
Abstract
Background:
Reverse total shoulder arthroplasty (rTSA) is an established procedure for cuff tear arthropathy. More lateralized prostheses have been designed to overcome the reported adverse outcomes of Grammont-style rTSA.
Purpose:
To compare the clinical and radiological outcomes of medialized and lateralized center of rotation (COR) in rTSA.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
This review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Included were studies with a level of evidence ≥3 that compared medialized and lateralized rTSA with a minimum follow-up of 12 months. Functional scores including the American Shoulder and Elbow Surgeons (ASES) score and Constant score (CSS), range of motion at final follow-up, gain of external rotation (ER), visual analog scale (VAS) pain score, scapular notching, and heterotopic ossification (HO) were compared. Data were analyzed using random-effects or fixed-effects models in accordance with heterogeneity.
Results:
Five retrospective cohort studies and 1 randomized controlled study (n = 594 patients) were included. Lateralized rTSA resulted in greater improvement in ER degree (P < .001), a lower VAS pain score (standardized mean difference [SMD], –0.39; P = .002), and a lower rate of scapular notching (risk ratio [RR], 0.40; P < .001) and HO (RR, 0.52; P < .001). Final forward flexion (SMD, –0.14; P = .629) and ER (SMD, 0.21; P = .238) did not differ significantly between the 2 groups. Overall functional scores, including ASES score (SMD, 0.22; P = .310) and CSS (SMD, 0.37; P = .077), also did not differ significantly (SMD, 0.28; P = .062). The overall complication rate did not differ significantly between the 2 groups (RR, 0.71; P = .339).
Conclusion:
Compared with medialized rTSA, lateralized COR rTSA results in greater improvement in ER and the VAS pain score, decreased rates of scapular notching and HO, and no significant changes in functional outcome scores or the complication rate.
Since Paul Grammont introduced the procedure for reverse total shoulder arthroplasty (rTSA), it has become a successful treatment option for many shoulder diseases. 3,8,26 Shoulder function and range of motion (ROM) are improved in cuff tear arthropathy (CTA) and other end-stage conditions 4,15 with rTSA.
Grammont designed prostheses with a medialized, distalized center of rotation (COR) to increase the deltoid lever arm. 3 However, some adverse results have been reported after Grammont-style rTSA, such as scapular notching and a lack of improvement in ROM. 6,20,32 Shifting the COR more laterally is one method that has been attempted to address these problems. Bony increased-offset rTSA (BIO-rTSA) was introduced, in which a bone graft is used to lateralize the COR. 2 Other studies achieved prosthetic lateralization by modifying the glenoid or humeral implant design. 16,18,30
Although the amount and method of lateralization remain controversial, many studies 7,9,12 have reported advantages of lateralized rTSA in improved ROM or shoulder function over conventional medialized rTSA, while 1 study 7 has suggested similar outcomes with both methods. A few systematic reviews 1,11,13 on this topic have been published, as well as a recent a meta-analysis by Nunes et al 22 with an evidence level of 4.
The purpose of the present study was to perform a meta-analysis of the advantages and outcomes of lateralized versus medialized rTSA in studies with a high level of evidence (level, ≥3). We hypothesized that most clinical outcomes, including functional scores, ROM, and pain scores, would not differ significantly between the two, while radiological outcomes, such as scapular notching and heterotopic ossifications (HOs), would be better in the lateralized rTSA group.
Methods
Search Strategy
The PubMed, Embase, and Cochrane Central Register of Controlled Trials databases were searched for any articles published before February 27, 2021, that combined the Medical Subject Headings terms “shoulder arthroplasty,” “lateralized,” “medialized,” “lateralization,” and “medialization” with the Boolean operators “AND” and “OR.”
Study Selection
Two independent reviewers (H.-J.L. and S.-H.C.) performed a literature search for studies comparing lateralized- and medialized-design rTSA with a minimum follow-up of 12 months. Searches were conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, 19 and any disagreements between the reviewers were resolved in a discussion with the senior author (Y.-S.K.).
The inclusion criteria were English-language articles with an evidence level of 3 or higher. A preoperative diagnosis and intergroup comparison of preoperative characteristics were required, as were reporting of functional or patient-reported outcomes using at least 1 clinical score and the visual analog scale (VAS) pain score. Functional outcomes or ROM had to be reported as means and standard deviations. Glenoid or humerus component lateralization and BIO-rTSA were included. The studies that used BIO with a 1-cm autologous bone graft with the same implant were considered to be glenoid lateralization. The prostheses used were classified as either humeral or glenoid lateralization as described by Werthel et al 30 ; these authors compared the degree of glenoidal and humeral lateralization of various implants to the Delta III prosthesis (DePuy). Studies that used a prosthesis not evaluated by Werthel et al 30 were included only when they specified the degree or type of lateralization. This process is illustrated in Figure 1. Excluded were case reports, case series, editorial letters, in vitro or animal studies, and systematic reviews.

