
Abstract
Background:
Knee kinematic parameters during a drop vertical jump (DVJ) have been demonstrated to be associated with increased risk of noncontact anterior cruciate ligament (ACL) injury. However, standard motion analysis systems are not practical for routine screening. Affordable and practical motion sensor alternatives exist but require further validation in the context of ACL injury risk assessment.
Purpose/Hypothesis:
To prospectively study DVJ parameters as predictors of noncontact ACL injury in collegiate athletes using an affordable motion capture system (Kinect; Microsoft). We hypothesized that athletes who sustained noncontact ACL injury would have larger initial and peak contact coronal abduction angles and smaller peak flexion angles at the knee during a DVJ.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
102 participants were prospectively recruited from a collegiate varsity sports program. A total of 101 of the 102 athletes (99%) were followed for an entire season for noncontact ACL injury. Each athlete performed 3 DVJs, and the data were recorded using the motion capture system. Initial coronal, peak coronal, and peak sagittal angles of the knee were identified by our software.
Results:
Five of the 101 athletes sustained a noncontact ACL injury. Peak coronal angles were significantly greater and peak sagittal flexion angles were significantly smaller in ACL-injured athletes (P = .049, P = .049, respectively). Receiver operating characteristic (ROC) analysis demonstrated an area under the curve of 0.88, 0.92, and 0.90 for initial coronal, peak coronal, and peak sagittal angle, respectively. An initial coronal angle cutoff of 2.96° demonstrated 80% sensitivity and 72% specificity, a peak coronal angle cutoff of 6.16° demonstrated 80% sensitivity and 72% specificity, and a peak sagittal flexion cutoff of 93.82° demonstrated 80% sensitivity and 74% specificity on the study cohort.
Conclusion:
Increased peak coronal angle and decreased peak sagittal angle during a DVJ were significantly associated with increased risk for noncontact ACL injury. Based on ROC analysis, initial coronal angle showed good prognostic ability, whereas peak coronal angle and peak sagittal flexion provided excellent prognostic ability. Affordable motion capture systems show promise as cost-effective and practical options for large-scale ACL injury risk screening.
Sport-related injuries are common, and it has been reported that up to 18% of athletes stop participating in sports as a result of such injuries. 5 Regarding sport-specific injuries, higher rates are observed among individuals participating in “cutting” sports such as basketball, soccer, and football.1,2 It is not surprising, therefore, that 44% of these injuries involve the knee, of which close to 80% are attributed to noncontact anterior cruciate ligament (ACL) tears.14,15
In response to the significant incidence of sport-related injuries, numerous training programs have been developed and implemented as preventive measures to reduce injury occurrence. 3 One such initiative is the FIFA11+ injury prevention program, focusing on quadriceps, hamstring, and core activation exercises to decrease the strain on the ACL during sports participation. 3 Successful injury prevention programs have been demonstrated to decrease the incidence of ACL injury, thereby highlighting the importance of identifying at-risk athletes and effectively decreasing their risk of sport-related injury with early targeted interventions.20,23
Certain parameters associated with neuromuscular control of the knee have displayed promise for use in ACL injury risk screening. In their landmark study, Hewett et al 10 found that increased coronal abduction angle and decreased peak sagittal flexion angle during a drop vertical jump (DVJ) were associated with increased risk for ACL injury. Although these results provided valuable information, assessment of athletes via traditional 3-dimensional motion tracking systems with multiple sensors is impractical and not cost-effective for routine screening. Alternative motion capture systems that are simple to use and cost-effective without compromising measurement accuracy are required to support widespread screening programs. In our laboratory, an affordable motion capture system (Kinect; Microsoft) has been shown to produce intraclass correlation coefficient values ranging from 0.771 to 0.917 for assessing DVJ parameters when compared with the current gold standard Vicon system (Karatzas et al, unpublished data, 2022). For reference, values >0.75 have been demonstrated to indicate excellent interrater reliability for kinematic assessment. 9 These findings warrant further research on kinematic knee angles as measured by practical and affordable motion capture systems.
The poor natural history of the ACL-injured knee, where many athletes do not achieve preinjury playing capacity after ACL reconstruction, and the failure of current surgical techniques to overcome long-term deterioration suggest that research should be directed at ACL injury risk screening and prevention.3,4,6,27 Thus, the goal of our study was to develop and test a novel and easy-to-use method for players, coaches, and supporting staff to assess knee kinematics using an affordable motion capture system and to identify the association between such knee kinematics and noncontact ACL injury. We hypothesized that athletes who sustained noncontact ACL injury would have significantly larger initial coronal (IC) and peak coronal (PC) angles, indicating greater knee abduction, and smaller peak sagittal (PS) angles, indicating less knee flexion, during a DVJ in keeping with previously demonstrated findings.
Methods
Ethics approval was received from the Research Ethics Office of the Faculty of Medicine and Health Sciences of McGill University before the start of this investigation, and informed consent was obtained from all participants in this study. After consultation with the coaches and training staff, all participants were tested during predetermined times. The enrollment period lasted from September 2017 to May 2018.
