
Abstract
Background:
Sex-based biomechanical differences during a drop vertical jump (DVJ) may explain the increased risk of anterior cruciate ligament injury in females. Video motion capture using artificial intelligence (VMocap) is a new method for accurate motion analysis.
Purpose:
To use VMocap to identify sex-based differences in biomechanics during a DVJ in Asian athletes.
Study Design:
Controlled laboratory study.
Methods:
A total of 63 female and 61 male Asian soccer players volunteered for this study in 2018. Participants performed a bilateral DVJ using VMocap, and the knee valgus angle (KVA), knee flexion angle (KFA), hip flexion angle (HFA), and lower leg anterior inclination angle (LAIA) were calculated from the motion capture data. These joint angles and inclination angles were evaluated at the time of highest point of the first jump (H1), initial contact (IC), maximum knee flexion (MKF), toe-off (TO), and highest point of the second jump (H2). The unpaired t test was used to compare sex-based differences.
Results:
At H1, the KVA in females showed more valgus (−2.9° vs −5.4°) and the LAIA in females was greater (29.1° vs 25.7°) versus males (P < .01 for both). At IC, the KVA in females showed more valgus (−1.3° vs −3.0°) and females had a greater KFA (20.8° vs 14.3°) and LAIA (5.1° vs 0.0°) compared with males (P < .01 for all). At MKF, female KVA showed more valgus (6.2° vs −9.5°), and females had greater LAIA (36.6° vs 34.6°), smaller KFA (77.5° vs 87.5°), and smaller HFA (55.8° vs 82.0°) compared with males (P < .01 for all). At TO, female KVA showed more valgus (−0.7° vs −3.1°) and female KFA, HFA, and LAIA were greater (31.7° vs 19.2°; 19.9° vs 16.4°; and 18.2° vs 11.5°, respectively) than males (P < .01 for all). At H2, females had a greater KFA (18.6° vs 14.6°) and LAIA (13.3° vs 9.9°) than males (P < .04 for both).
Conclusion:
Asian female soccer players showed increased KVA and LAIA, decreased KFA and HFA at MKF, and increased KFA at IC and TO compared with their male counterparts in this analysis of the DVJ.
Clinical Relevance:
Elucidation of kinematic differences between the sexes can aid in predicting injuries.
Anterior cruciate ligament (ACL) injury is increasing among young athletes. Frequently, ACL injury requires ligament reconstruction, where prolonged rehabilitation delays athletes’ returning to sport. 17 Female athletes have a higher incidence of noncontact ACL injuries than male athletes in the same sports. 25 In addition, they have a higher risk of incurring a subsequent ACL injury after primary ACL reconstruction. 2,24 Surprisingly, female sex has been reported as a primary risk factor for ACL injury, with an incidence 4 to 6 times higher compared with males. 12,28 Intrinsic neurocognitive, neuromuscular, and biomechanical risk factors for noncontact ACL injury in female athletes have been detailed previously. 12,22,29,32 In the context of ACL injury prevention, it is crucial to recognize sex differences in kinematics.
Hewett et al 12 first suggested that the drop vertical jump (DVJ) test could be used to screen for ACL injury risk. DVJ is used commonly as an evaluation tool that simulates the mechanism of landing and propulsion during athletic participation. 7,13 This task has been helpful in assessing patients with pathologic knee conditions, including after ACL injury and reconstruction. 30 Hewett et al 12 revealed that greater knee abduction angles and moments and shorter stance times in DVJ are the predictors of ACL injury risk in females. However, this finding was not replicated in another study, 18 possibly because of the multifactorial nature of ACL injury.
Some studies have reported sex-based differences in the DVJ or similar landing tasks, ¶ with differences existing in knee flexion, 5 knee valgus, 11,16 and normalized vertical ground-reaction force. 16 However, these reports have had limitations, such as relatively small sample sizes, 4,15,16,20,23 2-dimensional (2-D) motion analysis, 14,15 and studies based on only White athletes. # In particular, there are few studies regarding DVJ in Asian athletes.