(A) Glenoidal and humeral lateralization relative to the Delta III prosthesis for each implant according to Werthel et al. 30 (B) Comparison of the medialized (M) and lateralized (L) prostheses in each study. *Studies used the Bigliani/Flatow system (Zimmer) for the medialized group and Encore (DJO Global) for the lateralized group, according to Nelson et al. 21 BIO, bony increased offset. Black bar, glenoidal component. Blue bar, humeral component.
Bias Assessment
The risk of bias of the included studies was assessed using the Methodological Index for Non-Randomized Studies (MINORS) score 27 and the Newcastle-Ottawa Scale (NOS) 29 for nonrandomized studies or the Cochrane risk-of-bias tool for randomized studies. 14 Two independent reviewers (H.-J.L. and S.-H.C.) assessed bias, and the 2 values were averaged as the MINORS score. Disagreement regarding noncontinuous values was resolved through discussion with the senior author (Y.-S.K.).
Statistical Analyses
The data were analyzed using R (version 4.0.3; R Foundation for Statistical Computing) with the “meta” package. Effect sizes based on means were estimated as the standardized mean difference (SMD) using the Hedges g statistic. For binary data, we reported the risk ratio (RR) for effect size. Heterogeneity was identified and quantified as I 2 for each model; I 2 < 25% was considered low heterogeneity. We used a fixed-effects model only for this low-heterogeneity model, and a random-effects model was used otherwise. P < .05 was considered statistically significant.
Results
Literature Search
The initial literature search after removing duplicates resulted in 562 articles. After title and abstract screening, 48 full-text articles were assessed for eligibility. Forty-two articles did not meet the inclusion criteria, leaving 6 articles. 7,12,17,21,24,31 The flowchart of study selection is shown in Figure 2.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram on article selection process.
Study Characteristics and Patient Data
Included were 1 randomized controlled trial 12 and 5 retrospective cohort studies, 7,17,21,24,31 with 594 patients in total (mean age, 72.3 years; range, 69.3-75.4 years). The average follow-up was 37.3 months (range, 12-87.2 months). Four studies performed rTSA for treatment of CTA or osteoarthritis (OA) with rotator cuff insufficiency. 12,21,24,31 Two studies performed rTSA for treatment of CTA, massive cuff tear, or OA, without mentioning the cuff status. 7,17 All studies reported comparability of the preoperative data among groups.
Table 1 summarizes the characteristics of the included studies. All 6 studies used the deltopectoral approach: Three studies 7,12,24 used the Aequalis system (Tornier) for the medialized rTSA, 2 studies 21,31 used the Anatomical Shoulder Reverse System (Zimmer) and Bigliani/Flatow System (Zimmer), and 1 study 17 used the Delta III (DePuy) or Delta Xtend (DePuy). Regarding the lateralized group, the Encore (DJO Global) was the most frequently used prosthesis, 17,21,24,31 followed by 1-cm autologous bone graft for BIO-rTSA with the same prosthesis as the medialized group. 7,12 Five studies 7,12,17,21,31 performed lateralization using glenoid components, and 1 study 24 used both glenoid and humeral lateralization. For the nonrandomized cohort studies, 7,17,21,24,31 the average MINORS score was 17.2 (range, 15.5-18) and the NOS was 7.6 (range, 7-8) (Table 2). The risk-of-bias assessment for the randomized controlled trial 12 is shown in Table 3.
Study and Patient Characteristics a

