
Abstract
Background:
Several studies have investigated sports participation in patients who undergo total shoulder arthroplasty (TSA). However, there are limited data in the setting of hemiarthroplasty (HA) and reverse total shoulder arthroplasty (rTSA), particularly regarding the frequency of participation in common sports.
Hypothesis:
The majority of patients who undergo TSA or HA will be able to maintain active lifestyles with high levels of sports participation after their procedure, while patients who undergo rTSA will have lower levels of sports participation.
Study Design:
Case series; Level of evidence, 4.
Methods:
We identified patients who underwent TSA, rTSA, stemmed HA, or humeral head resurfacing (the latter 2 were defined collectively as the HA group) by surgeons within our department since January 2004. We excluded patients who (1) underwent revision arthroplasty, (2) had a history of chronic pain syndrome, (3) experienced septic arthritis of the involved shoulder, and/or (4) were deceased at the time of follow-up. The minimum follow-up from the time of surgery was 2 years. Qualified patients were sent a questionnaire that asked about sports participation and the frequency of participation at the time of follow-up. Frequency was rated as 0, 1 to 3, or 4 to 7 times a week. Sports were defined as lower extremity sport, volleyball, tennis, skiing, bowling, swimming, weight lifting, golf, and other sport.
Results:
Overall, 95% of the TSA group, 40% of the rTSA group, and 76% of the HA group who had participated in at least 1 sport before surgery indicated that they were doing so at the time of follow-up. Among active patients in the TSA and HA groups, the most common sports at the time of follow-up were weight lifting (52%), swimming (36%), and golf (25%). For the 2 active patients in the rTSA group, 1 participated in swimming and hunting and fishing, while the other participated in weight lifting. For the active patients in the TSA and HA groups who were participating in at least 1 of the 3 most common sports, most patients indicated that they were doing so 1 to 3 times a week at the time of completing the questionnaire.
Conclusion:
Patients undergoing shoulder arthroplasty can maintain an active lifestyle with moderate to high frequencies of participation after surgery, particularly regarding weight lifting, swimming, and golf.
Keywords
Shoulder arthroplasty has become an increasingly common treatment option for glenohumeral osteoarthritis and rotator cuff arthropathy. Life expectancy continues to increase, and many patients undergoing shoulder arthroplasty are older, recreational athletes who would like to continue sports after surgery and achieve a high quality of life. In addition, shoulder arthroplasty is being performed more frequently in younger patients with glenohumeral osteoarthritis, with studies showing good short-term to midterm outcomes. 3,14 Patients commonly seek guidance regarding returning to a variety of sports after all shoulder arthroplasty procedures, but there is no clear consensus guiding participation, and there remains limited literature on this subject.
A recent study indicated that many surgeons allow a high percentage of patients to return to sports after total shoulder arthroplasty (TSA) or hemiarthroplasty (HA), while fewer surgeons allow return to sports after reverse total shoulder arthroplasty (rTSA). 7 Several studies have investigated sports participation in patients who undergo TSA, 2,4,8,9,11 but there are limited data in the setting of HA 5,9 and rTSA. 6,12 No study has compared all 3 types of arthroplasty procedures. Furthermore, few studies have investigated in detail the frequency of participation in common sports after shoulder arthroplasty 2 as well as sports participation relative to age and duration of follow-up. 4
The aim of this study was to describe participation in all reported sports and the frequency of participation in each sport in patients who have undergone TSA, rTSA, or HA. We hypothesized that the majority of patients who underwent TSA or HA would be able to maintain active lifestyles with high levels of sports participation after their procedure, while patients who underwent rTSA would have lower levels of sports participation.