Laboratory-based measures, such as 3-dimensional (3-D) motion capture, have been used to identify the movement patterns associated with ACL injury risk. 21 However, it is challenging to use these assessments in clinical settings due to equipment costs, extended time for data collection and processing, and the technical skills needed to operate the system. The passive optical motion capture method, which imposes the least constraint on participants, still requires approximately 40 spherical reactive markers to be attached to the body. To overcome this limitation, an image-based motion capture system that imposes no constraint on human patients needs to be developed. Video motion capture using artificial intelligence (VMocap) was created as an image-based 3-D human motion reconstruction with spatiotemporal accuracy and smoothness closer to passive optimal motion capture. 19 Unlike previous motion-capture methods, the placement of reflecting markers is unnecessary; hence, VMocap makes it possible to consecutively record data for a large number of human patients in a short time.
The purpose of this study was to assess sex-based differences during the DVJ in a large, athletic, Asian population using the VMocap system. Our hypothesis was that there would be sex-based differences in Asian soccer players during DVJ.
Methods
Study Design and Participants
A total of 124 high school and college soccer players (63 college and high school female soccer players and 61 college male soccer players) were included in this study in 2018. This study was conducted as a part of a sports injury prevention project, the “Prospective Study of Predictors of Sports Injuries: UTokyo Sports Science Initiative.” The study protocol was approved by the ethics committee of our institute; the purpose and potential risks of the study were explained to the participants, and written informed consent was obtained from all participants and/or their parents or guardians. The inclusion criteria for the participants were soccer players who participated in a preseason medical assessment. None of the players were injured at the preseason medical assessment, and none reported any lower limb musculoskeletal injury in the 3 months leading up to the study. Participant demographics are shown in Table 1.
Participant Demographics a
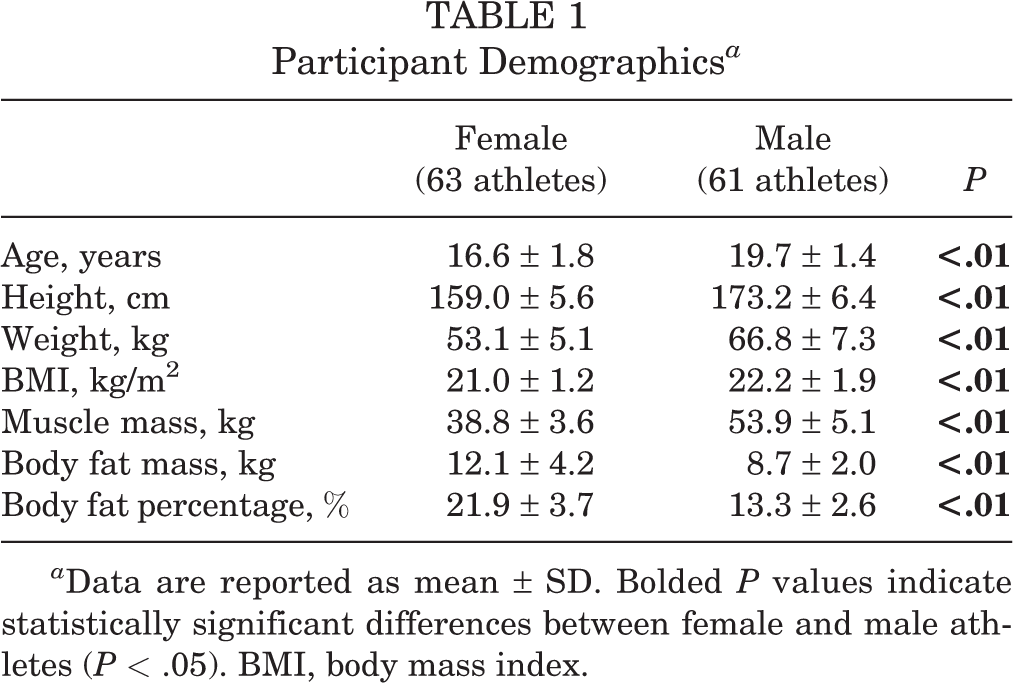
a Data are reported as mean ± SD. Bolded P values indicate statistically significant differences between female and male athletes (P < .05). BMI, body mass index.