a BIO-RSA, bony increase offset reverse shoulder arthroplasty; GL, glenoidal lateralization; HL, humeral lateralization; L, lateralized group; Lat, type of lateralization; LoE, level of evidence; M, medialized group; RCS, retrospective cohort study; RCT, randomized controlled trial.
b Data are reported as mean ± SD or mean (range).
MINORS and NOS Scores for Nonrandomized Comparative Studies a
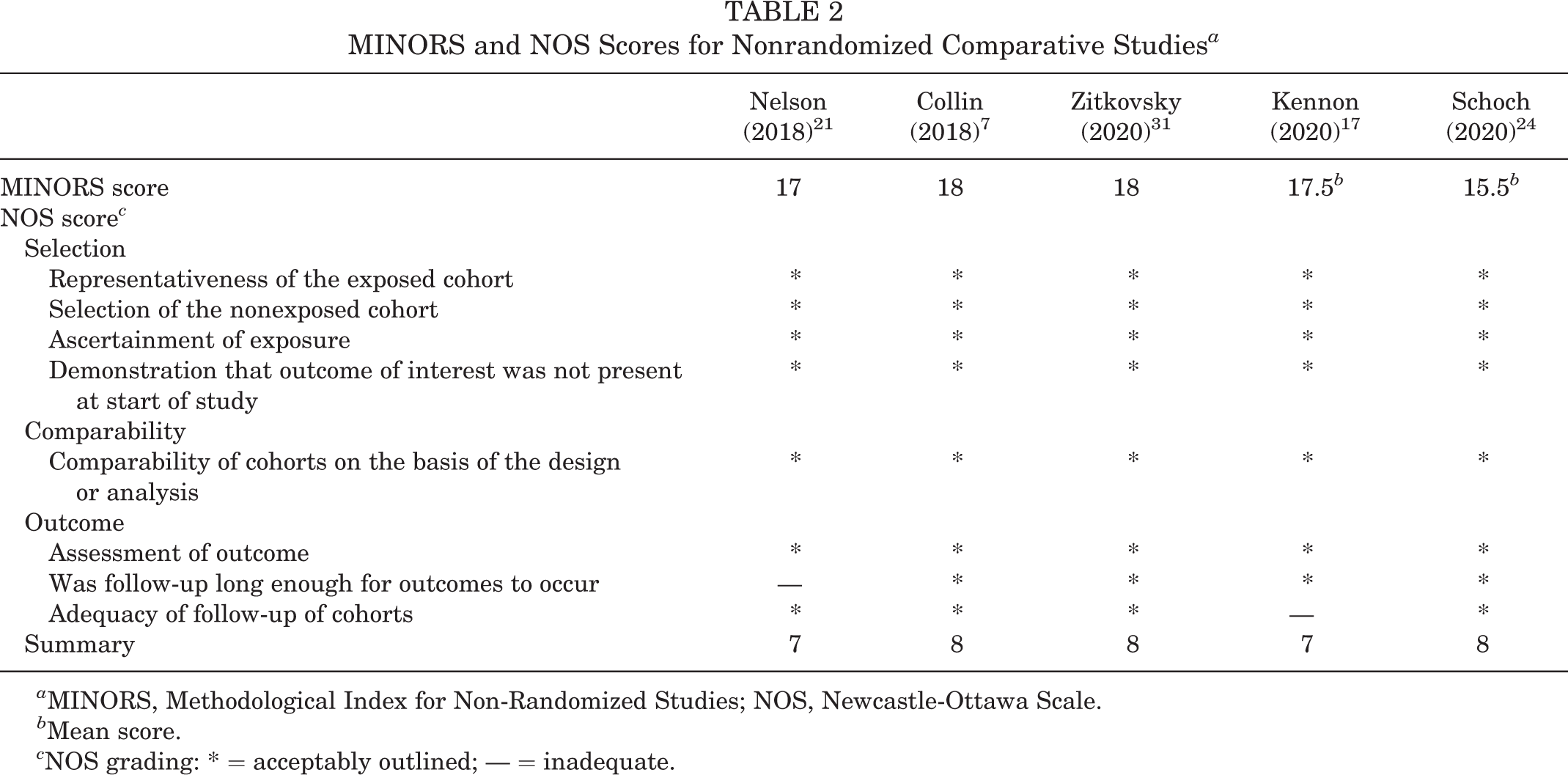
a MINORS, Methodological Index for Non-Randomized Studies; NOS, Newcastle-Ottawa Scale.
b Mean score.
c NOS grading: * = acceptably outlined; — = inadequate.
Cochrane Risk-of-Bias Assessment

Clinical Outcomes
Functional Scores
Of the 6 included studies, 4 studies 17,21,24,31 assessed outcomes using the American Shoulder and Elbow Surgeons (ASES) score and 3 studies 7,12,24 used the Constant score (CSS). Overall, the lateralized group had slightly superior ASES scores and CSS, although the difference was not statistically significant (ASES, P = .310; CSS, P = .077) (Figure 3). Combining the 2 scores also did not result in a significant difference (SMD, 0.28; 95% CI, –0.01 to 0.57; I 2 = 65%; P = .062) (Figure 3).