Methods
Two institutional review board approvals were obtained for this study: 1 for patients undergoing TSA and rTSA and 1 for patients undergoing HA. The methods for both cohorts are similar as described below, and identical inclusion and exclusion criteria were applied to all patient populations. First, a retrospective chart review was performed to identify patients who underwent TSA, rTSA, stemmed HA, or humeral head resurfacing by an orthopaedic surgeon within our department since January 2004. Stemmed HA and humeral head resurfacing were grouped together and defined collectively as the HA group. The indication for performing TSA or HA was glenohumeral osteoarthritis. HA was performed over TSA based on surgeon preference and concern for early glenoid loosening, particularly in patients such as heavy laborers. The indication for performing rTSA was rotator cuff arthropathy. The exclusion criteria were as follows: patients who (1) had undergone revision arthroplasty, (2) had a history of chronic pain syndrome, (3) experienced septic arthritis of the involved shoulder, and/or (4) were deceased at the time of follow-up. The minimum follow-up from the time of surgery was 2 years.
Demographic data were collected and included hand dominance, medical comorbidities, occupation, previous procedures on the same and contralateral shoulders, type of procedure, date of the procedure, and any subsequent procedures on the same shoulder.
Patients who met the inclusion and exclusion criteria were sent a detailed questionnaire that was in part designed by the authors and in part adapted from a study by Bulhoff et al. 2 The first portion of the questionnaire asked about standard demographic data and relevant questions regarding the operative shoulder and subsequent surgery on the same shoulder. The second portion of the questionnaire focused on the Brophy shoulder activity scale and sports participation. 1 Patients were asked to complete this portion of the questionnaire for 2 specific time points: (1) before shoulder arthroplasty and (2) at the time of the questionnaire. Regarding sports participation, the questionnaire asked patients about their participation in several sports and the frequency of participation in each sport; this aspect of the questionnaire was adapted from the study by Bulhoff et al. 2 The frequency of participation was defined as 4 to 7 times a week, 1 to 3 times a week, or never. The types of sports were defined as lower extremity sport, volleyball, tennis, skiing, bowling, swimming, weight lifting, golf, and other sport. The final portion of the questionnaire asked patients to complete the Single Assessment Numeric Evaluation (SANE) score and the American Shoulder and Elbow Surgeons (ASES) score for the affected shoulder.
Statistical analysis was performed using SPSS Statistics (version 25; IBM). Analyses of variance (ANOVAs) with multiple comparisons were used to compare continuous variables among all 3 patient groups. Fisher exact tests were used to compare categorical variables. Statistical significance was set at P ≤ .05.
Results
Demographics
Seventy-six patients in the TSA group, 21 patients in the rTSA group, and 173 patients in the HA group met the inclusion and exclusion criteria. Twenty-seven (35.5%) patients in the TSA group, 7 (33.3%) in the rTSA group, and 75 (43.4%) in the HA group responded to the questionnaire, for a total response rate of 40.3%; the remaining patients were not reachable or were lost to follow-up. Among the patients who underwent TSA, rTSA, or HA and responded to the questionnaire, the mean age at the time of surgery, mean duration of follow-up, sex distribution, and number of patients who underwent surgery on their dominant shoulder are summarized in Table 1. Patients in the HA group were significantly younger than those in the rTSA group (P = .03). The HA group also had a significantly longer duration of follow-up compared with the TSA and rTSA groups (P < .01).
Patient Demographics a

a HA, hemiarthroplasty; rTSA, reverse total shoulder arthroplasty; TSA, total shoulder arthroplasty.
b Statistically significant difference (P = .03).
c Statistically significant difference compared with the TSA and rTSA groups (P < .01).
Sports Participation
Overall, 95% (18/19) of patients in the TSA group, 40% (2/5) of patients in the rTSA group, and 76% (35/46) of patients in the HA group who participated in at least 1 sport before undergoing shoulder arthroplasty indicated that they were doing so at the time of follow-up. One patient in the TSA group and 2 patients in the HA group who did not participate in sports before surgery also indicated that they were participating in sports at the time of follow-up. Therefore, a total of 70% (19/27) in the TSA group and 49% (37/75) in the HA group indicated active participation in sports at the time of follow-up. Of these active patients, 37% (7/19) in the TSA group, 50% (1/2) in the rTSA group, and 51% (19/37) in the HA group indicated that they were participating in ≥2 sports at the time of follow-up. Among active patients in the TSA and HA groups, the most common sports that they participated in at the time of follow-up were weight lifting, swimming, and golf (Table 2 and Figure 1). For the 2 active patients in the rTSA group, 1 patient participated in swimming and hunting and fishing, and the other patient participated in weight lifting.
