while 60 (30.6%) male moderators served as a department chair, vice chair, or division chief. The trend was similar in academic rank, with no female moderators and only 19 (27.1%) female panelists being full professors versus 80 (40.8%) male moderators and 306 (44.7%) male panelists being full professors. These trends are consistent with previous findings that female sports medicine surgeons may be drawn to academic practices with opportunities for involvement in residency education and leadership. In a 2022 study of AAMC medical school faculty rosters and the 2016 AAOS member census, Kuhns et al 12 found markedly increased female representation in the academic setting compared with the total orthopaedic surgeon workforce. This is an encouraging sign that gender trends in orthopaedic sports medicine may be changing, as previous studies have demonstrated female medical students being more likely to apply to orthopaedic surgery residency if they attend an institution with greater resident and faculty gender diversity in orthopaedics. 13 As in this study, despite increased involvement in academia, the 2022 Kuhns et al 12 study found that female orthopaedic surgeons were proportionally less likely to be full professors compared with their male counterparts. The authors noted that the decreased female representation among full professors may be due to overall shorter time in practice of female surgeons, which reflects our study’s findings that among moderators and panelists, men had a greater mean number of years in practice.
Overall, our study shows a modest but promising increase in female representation within orthopaedic sports medicine society ICLs, yet a disproportionately small amount of representation at the academic or department leadership level. This is important because increased representation of female orthopaedic surgeons in leadership roles is likely to improve the diversity of medical students considering a career in orthopaedic surgery, particularly in academic settings, if students gain the opportunity to engage with these mentors. When creating panels for ICLs, we encourage those involved to consider potential intrinsic biases and entrenchment in historical trends that may affect how candidates are chosen for leadership roles in orthopaedic sports medicine societies.
There are several limitations to this study. With regard to data collection, our ability to obtain annual meeting programs was determined by archive availability. Data on surgeon background such as institution, years in practice, departmental leadership role, and academic rank were obtained via an internet search; as such, there are inherent limitations to the accuracy of data collected. There were several instances of institution or practice change among surgeons over the study period, although efforts were made to record data that were accurate for the surgeon at the time of the ICL. Additionally, the analysis of moderator differences was limited by the relatively small sample size of female moderators. Lastly, a few ICLs were given multiple times at different meetings over the years with similar panels.
Conclusion
Female faculty ICL representation at AOSSM and AANA annual meetings has been increasing over the past several years. Female faculty were predominantly in academic practices yet were less likely to be in academic or departmental leadership roles. ICLs with a female moderator were more likely to have female panelists. Sports medicine societies should take this into account when considering ways to increase diversity among faculty on ICLs at annual meetings.
Footnotes
Final revision submitted December 18, 2024; accepted February 3, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.K.M. is a board or committee member of the American Academy of Orthopaedic Surgeons, American Orthopaedic Association, American Orthopaedic Society for Sports Medicine, Arthroscopy Association of North America, Association of Bone and Joint Surgeons, Ruth Jackson Orthopaedic Society, and International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine; an editorial or governing board member of American Journal of Sports Medicine electronic media, Arthroscopy, Journal of Bone & Joint Surgery–American, and OrthoInfo; and a paid consultant and paid presenter or speaker for Arthrex Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.