Video Motion Capture Using Artificial Intelligence
The operating methods and accuracy of VMocap have been validated previously. 19 VMocap can be described as an iterative update of a human skeletal model’s joint angles based on the multicamera images that surround a patient. The skeletal model is treated as a virtual open tree-structure kinematic chain. From the red-green-blue (RGB) images captured from the multicamera system (image data were captured in 120 frames per second from 4 RGB cameras (acA1920-155uc, Basler), a person’s key joint points can be detected using the convolutional neural network of the OpenPose free software, as in the form of confidence maps for body part detection on a 2-D image. 3,31 There were 18 key points, consisting of joint positions at the shoulders, elbows, wrists, hips, knees, ankles, and neck, along with other features such as the eyes, ears, and nose. The virtual markers of probable joint positions are generated from these body part confidence maps of the key points. Next, inverse kinematics computation was solved so as to minimize the error between the virtual markers’ position and skeletal model’s joint position. These proposed methods enabled us to analyze the patients’ motions and identified the joint angles through motions (Figure 1). In addition, its accuracy was validated in comparison with conventional 3-D motion capture. 19

Video motion capture using artificial intelligence (VMocap) during a drop vertical jump. (A) Image data were captured at 120 frames/s from 4 red-green-blue cameras. (B) Joint positions were identified in each image by using convolutional neural networks. (C) Joint position and angle were estimated by solving inverse kinematics from a skeletal model.
Drop Vertical Jump
We instructed participants to DVJ according to methods described in previous studies. 6,8,12,14,18,27 Before testing, the instructions for DVJ were explained verbally to each participant and then demonstrated by instructors. The participants were instructed to stand on the top of a 30-cm box with their feet shoulder-width apart and their hands free, drop off the box to complete a first landing (first jump), and then immediately perform a maximal-effort vertical bilateral jump followed by a second landing (second jump). At each testing session, participants completed 3 to 5 practice trials until they felt comfortable with the technique. After completing the practice trials, participants were provided with sufficient break time before testing to prevent fatigue. Participants performed bilateral DVJ only once because they had to perform lateral jumps and cutting maneuvers immediately afterward.
Biomechanical Data Analysis
Frontal and sagittal planes were based on the plane defined by 3 points (midpoint of bilateral shoulders and bilateral hip center points). In the frontal and sagittal planes, the joint angles and inclinations were calculated for the ankle, knee, hip, and chest point using motion capture data. Knee valgus angle (KVA) was calculated in the frontal plane, and knee flexion angle (KFA), hip flexion angle (HFA), and lower leg anterior inclination angle (LAIA) were calculated in the sagittal plane (Figure 2). These joint angles and inclination angles were evaluated at the time of highest point of the first jump (H1), initial contact (IC), maximum knee flexion (MKF), toe-off (TO), and highest point of the second jump (H2). The IC and TO events were determined as the times at which ankle acceleration became zero (ie, the ankle was set on the ground) or left zero (ie, the ankle left the ground). The H1 and H2 events were determined as the time that midair hip acceleration became zero during the first jump (H1) and second jump (H2).

Biomechanical data analysis for the drop vertical jump. (A) Knee valgus angle in the coronal plane. (B) Hip flexion angle, knee flexion angle, and lower-leg anterior inclination angle in the sagittal plane.
Statistical Analysis
An unpaired t test was used in the comparison analysis between female and male athletes. All significance tests were 2-tailed, and a significance level of P < .05 was used for all tests. A post hoc power analysis showed that KVA, KFA, and HFA at MKF had over 90% power (0.96-0.99) with a 2-sided significance level set at .05. All statistical analyses were performed using SPSS Version 25.0 (IBM).
Results
Sex-based differences in the DVJ at each discrete time point are summarized in Table 2. At H1, KVA (knee coronal plane angle) in female showed significantly more valgus than in male (female, −2.9º; male, −5.4º; P < .01), and LAIA was significantly greater than in male (P < .01). At IC, KVA in female showed significantly more valgus than in male (female, −1.3º; male, −3.0º; P = .01), KFA and LAIA in female were significantly greater than in male (both P < .01) (Figure 3A). At MKF, KVA in female showed significantly more valgus than in male (female, 6.2º; male, −9.5º; P < .01), and LAIA in female was significantly greater than in male (P < .01) (Figure 3B). In addition, KFA and HFA in female were significantly smaller than in male (P < .01 for both). At TO, KVA in female showed significantly more valgus than in male (female, −0.7º; male, −3.1º; P < .01), and KFA, HFA and LAIA in female were greater than in male (P < .01, P = .04, P < .01, respectively) (Figure 3C). At H2, only LAIA in female was greater than in male (P = .04).