Participation in Sports at the Time of Follow-up for Each Type of Shoulder Arthroplasty Procedure a

a Data are shown as n (%). HA, hemiarthroplasty; rTSA, reverse total shoulder arthroplasty; TSA, total shoulder arthroplasty.
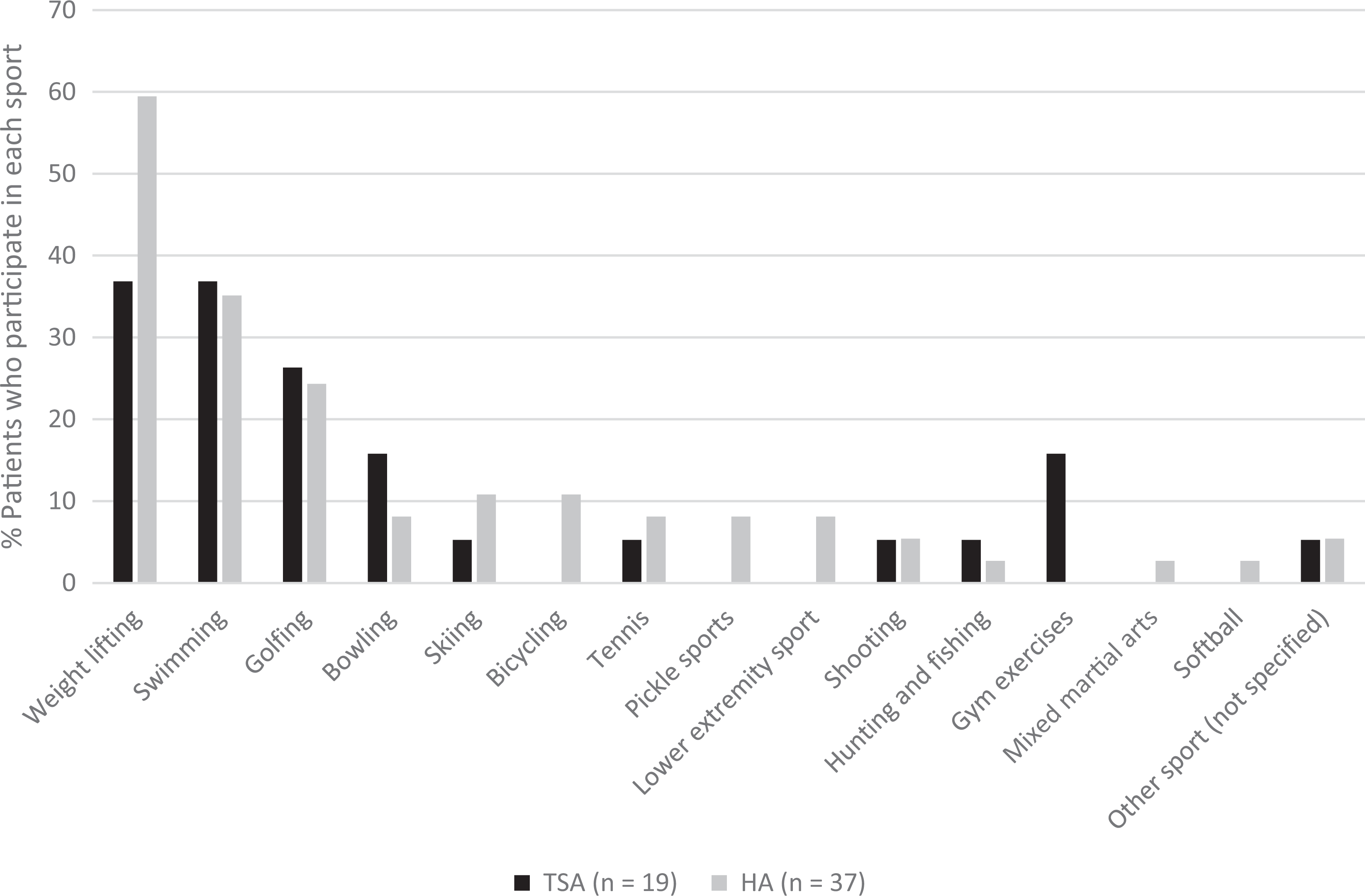
Comparison of participation in sports at the time of follow-up for patients undergoing total shoulder arthroplasty (TSA) or hemiarthroplasty (HA).