Forest plots of functional scores. ASES, American Shoulder and Elbow Surgeons score; CSS, Constant score; L, lateralized group; M, medialized group; SMD, standardized mean difference.
Range of Motion
Five studies 7,17,21,24,31 evaluated external rotation (ER) and 4 studies 7,17,21,24 measured forward flexion (FF). The combined results for each ROM did not differ between the 2 groups (ER, P = .238; FF, P = .629) (Figure 4). Greiner et al 12 and Zitkovsky et al 31 evaluated the gain in active ER, which was calculated as the difference between post- and preoperative ER. The combination of results revealed a significant increase in the lateralized group (SMD, 0.71; 95% CI, 0.36-1.07; I 2 = 0%; P < .001) (Figure 5).

Forest plot of ranges of motion. ER, external rotation; FF, forward flexion; L, lateralized group; M, medialized group; SMD, standardized mean difference.

Forest plot of external rotation gain. L, lateralized group; M, medialized group; SMD, standardized mean difference.
VAS Pain Score
Three studies 21,24,31 evaluated VAS pain scores. The integrated value was significantly lower in the lateralized group (SMD, –0.39; 95% CI, –0.65 to –0.14; I 2 = 0%; P = .002) (Figure 6).

Forest plot of VAS pain score. L, lateralized group; M, medialized group; SMD, standardized mean difference; VAS, visual analog scale.
Scapular Notching and Heterotopic Ossification
Five studies 7,17,21,24,31 (539 patients) assessed scapular notching, which was significantly lower in the lateralized group (RR, 0.40; 95% CI, 0.27-0.60; I 2 = 51%; P < .001) (Figure 7). HO was assessed in 3 studies, 7,21,31 and a significant difference favored the lateralized group (RR, 0.52; 95% CI, 0.38-0.71; I 2 = 0%; P < .001) (Figure 8).

Forest plot of scapular notching. L, lateralized group; M, medialized group; RR, risk ratio.

Forest plot of heterotopic ossification. L, lateralized group; M, medialized group; RR, risk ratio.
Complications
Four studies 12,17,21,24 reported complications. The overall RR of complications was lower in the lateralized group, although not significantly (RR, 0.71; P = .339) (Figure 9). Since the complications described in each study were too heterogeneous to analyze individually, the overall complication rate was assessed. Reported complications included acromial stress fracture, intraoperative and postoperative fracture, neurological deficit, wound healing problems, dislocation, dissociation of prosthesis components, and unspecified complications.