Participants and Injury Surveillance
Collegiate varsity athletes were prospectively enrolled in the study before the start of their athletic season. Male and female varsity athletes were eligible for inclusion. Exclusion criteria were athletes <18 years or >30 years or the presence of a lower limb injury at the time of consent. Athlete participants were followed until the end of their respective sport seasons. Data collection included injury reports and clinical data, including sex, age, body mass index (BMI), and sport played. Suspected ACL injuries were confirmed by magnetic resonance imaging and, for those athletes undergoing ACL reconstruction, under direct visualization with arthroscopy. Noncontact ACL injuries were defined as those occurring in the absence of a direct blow to the affected limb.
Motion Capture System
Testing was conducted during the varsity athletes’ respective preseason practice sessions. The motion capture system was connected to a personal computer with software developed using an open-source software development kit (Kinect V2; Microsoft). The system was mounted on a tripod 2.5 m away from the athletes, who were instructed to begin their DVJ from a 31-cm box. Participants were instructed to stand with the balls of their feet over the edge of the box, lean forward with their chest such that they fell off of the box, land with both feet simultaneously, absorb their weight, and immediately bounce back up vertically to jump as high as possible. Participants were offered 1 practice DVJ to ensure the jump would be performed properly. No standardized warm-up was performed; however, 3 DVJs were performed in succession in keeping with the protocol outlined by Hewett et al. 10
The motion capture system employed in this study uses an infrared depth sensor with a capture rate of 30 frames per second to track 3-dimensional movement. 9 Our software used a set of formulas that incorporated force vectors from the knee to the hip as a surrogate for the femur and from the knee to the ankle as a surrogate for the tibia (Figure 1A). These formulas provided measurements of knee abduction in the coronal plane (Figure 1B) and knee flexion in the sagittal plane (Figure 1C) at every frame throughout the DVJ. The software used in this study did not apply inverse kinematics to adjust sagittal knee angles based on coronal abduction angles. To extract the IC, PC, and PS angles, our software was designed to recognize specific movements throughout a DVJ (kinematic triggers). The kinematic trigger that our system used to identify the initial contact frame was the moment at which the foot joint stopped traveling in the downward direction, indicating that the participant had contacted the floor. Subsequently, the kinematic trigger used to indicate the peak landing frame was the moment at which the ankle joint and hip joint were closest to each other. Our software generated an Excel file with the IC, PC, and PS angles for further analysis.
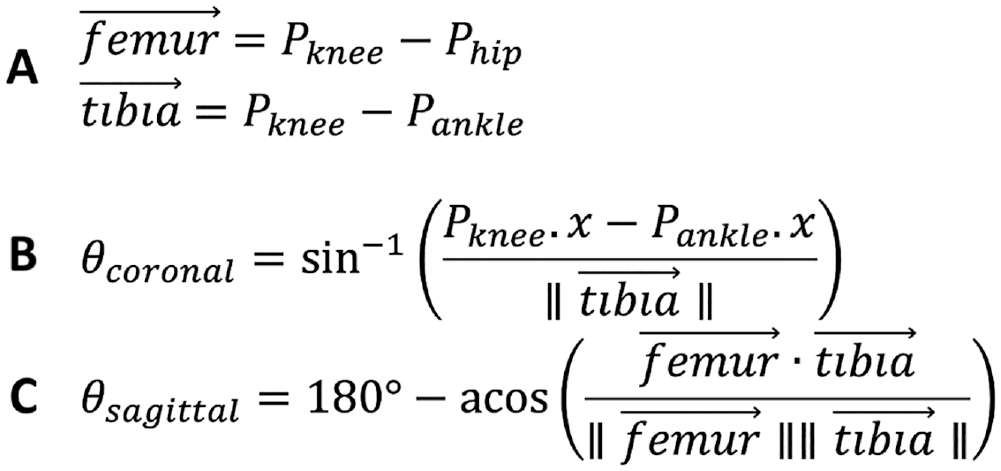
Formulas used by our software. (A) Vector definition of femur and tibia. (B) Formula for calculating coronal knee abduction angles. (C) Formula for calculating sagittal knee flexion angles.
Statistical Analysis
Assessment of kinematic knee angles was performed by comparing the parameters discussed above with ACL injury parameters previously established in a study by Hewett et al. 10 In that study, the investigators found a significant difference in the mean initial contact coronal abduction angle, peak contact coronal abduction angle, and peak contact sagittal flexion angle between athletes who sustained noncontact ACL injuries and those who did not injure their ACL. In keeping with the same protocol, each participant performed 3 DVJs. 10 Faulty jump data were defined as knee angles measured by the motion capture system that were not physically feasible and were inconsistent with the visual recordings as verified by a researcher blinded to injury outcomes. After faulty jumps were excluded, the angles from both knees for each athlete’s eligible jumps (ranging from 1 to 3 jumps) were averaged to create 1 IC, 1 PC, and 1 PS angle per athlete.