For patients in the TSA and HA groups who were participating in at least 1 of the 3 most common sports (weight lifting, swimming, and golf) at the time of follow-up, most patients indicated that they were participating 1 to 3 times a week at the time of completing the questionnaire (Figure 2). The 1 patient in the rTSA group who participated in swimming and hunting and fishing did so at a frequency of 1 to 3 times a week for both sports. The other patient in the rTSA group who participated in weight lifting did so at a frequency of 4 to 7 times a week.

Comparison of frequency of participation in the 3 most common sports for patients undergoing total shoulder arthroplasty (TSA) or hemiarthroplasty (HA).
All patients who responded to the questionnaire were further subgrouped by age at the time of follow-up and duration of follow-up (Table 3). For patients in the HA group, there was a significant difference among different age groups regarding participation in sports at the time of follow-up (P = .001). When directly comparing patients in the TSA and HA groups aged >70 years, a significantly higher percentage of those in the TSA group participated in sports at the time of follow-up (P = .018). For both the TSA and HA groups, there was no significant difference among different durations of follow-up regarding participation in sports at the time of follow-up.
Participation in Sports at the Time of Follow-up by Age at Follow-up and Duration of Follow-up a
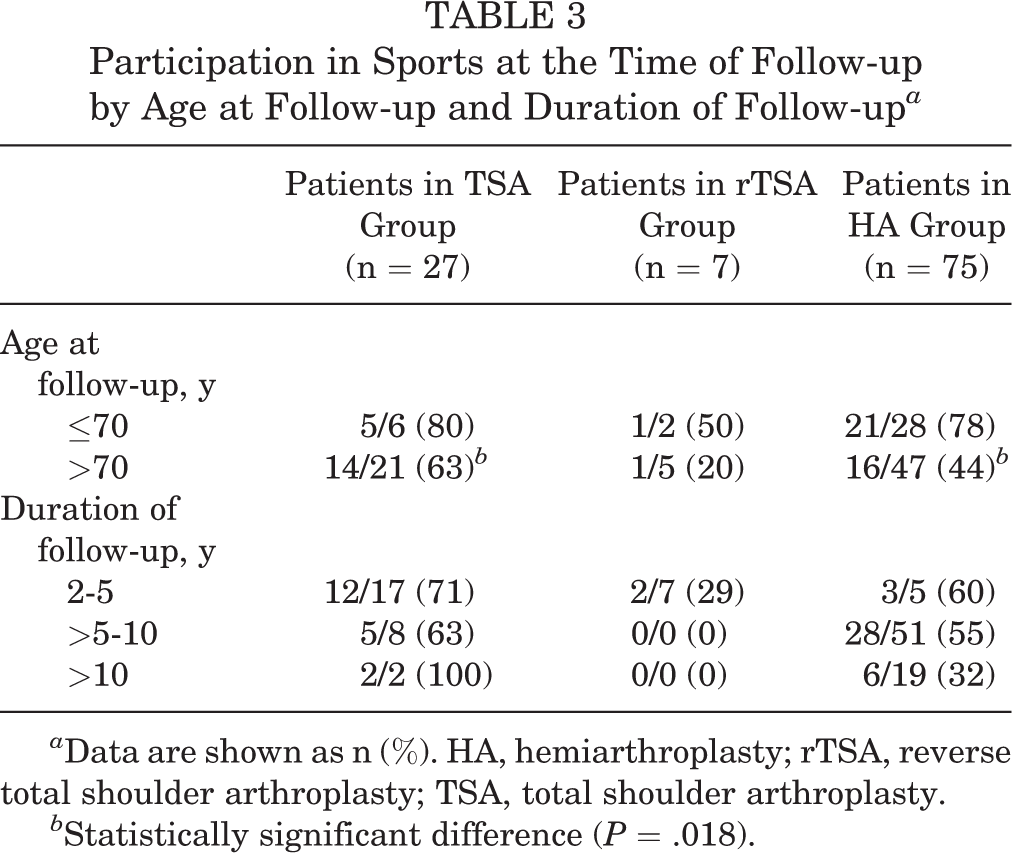
a Data are shown as n (%). HA, hemiarthroplasty; rTSA, reverse total shoulder arthroplasty; TSA, total shoulder arthroplasty.
