
Abstract
Background:
Research productivity is considered an important factor in academic advancement in sports medicine. No study to date has evaluated academic productivity and correlates of academic rank for sports medicine fellowship faculty.
Purpose:
To describe the academic productivity of American Orthopaedic Society for Sports Medicine (AOSSM) fellowship program faculty and to determine the association between academic productivity, fellowship characteristics, and academic rank.
Study Design:
Descriptive epidemiology study.
Methods:
Characteristics of orthopaedic sports medicine fellowship programs were obtained from the AOSSM and program websites. Metrics of academic productivity (Hirsch index [h index], I-10 index, publications, citations, and number of publications in several journals) were obtained from Scopus. Statistical analyses were conducted to determine whether academic productivity differs with fellowship attributes and academic rank.
Results:
A total of 90 AOSSM sports medicine fellowship programs with 610 associated faculty members were identified. Faculty were predominantly male (94%), at academic medical centers (74%), members of AOSSM (71%), and sports medicine–fellowship trained (84%). Faculty had a median of 18 (range, 0-684) publications overall, including a median of 3 (range, 0-161) publications since 2012. All measures of academic productivity were significantly higher among faculty employed at academic medical centers compared with those not employed at academic centers (P < .05 in all cases). On multivariate ordinal regression analysis, the best correlates of higher academic rank were higher cumulative h index (1.22; P < .001) and longer time in practice since fellowship (1.14; P < .001), which predicted 63.8% of the variance in academic rank. Fellowships with a larger number of fellows had more publications and citations per faculty member, higher faculty cumulative h index, and more publications in the American Journal of Sports Medicine and Arthroscopy per faculty member (P < .017). Regional differences were present, with the Northeast fellowship faculty the most productive, followed by the Midwest.
Conclusion:
Higher cumulative h index and more years in practice were the best correlates of higher academic rank among AOSSM sports medicine fellowship faculty. Research productivity was higher among faculty employed at academic centers in the Northeast and Midwest regions and at programs with a larger number of fellows.
Sports medicine and arthroscopy continues to be a popular fellowship choice for graduating orthopaedics residents; in 2015, those programs participating in the SF Match Residency and Fellowship Matching Services represented 220 accredited positions, of which 89% were filled and with 84% of programs matching in full. 19 Sports-related procedures continue to increase: For example, the incidence of anterior cruciate ligament reconstruction (ACLR) in the United States has risen from 86,687 (32.9 per 100,000 person-years) in 1994 to 129,836 (43.5 per 100,000 person-years) in 2006. 13 Surgical procedures addressing cartilage defects in the knee were performed in 1,959,007 patients between 2004 and 2011, with a mean annual incidence of 90 surgeries per 10,000 patients and a growing incidence annually of 5% over that time. 14 Young orthopaedic surgeons continue to use sports medicine fellowship opportunities to not only refine their surgical skills to meet this growing demand but additionally to promote research initiatives to facilitate future advancements in the field of sports medicine.
Sports medicine fellowship programs commonly provide research opportunities or requirements for fellows. Research is crucial for the improvement of the evaluation, understanding, and treatment of orthopaedic pathology. Research productivity is thus often considered a prerequisite for academic advancements for fellows and faculty in tenure-track positions, although many institutions are now instituting clinical tracks with less emphasis on research productivity. Beyond simple metrics such as total number of publications and publications in top journals, academic productivity is increasingly measured by more sophisticated metrics combining number of publications and citations to better reflect research impact. Journals increasingly emphasize publication quality based on factors including level of evidence 2 as well as Impact Factor (Thomson-Reuters), which reflects the average number of citations per publication within the journal. Similarly, the Hirsch index (h index) measures individual researcher scientific impact based on number of publications and frequency of citations for each publication. 5,6 The h index is calculated using a formula that determines the maximum number h for which the researcher has published at least h papers with at least h citations each. 5,6 This index is used by institutional promotion committees and has been associated with academic promotion in surgical disciplines, including hand surgery, 11 spine surgery, 18 urology, 1 neurosurgery, 8,10 oral and maxillofacial surgery, 20 and plastic surgery. 4
To our knowledge, no study to date has evaluated academic productivity and correlates of academic rank for sports medicine fellowship faculty. As these statistics differ from specialty to specialty, it is useful to provide specialty-specific statistics to allow benchmarking. In addition, sports medicine fellowships differ from other subspecialty fields in that many fellowships are based within private practices and not within academic departments. However, many private practice–based sports medicine fellowships have fellows who produce significant research. Thus, subspecialty-specific differences might be expected given that fellowship staff may be less motivated by academic advancement. We therefore aimed to describe the academic productivity of American Orthopaedic Society for Sports Medicine (AOSSM) sports medicine fellowship faculty and to determine associations between academic productivity, fellowship characteristics, and academic rank.