The Shapiro-Wilk test was used to determine the normality of the parameters. The independent-samples t test was used to compare the mean knee angles between injured and uninjured athletes. Receiver operating characteristic (ROC) analysis with 5-fold cross-validation was used to further assess the prognostic ability of each parameter and to subjectively determine the optimal angle cutoffs for identifying athletes at high risk of noncontact ACL injury based on sensitivity and specificity. A 5-fold cross-validation was used instead of traditional ROC analysis to provide a more robust and accurate representation of each parameter’s prognostic value, given the relatively low number of injury events expected in this study cohort. Knee angles are reported as mean ± SD. Shapiro-Wilk tests and independent-samples t tests were performed using statistical software (SPSS Version 27; IBM), and P < .05 was interpreted as statistically significant. ROC analysis with 5-fold cross-validation was performed using Python with code from the Scikit-learn library.17,21
Results
A total of 102 participants were recruited for this investigation. After exclusion of athletes with no valid jumping data, 101 participants remained, including 64 male and 37 female varsity athletes (Figure 2). Participant characteristics are summarized in Table 1, and type of sports participation is presented in Figure 3. At the end of the 8-month trial period, 5 athletes (4.95%) sustained noncontact ACL tears, including 2 male and 2 female basketball players and 1 male soccer player. None of the athletes sustained concurrent meniscal injuries, whereas the male soccer athlete sustained a concurrent low-grade lateral collateral ligament injury. The noncontact mechanism of each ACL injury was obtained directly from the athlete as well as from the athletic trainers and physicians looking after each athlete. Descriptive statistics for all 3 DVJ parameters are summarized in Table 2.
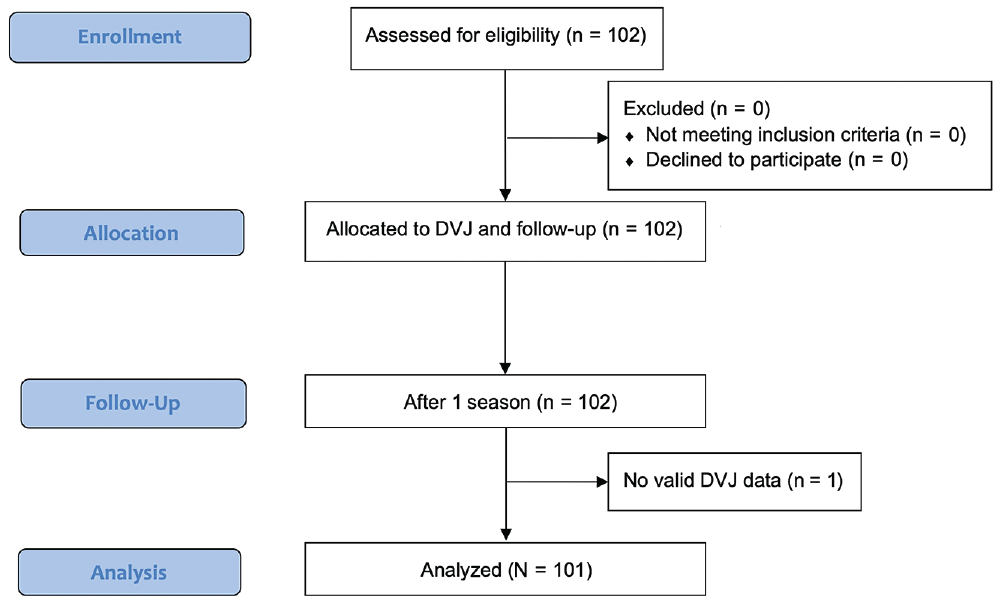
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flowchart. DVJ, drop vertical jump. Figure shows the sports participation of the 101 athletes who were included for analyses.
Participant Characteristics a
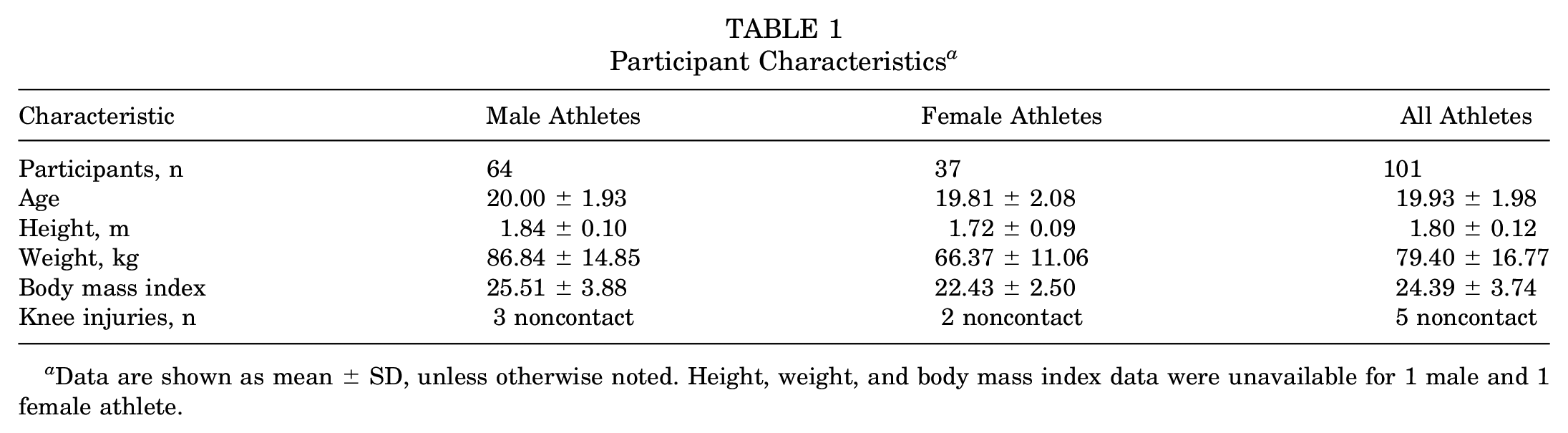
Data are shown as mean ± SD, unless otherwise noted. Height, weight, and body mass index data were unavailable for 1 male and 1 female athlete.