b Statistically significant difference (P = .018).
Patient-Reported Outcomes
The mean postoperative ASES and SANE scores for all patients who responded to the questionnaire are displayed in Table 4. The mean ASES score was significantly higher (better) in the TSA group than in the HA group (P < .001, ANOVA with Tukey post hoc comparison). This was not observed between the TSA and rTSA groups (P = .805) or between the rTSA and HA groups (P = .395). The mean ASES score in patients in the TSA group who participated in at least 1 sport at the time of follow-up was significantly higher than in patients who did not participate in any sport at the time of follow-up (85.8 vs 62.9, respectively; P = .002). This was not observed in the HA group (56.9 vs 53.0, respectively; P = .487). There was no statistically significant difference in the SANE score among the different groups of patients (P = .417, ANOVA).
ASES and SANE Scores a

a Data are shown as mean ± SD (range). ASES, American Shoulder and Elbow Surgeons; HA, hemiarthroplasty; rTSA, reverse total shoulder arthroplasty; SANE, Single Assessment Numeric Evaluation; TSA, total shoulder arthroplasty.
b Statistically significant difference (P < .001).
Discussion
In our study, 95% of the TSA group, 40% of the rTSA group, and 76% of the HA group who had participated in at least 1 sport before undergoing their respective shoulder arthroplasty procedure indicated that they were participating in at least 1 sport at the time of follow-up. The most common sports among patients in the TSA and HA groups were weight lifting, swimming, and golf. For these sports, the majority in the TSA and HA groups were participating 1 to 3 times a week. Patients in the rTSA group were less likely to participate in sports, although the small sample size should be taken into consideration.
Our patients’ overall rate of sports participation with respect to TSA is comparable with those in similar studies. These studies have reported 57% to 97% rates of return to sports in patients undergoing TSA who participated in sports before and after surgery. 2,4,11 With respect to HA, similar studies have reported 66% to 81% rates of return to sports in patients who participated in sports before and after surgery. 4,5,9 The rate of return to sports for rTSA has not been studied in detail, with only 1 recent study reporting an 85% rate of return to sports in patients who participated in sports before and after surgery. 6 Our rate of return to sports after rTSA was much lower than this reported rate; however, the smaller sample size may limit an overall conclusion.
Interestingly, our rates of return to sports for TSA, rTSA, and HA are comparable with those in a recent study 7 investigating surgeon preferences regarding sports participation after various types of arthroplasty procedures. That study found that 76.5% of surgeons allowed patients undergoing TSA to return to all sports, whereas 87.2% and 92.0% of surgeons allowed patients undergoing HA and humeral head resurfacing to return, respectively, while only 45.2% of surgeons allowed return to sports for patients undergoing rTSA. Our results are also consistent with a recent study demonstrating a significantly higher rate of return to sports for TSA versus HA. 4
Our study was also able to elucidate the most common sports played by patients after their procedure. While swimming and golf have been reported as common sports after TSA and HA, 2,6,9,11 weight lifting, which was our most common sport for all arthroplasty procedures, has not been described previously. Moreover, while a majority of patients participated with a moderate frequency of 1 to 3 times a week, several patients reported a moderate to high frequency of 4 to 7 times a week, indicating a relatively high activity level and active lifestyle after shoulder arthroplasty.