Sex-Based Differences During Drop Vertical Jump a

a Data reported in degrees as mean ± SD. Bolded P values indicate statistically significant difference between females and males (P < .05). IC, initial contact; MKF, maximum knee flexion; TO, toe-off.
b H1, highest point of the first jump; H2, highest point of the second jump.

Sex-based differences during the drop vertical jump. Shown are male and female postures at (A) initial contact, (B) maximum knee flexion, and (C) toe-off.
Discussion
The most important findings in this study were that VMocap could reveal significant sex-based differences in KVA, KFA, HFA, and LAIA in DVJ at all typical discrete time points in young Asian soccer players. Specifically, the female knee showed more valgus angle at almost discrete time points, the female KFA was greater at IC and TO and smaller at MKF, and the female HFA was smaller at MKF and greater at TO. Our results could provide answers to the previously unsolved sex-based differences in DVJ such as knee angles and hip angles among young Asian soccer players.
Regarding the valgus angle difference between females and males, the KVA in females was significantly greater than that in males at H1, IC, MKF, and TO (other than H2) in this study, and the differences were approximately 2.5º, 1.7º, 15.7º, and 2.4º at H1, IC, MKF, and TO, respectively. Similarly, Ford et al 8 reported that the female valgus angle was significantly greater at IC and MKF, and, in addition, the female valgus angle was greater during the whole DVJ in 81 high school basketball players. Hewett et al 11 also revealed that the female valgus angle was greater at IC and MKF in the DJV of 88 adolescent athletes. Holden et al 14 found greater dynamic KVA in adolescent females during a landing exercise, and a subsequent 2-year tracking study revealed that this sex difference remained for 2 years. They mentioned that the dynamic valgus angle came from a combination of hip adduction, internal rotation, and external tibial rotation. Our results using VMocap were consistent with previous studies on the sex differences in KVA. 1,8,11,14,23 In addition, the total number of participants in the present study was 124, and this was therefore a relatively large study.
In addition, Ford et al 8 mentioned that the greater female valgus angle could be related to poor muscular control of the lower extremity in the coronal plane in female athletes. This likely reflects changes in the contraction patterns of the knee adductors and abductors, primary the knee flexors, hamstrings, and gastrocnemius, which possess tendons that cross both the medial and lateral sides of the joint. As a result of decreased neuromuscular control, greater KVA may cause female athletes to exhibit decreased joint control in the coronal planes, predisposing them to increased risk of ACL injury. 8 In this point of view, the sex-based difference in KVA must be focused on, and landing training to decrease valgus angle could be particularly effective for female athletes. 10 However, in this study, neither postural stability nor muscular control was evaluated; therefore, we are investigating the relationship between the KVA and postural control or muscular control prospectively.
Regarding the KFA difference between female and male athletes, the female KFA was greater at IC and TO and smaller at MKF in this study. This result indicated that total female knee range of motion was significantly lesser than that of males during DVJ. However, Holden et al 14 revealed that the female KFA at the frame immediately prior to IC was smaller than the male KFA and that the female peak KFA was smaller than the male KFA in adolescent athletes in DVJ. Decker et al 4 reported that female KFA was smaller at IC, and female knee range of motion was greater during a drop jump, of 21 recreational athletes and suggested that the female erect landing posture could present a risk of ACL injury. In addition, they showed both male and female athletes demonstrated similar landing phase time but the female knee flexed deeply, thereby indicating that females could attempt to dissipate the large external force over a wider range of knee joint motion. 4 Huston et al 15 found that female KFA was smaller at IC and there was no difference at MKF in 20 athletes who performed some activity grades in the bilateral drop test.
On the contrary, several studies have reported no sex difference in the KFA at IC and MKF in a landing task. 10,16,21 Therefore, no clear consensus from previous studies exists regarding the sex difference in KFA. In our study, unlike the previous reports, female knee flexion was greater than male knee flexion at IC. One of the reasons why female knee flexion at IC was greater may be because female soccer players in this study were willing to participate in this sports injury prevention study; therefore, they might have been trained in variable fundamental motions including landing tasks. However, the whole range of knee flexion at DVJ was significantly lower. In other words, females could have stiffer landing without sufficient force absorption, and this could induce sports injuries such as ACL injury and ankle sprains.