Methods
Data Collection: Identification of Fellowship Faculty and Faculty Demographics
We identified current AOSSM sports medicine fellowship programs using the AOSSM fellowship website (https://www.sportsmed.org/AOSSMIMIS/Applications/Fellowship_Listing.aspx), accessed on September 17, 2015. For each fellowship, the AOSSM website and the individual programs’ websites were evaluated to determine fellowship faculty members. To focus on sports medicine orthopaedic surgeons, those faculty with primary care sports medicine training and individuals not involved in clinical medicine (such as PhD research faculty) were excluded. Fellowship program features were extracted, including academic affiliation and number of fellowship positions. Fellowship faculty demographics were extracted from departmental websites and the AOSSM member directory, including sex, fellowship training (none, sports medicine, or other), presence of PhD degree, years since completion of training, AOSSM membership status, academic affiliation, academic rank (none, instructor or assistant professor, associate professor, and full professor), director of fellowship program, department chairman, and current or former AOSSM president status. Whether faculty were in a clinical or tenure track position was not considered since this information was inconsistently reported on the websites.
Data Collection: Academic Productivity Metrics
Academic productivity metrics were obtained using the Scopus commercially available index of publications and citations (Reed-Elsevier) on September 17, 2015. This included total number of publications; number of publications since January 1, 2012; cumulative h index; h index for January 1, 2012 to present; I-10 index; total number of citations; number of citations since January 1, 2012; maximum number of citations of a single work; and number of publications in select high-impact journals relevant to sports medicine surgery (American Journal of Sports Medicine [AJSM]; Arthroscopy; Journal of Shoulder and Elbow Surgery [JSES]; Journal of Bone and Joint Surgery, American Edition [JBJS]; and Clinical Orthopaedics and Related Research [CORR]). The I-10 index is defined as the number of publications with 10 or more citations. 9
Statistical Methods
All analyses were conducted in Excel X (Microsoft Corp) and SPSS 22 (IBM Corp). First, descriptive statistics (mean and 95% CI) were calculated. Univariate analyses were then conducted to determine whether (1) sex, (2) PhD status, (3) sports fellowship training, (4) number of fellowships performed, (5) years since fellowship, (6) AOSSM membership, (7) being fellowship director, (8) being section director, (9) being department chairman, (10) being past or present president of the Arthroscopy Association of North America (AANA), (11) being past or present president of AOSSM, (12) number of publications, (13) number of publications in AJSM, (14) number of publications in JSES, (15) number of publications in Arthroscopy, (16) number of publications in JBJS, (17) number of publications in CORR, (18) total number of citations, (19) h index, (20) maximum number of citations of a single work, or (21) I-10 index differed between academic ranks. For categorical variables, chi-square and Fisher exact tests were used as appropriate depending on cell populations. For continuous variables, analysis of variance tests or Kruskal-Wallis tests were used as appropriate depending on data normality as determined with the Kolmogorov-Smirnov test. Multivariate ordinal regression was then performed to determine the best correlates of academic rank using the Nagelkerke method of estimating R 2. Academic productivity was also compared between faculty employed at academic centers and those not employed at academic centers. An analysis of regional variations in academic productivity was then performed.
While all previous analyses were conducted on a per-individual basis, we then performed several analyses on a per-institution basis. Spearman correlation coefficients were calculated between academic productivity variables and fellowship size. Number of fellowship spots and dedicated research time were also compared between regions. In all cases, a P value of <.05 was used to determine statistical significance.