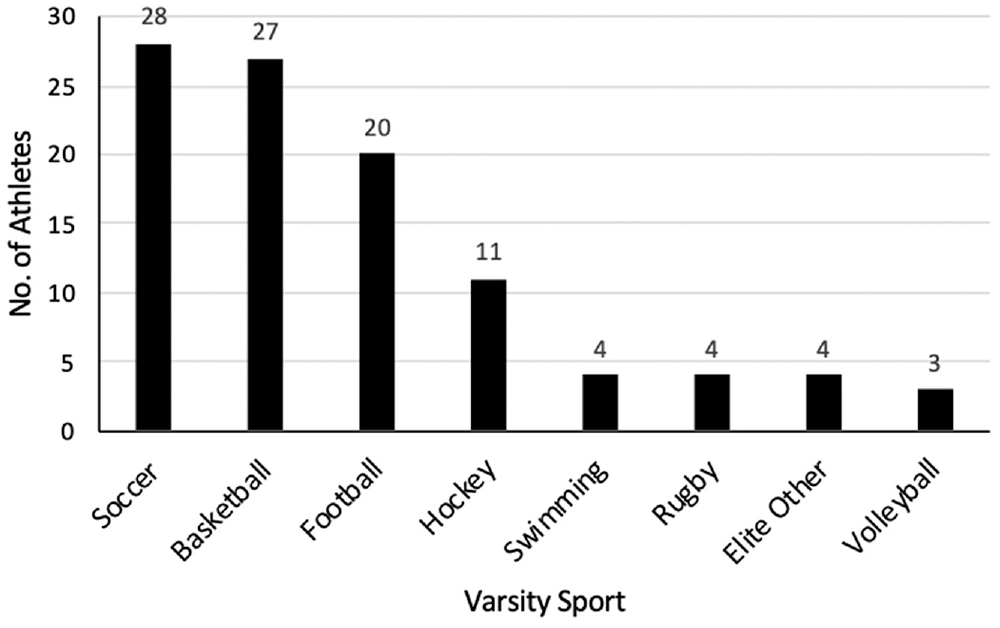
Breakdown of the type of sports participation from the of 101 athletes included for analysis (of 102 total recruited athletes).
Descriptive Statistics for Drop Vertical Jump Parameters a
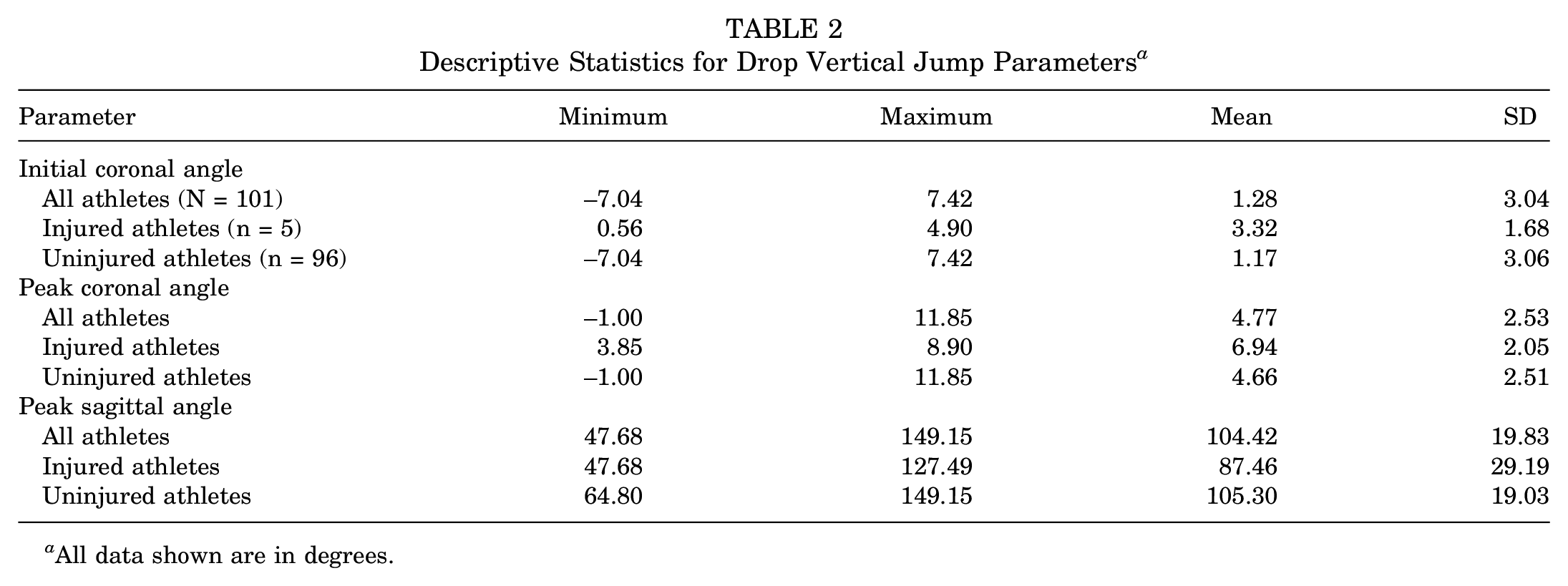
All data shown are in degrees.