Forest plot of the complication rate. L, lateralized group; M, medialized group; RR, risk ratio.
Discussion
Patients who underwent lateralized rTSA had significant improvements in ER gain (SMD, 0.71; P < .001), postoperative pain (SMD, –0.39; P = .002), scapular notching (RR, 0.40; P < .001), and HO (RR, 0.52; P < .001). The functional outcome scores and complication rate did not differ significantly between the 2 groups. While several systematic reviews have examined this, few have performed meta-analyses of various components comparing lateralized and medialized prostheses. 1,11,13,22 Recently published papers with a high level of evidence were combined in this study, and the heterogeneity of the results was relatively low.
One of our interesting findings was that improvement in ER was seen in the lateralized group. Although the ER value at final follow-up did not differ significantly, the ER improvement showed an advantage of lateralized rTSA. Valenti et al 28 reported that a less medialized prosthesis increased ER by 15° to 30°. However, that study was not included in our meta-analysis because it was not a comparative study. Erickson et al 9 systematically reviewed pre- and postoperative ROM after rTSA with 135° and 155° humeral components. While not a meta-analysis, they found that the final ER was significantly higher in the 135° group (135° group, 33.0° vs 155° group, 20.5°), which led to greater ER gains. Only a few studies measured and compared the increase in ER, rather than the final ER, so it was difficult to determine the improvement in ER. Our results are in line with previous studies. Given that rTSA is one of the best possible options for resolving ER restriction, which is a challenging problem, lateralized prostheses can be helpful to increase ER.
The features of lateralized prostheses that help to achieve greater ER are not known. The differences between lateralized and medialized prosthesis might arise from anatomic differences. In our view, scapulothoracic motion, which is differentiated by lateralization, might affect the ER gain. Using electromyography, Pelletier-Roy et al 23 demonstrated that shoulder motion intervention using rTSA was affected by modified scapulothoracic sequencing. They reported that the upper trapezius and latissimus dorsi are the main activator muscles in the rTSA shoulder. Whether glenoid or humeral lateralization was used, both modified the length of the scapular medial border to the glenohumeral joint more than medialized prostheses, which affects the scapulothoracic muscles. Werthel et al 30 measured the amount of offset from the most commonly used implants. Based on their findings, the lateralized prostheses included in our study had a more lateralized offset of 7 to 10 mm compared with the medial group. This difference might be sufficient to alter scapulothoracic motion. Another study 13 suggested that lateralization improves the length-tension relationship of the remaining external rotator cuff muscles. However, no biomechanical papers have examined whether glenoid- or humeral-side lateralization is more beneficial or how much is required. This warrants further study.
Our second major finding was in quantifying the risk of scapular notching and HO as RR. The excellence of a lateralized prosthesis in relation to scapular notching has been reported, but the extent of its superiority varies considerably across studies. 9 –11,24 We determined that the RR of the lateralized prosthesis was 0.40. Similarly, the RR of HO was evaluated. Zitkovsky et al 31 reported the HO of medialized prosthesis as 71.8% compared with 35.3% in the lateral group. This value is considerably different from that of Nelson et al, 21 who reported 35.4% for the medial group compared with 12.2% for the lateral group. All studies reported higher rates of HO for medialized versus lateralized prostheses. After we combined several studies, the RR of HO in the lateralized group was 0.52. Like Friedman et al, 11 we agree with the hypothesis that a change in scapular structure affects scapular notching or HO. Ideally, we would have liked to perform a meta-analysis of radiological measurements of lateralization, such as the acromiohumeral distance, humeral offset from the COR, or scapular neck length, to identify the relevance of more lateralized structure changes and the associated risks. 5 However, there are only a few radiological comparative studies on which to perform a meta-analysis. A future study should compare the radiological results of the 2 groups and assess the clinical outcome relationships.
In our combined results we found a significant difference in VAS pain score. We did not identify specific lateralized prosthesis factors that reduce pain. Some studies 11,20,25 have reported equivocal results regarding the association between scapular notching and worse clinical outcomes. Some studies 11,20 have found no differences in CSS or ROM, while others have reported a significant difference in inferior functional scores that correlates with scapular notching. Further study of the pain source according to rTSA prosthesis design is necessary.
Functional scores and ROM (FF and ER) had a slightly superior SMD in the lateralized group but without statistical significance. Many studies 9,12,21 have reported similar results in that the lateralized group had significantly improved ROM or functional scores, or there was statistical similarity in both groups. However, Kennon et al 17 reported different outcomes, with the medialized group having significantly better FF and ER at final follow-up. Their mean follow-up period was 87.2 months, which was the longest of all studies examined. Therefore, more long-term research is needed. ER gain and pain were significantly better in the lateral group in that study, so future studies should determine whether long-term follow-up reveals a difference in functional scores.
Our study has some limitations. First, the number of studies included in the meta-analysis was small. As we only included studies with an evidence level ≥3, many comparative case-series studies were excluded. Nevertheless, our cohort included 594 patients, which may provide relatively high reliability. Next, the mean follow-up period was relatively short. One included study 17 had a long-term follow-up of 87.2 months, while the mean follow-up of 2 studies 12,21 was shorter than 24 months. More long-term research is needed. Not all of the studies examined here used the same prostheses, so there was heterogeneity in the amount of lateralization. The indications for rTSA differed among studies. Preoperative diagnoses and posterior cuff status could affect the clinical outcomes. However, the 2 groups were similar preoperatively in both studies in terms of ROM, functional scores, strength, and indications for rTSA. It is also possible that some relevant studies that met the inclusion criteria were not included in this research.
Conclusion
Compared with medialized rTSA, VAS pain score, scapular notching, and HO risk were significantly lower in the lateralized rTSA group and the ER increase was greater. Functional scores (ASES and CSS), final ROM (FF and ER), and overall complication rates did not differ between the 2 groups when the findings of the 6 included studies were combined.
Footnotes
Final revision submitted August 29, 2021; accepted September 16, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.