Results
A total of 90 sports medicine fellowships were identified with 610 associated faculty members, most of whom were male, sports fellowship–trained, AOSSM members. A minority had additional training with a PhD (12; 2%), a shoulder fellowship (43; 7%), a hand fellowship (8; 1%), a trauma fellowship (17; 3%), an adult reconstruction fellowship (12; 2%), a pediatrics fellowship (15; 3%), or a foot and ankle fellowship (11; 2%). Most surgeons (502; 82%) had undergone a single fellowship, with 51 (8%) undergoing 2 fellowships, 3 (1%) undergoing 3 fellowships, and 1 (0.2%) undergoing 4 fellowships. Demographic and publication statistics for each academic rank as well as for the average academic sports surgeon are provided in Table 1 and Figure 1. The mean h index for AOSSM sports medicine fellowship faculty was 15 (95% CI, 13-17).
Demographic and Academic Productivity Statistics by Academic Rank a

a All results are shown as mean per person (95% CI) unless otherwise indicated. AJSM, American Journal of Sports Medicine; AOSSM, American Orthopaedic Society for Sports Medicine; CORR, Clinical Orthopaedics and Related Research; JBJS, Journal of Bone and Joint Surgery; JSES, Journal of Shoulder and Elbow Surgeons.

Mean total number of publications, cumulative h index, and maximum citations of a single work for assistant, associate, and full professors. Errors bar demonstrate 95% CI. There was a statistically significant difference between groups in each case (P < .001).
In univariate analysis, while sex, PhD status, sports fellowship training, number of fellowships performed, and current or former AANA presidency did not differ between academic ranks, all other measures of academic productivity sequentially and significantly increased with academic rank (P < .005 in all cases) (Table 1). On multivariate analysis, the best correlates of academic rank were higher cumulative h index and longer time in practice since fellowship (Table 2). Once these 2 variables were accounted for, no other measures of academic productivity were significant correlates of academic rank. A model constructed with these variables predicted R 2 of 63.8% of the variance in academic rank.
Multivariate Ordinal Regression Modeling to Determine Correlates of Academic Rank a

a AOSSM, American Orthopaedic Society for Sports Medicine.
Of the 610 included surgeons, 453 (74%) were employed at an academic center and 157 (26%) were not. All measures of academic productivity were higher among those with academic employment, and the difference was significant in most cases, with the exception of maximum citations of a single work (Table 3).
Academic Productivity by Academic or Nonacademic Affiliation a

a All results are shown as mean per person (95% CI). AJSM, American Journal of Sports Medicine; CORR, Clinical Orthopaedics and Related Research; JBJS, Journal of Bone and Joint Surgery; JSES, Journal of Shoulder and Elbow Surgeons.
The included surgeons were spread throughout the country, with 148 (24%) residing in the Midwest, 184 (30%) residing in the Northeast, 147 (24%) residing in the South, and 131 (22%) residing in the West. Most measures of academic productivity, including number of publications, cumulative h index, h index since 2012, I-10 index, total citations, citations since 2012, number of AJSM publications, and number of JBJS publications, varied significantly between regions (P < .05) (Table 4). The Northeast was the most productive, followed by the Midwest, the West, and then the South. Other measures, including number of publications since 2012, maximum number of citations of a single work, number of Arthroscopy publications, number of CORR publications, and number of JSES publications, did not vary across regions.
Academic Productivity by Region a
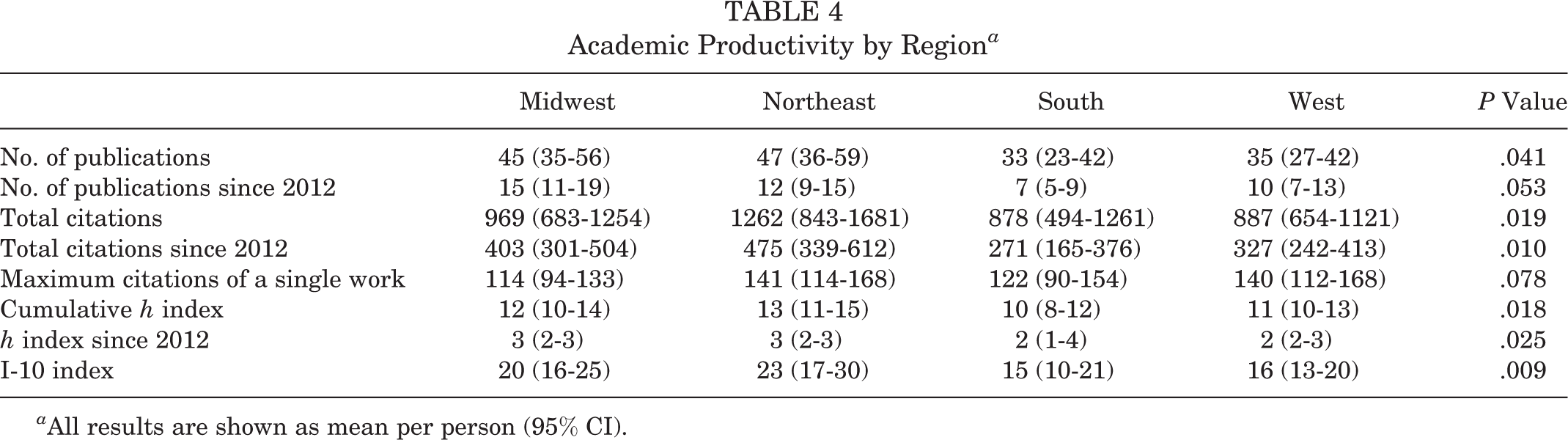
a All results are shown as mean per person (95% CI).