DVJ Parameter Comparison
Based on the Shapiro-Wilk test for normality, the IC, PC, and PS angles were all normally distributed (P = .624, .858, and .958, respectively). Accordingly, independent-samples t tests were performed to compare the mean knee angles between injured and uninjured athletes. There was no significant difference in IC angle between injured and uninjured athletes (P = .124). PC angle was significantly greater in injured athletes (6.94°± 2.05°) than in uninjured athletes (4.66°± 2.51°), indicating more knee abduction (t99 = 1.99; P = .049). Likewise, PS angle was significantly smaller in those who injured their ACL (87.46°± 29.19°) compared with those who did not (105.30°± 19.03°), indicating less knee flexion (t99 = 1.99; P = .049).
Assessment of Prognostic Ability
ROC analysis with 5-fold cross-validation determined that the IC angle showed a mean area under the curve (AUC) of 0.88 ± 0.09 with 80% sensitivity and 72% specificity on our cohort at a cutoff of 2.96° of knee abduction (Figures 4A and 5A). Similarly, the PC angle showed a mean AUC of 0.92 ± 0.10 with 80% sensitivity and 72% specificity at a cutoff of 6.16° of knee abduction (Figures 4B and 5B). Finally, the PS angle showed a mean AUC of 0.90 ± 0.16 with 80% sensitivity and 74% specificity at a cutoff of 93.82° of knee flexion (Figures 4C and 5C).
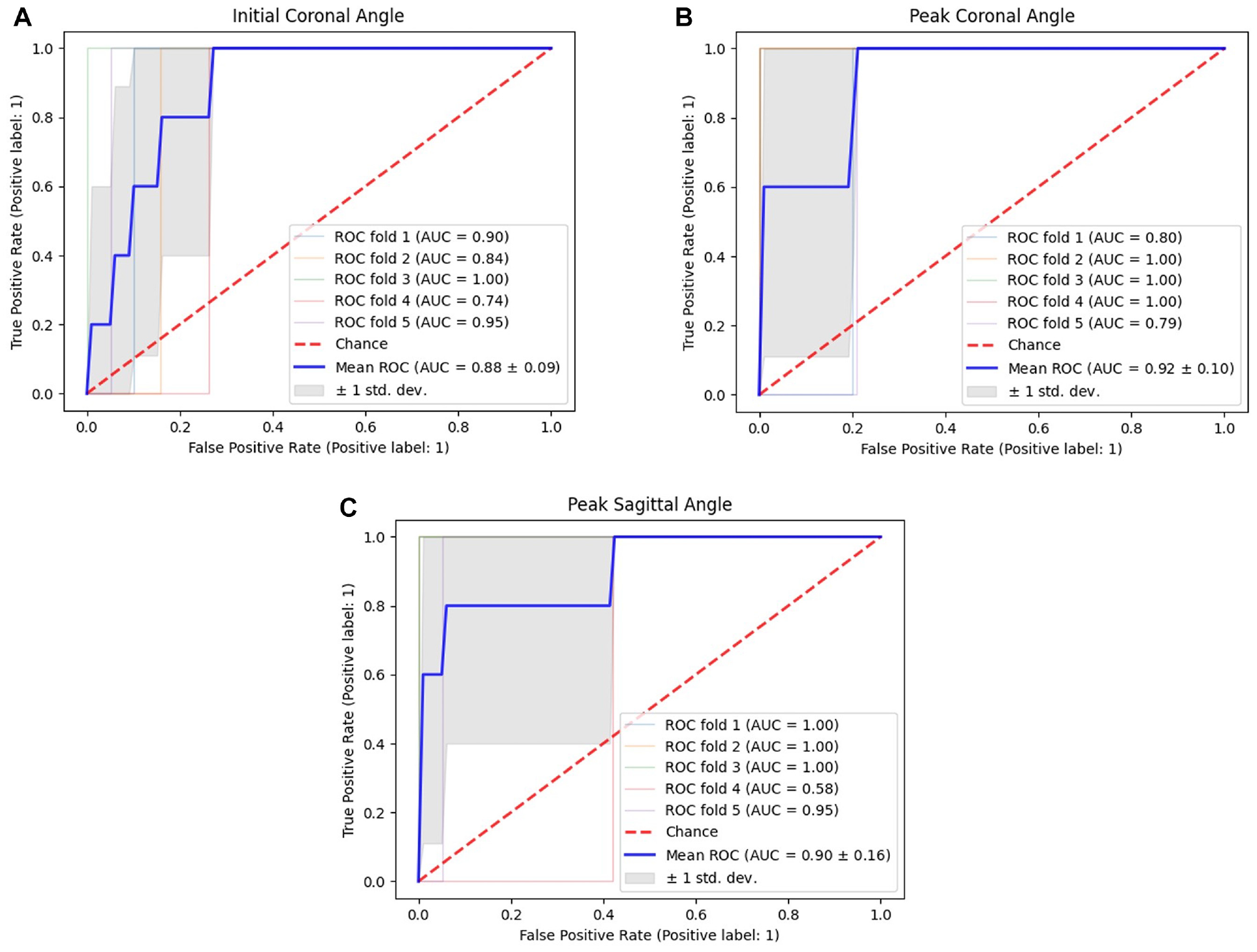
Receiver operating characteristic (ROC) curves for knee joint kinematic angles measured by the motion capture system. The mean area under the curve (AUC) was as follows: (A) initial coronal angle, 0.88 ± 0.09; (B) peak coronal angle, 0.92 ± 0.10; and (C) peak sagittal angle, 0.90 ± 0.16.