In this study, the HFA in females was smaller at MKF and greater at TO that it was in males. However, previous studies demonstrated that HFA in the bilateral drop landing task did not reveal any sex differences in the athletes. 4,16,20 Recently, Koga et al 17 revealed the importance of hip kinematics on noncontact ACL injury at IC using video analysis. However, many studies on the kinematics in landing or DVJ did not evaluate their HFAs. From this point of view, this study is meaningful because we discovered the female lower hip flexion at MKF. HFA is supposed to be crucial for sports injury prevention, as the HFA is related closely to the position of the center of gravity and absorption of vertical ground force. 20 In addition, we also demonstrated sex differences in the LAIA. Considering the kinematics in DVJ, we should put an emphasis on the whole-body posture and not focus on only a specific joint. The future direction of our research will focus on the relationship between sex differences in DVJ and sex differences in sports injury. Therefore, we are prospectively investigating sports injuries in participating athletes.
In this study, there were many sex-based differences in posture during the DVJ, not only at IC and MKF but also at TO, H1, and H2. In DVJ, many studies evaluated the posture only at IC. 4,8,11,14,15,16,20,21 because the posture at IC was supposed to be related to ACL injury risk. Recently, Koga et al 17 investigated ACL injury situations using video analysis with model-based matching and revealed that ACL injury occurred within 40 milliseconds of IC. Therefore, it was proven that the posture at IC as well as the H1 posture were critical for the prevention of ACL injury because the H1 posture could be related to ACL injury regarding feedforward control. In addition, some studies have investigated the posture at maximum knee angle, 8,14,15,16,21 because maximum knee angle may be related to stiff landing, which generates amplified vertical ground force, and total KFAs during landing have been identified as intrinsic risk factors for knee injury through prospective studies. 22 However, there seem to be few studies regarding the posture of TO because TO exists only in DVJ and not in the drop landing task. However, the posture at TO could be influenced by balance ability during the landing phase and the ability to dissipate vertical force, because all motions during DVJ were performed in succession within a short time period and were interrelated. Therefore, we should focus on sex differences in posture at TO, and we are now investigating prospectively its relationship with sports injury.
There are limitations to the present study. First, there was an age difference between female and male participants. However, physical maturity is reached earlier in girls than in boys. Our female athletes were 15 to 23 years old; therefore, their physical growth was complete. In addition, Holden et al 14 revealed that there was no effect of maturation on DJV after the age of 14 years in female athletes. Second, we could not evaluate the ankle angle and hip coronal angle; hence, we evaluated the lower leg anterior inclination. The technical limitation is that the VMocap system could not recognize the direction and rotation of the foot. The recently upgraded AI VMocap can recognize an ankle and measure its angle. Therefore, we will investigate ankle kinematics in DJV in a future study. In addition, we could not evaluate the hip rotation angle; Koga et al 17 mentioned that hip rotation angle and not only hip flexion might contribute to ACL injury. For that reason, we will study hip rotation in DVJ by revising VMocap in the future. Third, the fact that we included only soccer players in our study limits the generalizability of these research findings. However, we are now prospectively assessing DVJ in other sports players as well as other motions, such as the cutting maneuver, and we will reveal the results in the future. Fourth, the results of the present study are applicable to athletes willing to participate in a sports-injury prevention study; therefore, the results should be confirmed in a larger cohort.
Conclusion
Asian female soccer players showed increased KVA and LAIA during DVJ and showed decreased KFA, HFA at MKF and increased KFA at IC and TO. VMocap revealed that there were significant sex differences in DVJ at all discrete time points in Asian soccer players.
Footnotes
Notes
Acknowledgment
The authors gratefully acknowledge the cooperation of the physicians, physical therapists, and athletic trainers as volunteer staff during our prospective study of predictors for sports injuries.
Final revision submitted May 1, 2021; accepted July 14, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding. This study was funded by scholarships from the East Japan Railway Company and Shimamura-Syoukai and grants from the Nakatomi Foundation, the Japanese Orthopaedic Society of Knee, Arthroscopy and Sports Medicine, the Japanese Sports Medicine Foundation, the Japan Sport Council, the Watanabe Memorial Foundation for the Advancement of Technology, and the Japan Orthopaedics Traumatology Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Graduate School of Medicine and Faculty of Medicine, The University of Tokyo (reference No. 11907-2).