When viewed by program, most programs had an academic affiliation (65; 72%) and dedicated research time (36; 52%). Most (71; 78.9%) had 1 to 3 fellow positions, with 1 program having 1 nonaccredited fellowship spot and 1 having 2 nonaccredited fellowship spots. Fellowship size positively correlated with almost all measures of academic productivity (P < .017) except for h index since 2012, number of publications since 2012, number of JSES publications, and number of JBJS publications (P > .053). The presence of dedicated research time did not differ between regions (P = .726), being present in 64% of programs in the West, 52% of programs in the South, 50% of programs in the Northeast, and 44% of programs in the Midwest. Number of fellowship spots per program did differ significantly across regions (P = .042), with the largest programs being located in the South (2.8 [95% CI, 2.3-3.3]), West (2.7 [95% CI, 1.9-3.4]), and Northeast (2.6 [95% CI, 2-3.1]), and the smallest programs being located in the Midwest (1.9 [95% CI, 1.4-2.4]).
Discussion
New metrics of publication productivity such as Impact Factor for journals and h index for individuals are increasingly utilized to predict and determine academic promotion in a variety of surgical disciplines. 1,4 –6,8 –11,15,18,19 We present the first analysis of academic productivity of AOSSM sports medicine fellowship faculty. Multivariate analysis revealed that independent factors predictive of higher academic rank were higher cumulative h index and more years in practice.
We found that faculty employed at academic centers had greater academic productivity than faculty not employed at such centers. The reasons for this may include an emphasis on publications in the academic setting for promotion as well as the productivity boost provided by residents, fellows, and other institutional academic supports that assist academic faculty in producing research. Certainly, a selection bias also exists. The finding that h index—rather than simpler metrics such as number of publications or number of citations—is strongly associated with academic rank for sports medicine fellowship faculty is similar to Lopez et al 11,20 for hand fellowship faculty and findings in other surgical disciplines. 1,10
In addition to higher cumulative h index, multivariate ordinal regression showed that more years in practice was the key factor predicting academic rank. Number of years in practice is intuitively associated with academic rank based on typical promotion criteria, and this factor has similarly been identified in other studies such as that by Lopez et al 11 for hand fellowship faculty. AOSSM membership tended to be associated with higher academic rank, analogous to Lopez et al, 11 who found that American Society for Surgery of the Hand membership was associated with rank for hand fellowship faculty, but was not significant on multivariate modeling. This could relate to younger faculty not yet meeting AOSSM membership criteria. A model with h index and numbers of years in practice predicted 63.8% of variance in academic rank in sports medicine fellowship faculty.
The mean h index for AOSSM sports medicine fellowship faculty was 15 (95% CI, 13-17). This compares favorably to other specialties analyzed with h index in orthopaedics, including a mean h index of 13.2 for spine fellowship faculty 18 and 10.2 for hand fellowship faculty. 11 This also compares favorably to other surgical specialties, with a mean h index of 14 for academic neurosurgeons, 8 7 for academic plastic surgeons, 4 and 15 for academic urologists. 1 Comparisons between specialties, especially dissimilar specialties, with regard to research and publication should be interpreted with caution as the definition of research productivity and therefore the mark of a “successful” h index might vary widely. Hirsch 5 found that the h index of top biologists often exceeded 150, higher than the top physicists and other disciplines. For instance, our highest h index was 87. Because these measures of academic productivity differ between specialties, our data provide benchmark statistics of interest to sports medicine surgeons and fellows.