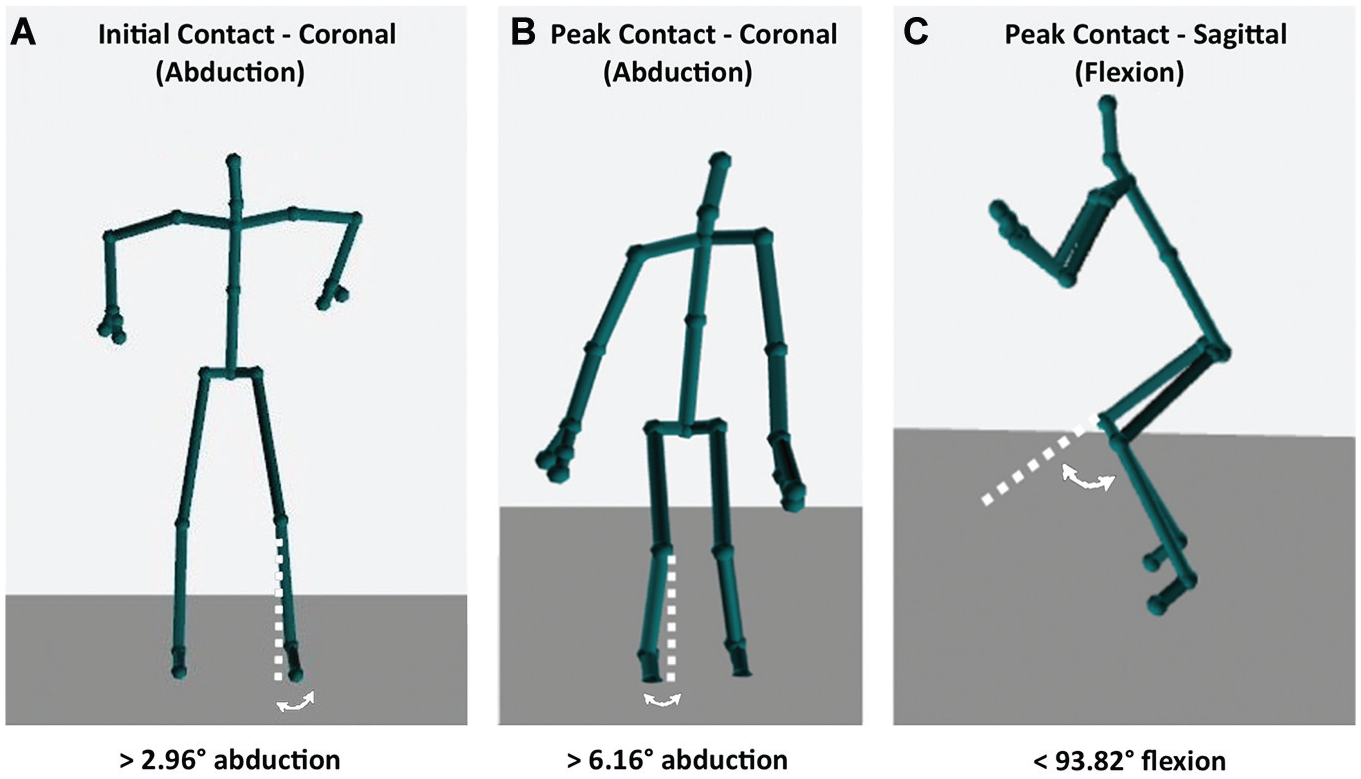
Images of the optimal knee joint kinematic angle cutoffs associated with increased risk of noncontact anterior cruciate ligament tear as generated by the motion capture system software. (A) Initial coronal angle >2.96°. (B) Peak coronal angle >6.16°. (C) Peak sagittal flexion angle <93.82°.