To our knowledge, only 1 study has investigated participation in sports after shoulder arthroplasty by age group, 4 and none has investigated trends in return to sports depending on the time of follow-up. In our study, a significantly higher percentage of patients in the TSA group aged >70 years were participating in sports when compared with those in the HA group. Fewer patients in the HA group were participating in sports as the duration of follow-up increased, particularly after 10 years. This may be consistent with either the natural history of HA and increased likelihood of progressive glenoid wear or generalized decreased activity levels with aging. Additional data and larger numbers are required to better compare sports participation after TSA versus HA.
Regarding patient-reported outcomes, the TSA group had a significantly higher mean ASES score than the HA group. These findings are similar to those reported in other studies comparing TSA and HA. 4,13 These results suggest that even though high percentages of both the TSA and HA groups eventually return to sports after undergoing shoulder arthroplasty, patients in the TSA group may be able to participate in their sports with improved pain and functional outcomes. While the mean SANE score for the TSA group was higher (better) than that of the HA group, this did not reach statistical significance as it did in other studies. 4,10
Regarding rTSA, while our sample size was limited, we found that the rate of sports participation was lower, which was consistent with our hypothesis, and also lower than the reported rate in the literature. 6 For those who did participate in sports, however, the type of sports and frequency were similar to those of TSA and HA. While a prior study reported a hesitation of surgeons to allow sports after rTSA, 7 our study indicates that patients may be advised that some level of sports participation is possible. It is possible that the lower rate of sports participation in the rTSA group when compared with the TSA and HA groups is because of the higher mean age at the time of surgery and lower preoperative baseline activity.
The major limitation of this study is the retrospective nature of part of the questionnaire, resulting in recall and selection biases. Patients may have had difficulty recalling their previous level of participation in sports. There was a limited response rate, as only 35.5% of those in the TSA group, 33.3% in the rTSA group, and 43.4% in the HA group responded to our survey. A large portion of patients were lost to follow-up and could not be reached. While it is feasible that patients who did not complete the questionnaire were not involved with sports and may have felt less inclined to participate in the study, it is not possible to know. Given the overall response rate of only 40.3%, sampling bias is another significant limitation, particularly regarding the type of sport and frequency of participation. Stemmed HA and humeral head resurfacing were grouped together into a collective HA group, but future studies with larger patient samples may be able to evaluate these 2 groups separately. In addition, this was purely a descriptive study, without correlation with objective data including range of motion and radiographic data. Given the small sample size for the rTSA group, only limited conclusions could be drawn. Future studies that are prospective in nature, have larger numbers of patients, and have a more detailed follow-up, including radiographic data, may help address both recall bias and limited sample sizes. These studies may shed light on whether some sports are more acceptable than others regarding revision and implant survivorship rates.
Conclusion
Among patients who undergo TSA or HA who participated in sports before shoulder arthroplasty, a high percentage can expect to participate in sports after surgery. Sports participation is also a reasonable expectation after rTSA but may be influenced by surgeon-specific preferences regarding postoperative restrictions. Our study suggests that patients can maintain an active lifestyle with moderate to high frequencies of participation after surgery, particularly regarding weight lifting, swimming, and golf. These results may be helpful for preoperative counseling and setting of expectations, particularly for patients interested in continuing sports after shoulder arthroplasty.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Intramural Ferguson Grant from the University of Pittsburgh Medical Center. A.L. is a consultant for Arthrex and has received educational support from Mid-Atlantic Surgical Systems. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Pittsburgh Institutional Review Board.