We found that academic productivity is higher in academic centers, in the Northeast and Midwest regions, and at programs with a larger number of fellows. Multiple factors likely impact regional variations, including the age of the institutions with which faculty are associated, cultural factors, research facilities and faculty, differences in the prevalence of managed care organizations, and population density. Given the unexpected size of variations between regions, institutions may consider comparing themselves against regional norms in addition to national norms. Programs with more fellows might have greater research productivity as a result of fellow-driven research ideas and manpower. In addition, institutions with large fellowship programs may have a greater focus on academic aspects of sports medicine including research productivity and fellow education.
Several prior studies have identified associations between sex, academic productivity metrics such as the h index, and academic rank in surgical disciplines. 3,12,16,23 Women were underrepresented at only 7% of AOSSM sports medicine fellowship faculty in this analysis. In contrast to some other surgical disciplines, we found no difference in academic rank (P = .187) or h index by sex, although the study is underpowered to perform this analysis because of the small numbers of female sports medicine surgeons. It is also worth noting that academic rank may have less financial benefit in orthopaedic sports medicine than other disciplines because clinical activities usually account for the majority of income.
This study has limitations. We focused our analysis on surgeons affiliated with AOSSM sports medicine fellowship programs and did not analyze a broader population of sports medicine surgeons such as all fellowship-trained sports medicine surgeons or all AOSSM members. Although this limits our findings to sports medicine fellowship faculty only, we felt that limiting analysis to this group would be most relevant to sports medicine research, which is preferentially performed at programs with fellowships, while still allowing comparison of academic and nonacademic programs as well as fellowship factors associated with research productivity. We were not able to compare tenure-track versus clinical faculty, who have differential emphasis on research productivity for academic promotion. Second, by virtue of study design, we relied on website information, which can be imperfect. We attempted to mitigate this limitation by checking information from AOSSM websites as well as individual departments and sports medicine fellowship programs. Future studies could confirm these findings with surveys to directly collect data from the institutions themselves. Third, we did not consider author position or number of authors, even though certain publication positions might reflect a greater contribution to the research project and manuscript than others. Fourth, the associations we find, even on multivariate regression, do not necessarily reflect a causative effect between variables and academic rank, and unmeasured confounding factors could be at play. Fifth, we did not consider other indices of academic productivity including lectures, national presentations, and visiting professorships. We used the most common indices that would allow comparison to the relevant prior literature, with the h index and simple citation and publication counts most widely used. 1,4 –6,8 –11,15,18,20 Addition of other indices was felt to add unnecessary complexity without additional pertinent information. Finally, there are inherent limitations of all proposed metrics of research productivity that focus on publications alone, which is why they should be used cautiously and considered in a broader context when assessing an individual’s research or considering promotion decisions. Other factors include clinical activity, teaching, service to the institution, and national service. For instance, the h index will bias toward the most senior faculty with seminal work that is repeatedly cited even if their productivity has waned in recent years. 7 Also, the h index could theoretically be artificially elevated by self-citation, but this seems to play a minor role in practice. 17,21,22 We attempted to account for limitations of these metrics by using multiple metrics as well as other faculty demographic factors in our multivariate analysis.
Conclusion
Higher cumulative h index and more years in practice were the best correlates of higher academic rank among AOSSM sports medicine fellowship faculty. Research productivity was higher among faculty employed at academic centers, in the Northeast and Midwest regions, and at programs with a larger number of fellows.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.R.B. receives research support from Arthrex Inc, Conmed Linvatec, DJ Orthopaedics, Ossur, Smith & Nephew, and Tornier. B.J.C. receives research support from Aesculap/B.Braun, Arthrex Inc, Cytori, Medipost, National Institutes of Health, and Zimmer; other financial or material support from Athletico, Ossur, Smith & Nephew, and Tornier; is a paid consultant for Athrex Inc, Regentis, and Zimmer; holds stock or stock options in Carticept, Regentis; and receives royalties from Arthrex Inc, DJ Orthopaedics, and Elsevier.
Ethical approval was not sought for the present study.