Discussion
In the present study, an affordable motion capture system coupled to a personal computer was used to assess jumping kinematics of male and female collegiate varsity athletes during a DVJ. Peak coronal abduction angle and peak sagittal flexion angle were shown to be excellent predictors of ACL injury, whereas initial coronal angle demonstrated questionable reliability as a risk prediction parameter.
The assessment of jumping kinematics to predict risk of ACL injury is an emerging field in orthopaedic and sports medicine research. The DVJ is a validated method for physical ACL injury risk assessment, the theory being that individuals who demonstrate poor lower extremity biomechanics are at higher risk of ACL injury.7,18 Hewett et al 10 used motion capture software to prospectively assess jumping kinematics of 205 female athletes participating in cutting sports. Those investigators determined that the athletes who sustained a noncontact ACL injury had significantly greater initial and peak knee coronal abduction angles and smaller peak sagittal flexion angles during a standardized DVJ. Although motion analysis is an important breakthrough in understanding factors that predispose individuals to ACL injury, high cost and limited access pose a barrier to widespread implementation of motion analysis during routine preseason physical assessment. Compared with the simpler motion capture system used in this study, traditional motion analysis laboratories are more expensive, require more staff to run accurately, and are more labor intensive. 9
Another method of assessing jumping biomechanics for prediction of injury is an assessment done by a trained strength and conditioning coach or kinesiologist. These health care professionals will likely be able to identify which athletes are at an increased risk of injury based on a number of parameters that these professionals have learned through years of experience. However, conflicting evidence is found in the literature regarding the reliability and validity of such an assessment method. 12
We found that the PC angle was significantly greater in athletes who sustained noncontact ACL injuries compared with those who did not injure their ACL. Conversely, the mean PS angle was significantly smaller in injured athletes compared with uninjured athletes. These findings are consistent with those of Hewett et al 10 and provide further validation that these neuromuscular characteristics can increase the risk for ACL injury in varsity athletes. Furthermore, although the findings of Hewett et al were based on a cohort of only female athletes, the present study consisted of 63% male athletes. The extension of previous findings on this cohort suggests that PC and PS angles have the potential to accurately risk-stratify athletes of both sexes. Conversely, although Hewett et al found that IC angle was significantly greater in injured athletes, we found no significant difference in IC angle between injured and uninjured athletes in this study. This inconsistency may be an indication that IC angle is a weaker prognostic indicator of noncontact ACL injury compared with PC and PS angles among all athletes. Alternatively, this may indicate that IC is a weaker prognostic indicator only in male athletes, given the high percentage of male athletes in this study. Future studies should investigate IC angle in male and female athletes separately and together to better characterize the reliability of IC angle as a DVJ parameter for predicting ACL injury.
Using these data and ROC analysis with 5-fold cross-validation, we further investigated the ability of these angles to identify athletes at increased risk for noncontact ACL injury. IC angle showed an AUC of 0.88, with a sensitivity of 80% and specificity of 72% at a cutoff of 2.96° of abduction. PC angle also showed a promising AUC, 0.92, with an 80% sensitivity and 72% specificity at a cutoff of 6.16° of abduction. PS angle showed an AUC of 0.90 with an 80% sensitivity and 74% specificity at a cutoff of 93.82° of flexion. With an AUC of 0.5 corresponding to a diagnostic accuracy equal to random chance and 1.0 corresponding to perfect diagnostic accuracy, IC angle would be considered a good predictor of ACL injury whereas PC and PS angle would be considered to have excellent prognostic ability. 11 This evidence suggests that initial and peak coronal angle, as well as peak sagittal angle, can be valuable parameters to include in an ACL injury risk screening tool for identifying high-risk athletes who may benefit from targeted injury prevention programs. Interestingly, the AUC was the lowest for IC angle, which was the only parameter that was not significantly different between injured and uninjured athletes. This consistency in pattern further supports the hypothesis that IC angle may be a relatively weaker prognostic indicator of ACL injury, either in all athletes or primarily in male athletes.
At the end of each athlete’s respective season, his or her ACL injury status was identified, with all ACL injuries confirmed clinically and using magnetic resonance imaging. A total of 5 of the 101 athletes (4.95%) enrolled in the study sustained a complete ACL tear during the course of the investigation, which is a substantially higher incidence than has been reported in the literature. In 2016, a systematic review and meta-analysis found that the highest incidence of ACL injury was in female soccer athletes at 1.1% per season and male football athletes at 0.8% per season. 8 The elevated incidence in our cohort may partially be explained by significant increasing trends in ACL injury in collegiate basketball, football, ice hockey, and volleyball. 1 However, we hypothesize that other factors such as the intensity of training and hours of exposure per season are at play, because ACL injury risk is multifactorial in nature. In the present study, 3 of the 5 injured athletes were male, and the injury rates were similar between sexes (4.69% of male and 5.41% of female patients). Although female sex is widely known to be a significant risk factor for noncontact ACL injury, the sample size of this study did not allow for assessment of sex as an independent risk factor for ACL injury.24,25
Although our findings suggest that the knee kinematics measured during a DVJ can be effective parameters for a screening tool for noncontact ACL injury, largely consistent with those of Hewett et al, 10 other investigations have had difficulty replicating these results. An investigation by Krosshaug et al 12 prospectively examined 710 elite female handball and soccer athletes and did not find an association between jumping angles measured during a DVJ and the risk of noncontact ACL injury. Although these results are not in keeping with our findings, they potentially highlight the need for comprehensive screening protocols that use both knee kinematics and clinical assessment to provide a more holistic approach to risk stratification. Risk factors that are easily identifiable in the clinical setting, such as weight and BMI in female athletes and previous knee injuries in all athletes, may provide different yet complementary information in conjunction with kinematic data. As a result, a future direction will be to input clinical risk factors into the motion capture system’s algorithm to provide a more comprehensive risk assessment for noncontact ACL injury.
As mobile health begins to emerge as a field, sports teams are looking to incorporate portable medical technology in the assessment of their athletes. The motion capture system used in this study, equipped with infrared depth sensors and a skeletal tracker, has proved to be convenient and inexpensive for kinematic imaging. 13 Although originally designed for gaming, the corresponding open source software development kit has allowed programmers to use the built-in skeleton tracking for a number of health care applications, including stroke rehabilitation, Parkinson disease rehabilitation, at-home cardiovascular rehabilitation, and now athlete kinematics.9,16,22,26 Given the advancements both in the motion analysis capabilities of affordable systems and in ACL injury prediction, the integration of these 2 technologies is both logical and desirable. As discussed above, traditional motion analysis systems are costly, time-consuming, and limited to highly specialized training centers. Conversely, the motion capture system used in this study consists of a camera that is secured on a tripod, which is then plugged into a personal computer. The total setup time of this system is <5 minutes. Each DVJ takes a mean of 8 seconds to perform, preceded by 10 seconds to start the recording and followed by 12 seconds for analysis. The total mean time of 1 athlete jump is approximately 30 seconds. The user interface has been developed to be user-friendly and therefore does not require a trained professional to run the test.
Along with incorporating clinical parameters into the risk stratification algorithm, future directions will be aimed at improving portability to facilitate on-field assessment and developing novel ways to improve diagnostic accuracy. With improved cell phone camera technology, offering this platform on a mobile device could facilitate widespread adoption of this tool, an important consideration for effective, large-scale screening programs. Recent advancements in artificial intelligence have also resulted in machine learning algorithms capable of identifying features unique to ACL-injured knees from motion analysis data. 19 The data generated by our software could be amenable to similar analyses in an effort to determine previously unknown patterns in knee biomechanics that may ultimately improve screening for noncontact ACL injury.
Despite the promising results of the present investigation, some potential limitations merit discussion. The 30 Hz sample rate of the motion capture system from this study may have posed a limitation to accurately capturing and identifying the frames at which IC, PC, and PS angles should be extracted. However, despite the 30 Hz frame rate, the system used in this study has demonstrated excellent correlation with a gold standard Vicon motion capture system in the identification of the knee-ankle separation ratio at initial contact and peak contact during a DVJ. 9 The knee-ankle separation ratio requires tracking of the knees and ankles throughout a DVJ, similar to what was required for determining coronal and sagittal knee angles in this study. Furthermore, unpublished results from our laboratory have demonstrated that this system captures IC, PC, and PS angles during a DVJ with intraclass correlation coefficients between 0.771 to 0.917 in agreement with a Vicon system, which used 10 cameras capable of capturing at a frame rate of 120 Hz. Ultimately, these findings suggest that the 30 Hz frame rate may be an acceptable technical limitation in a more affordable, practical, and highly scalable motion capture system that does not limit its ability to accurately determine the critical parameters of a DVJ to an appreciable extent. It is also worth mentioning that because only 1 motion capture system was used to track the DVJ from a frontal view in this study, it is unknown whether sagittal knee angles would be more accurately tracked by the same motion capture system from a side view. A future study may compare the accuracy of sagittal knee angle tracking from frontal and side views using a device similar to the one in this study, with a gold standard motion tracking setup for standardization. Although this may fill a knowledge gap and provide perspective on the possible advantage of tracking DVJs simultaneously from front and side views, we hypothesize that the potential benefit of adding a second motion capture system to the current setup would not be worth the trade-off of practicality, simplicity, and affordability. These properties are integral to the overall goal of developing an effective setup for ACL injury risk prediction that can easily be deployed on the sideline or in the clinic. The limited number of participants and ACL injuries is another potential limitation of this study, as a larger cohort with more injury data may provide more granularity in determining optimal angle cutoffs for identifying high-risk athletes. Additionally, our investigation looked at each parameter individually as potential risk factors for predicting noncontact ACL injury. In the goal of ultimately developing a comprehensive screening tool, future studies should examine how interpreting these parameters together can further increase prognostic accuracy by increasing both sensitivity and specificity. Other risk factors such as patient characteristics may be studied in conjunction with kinematic measurements to develop a more holistic risk assessment approach.
Conclusion
Our unique software, which uses an affordable motion capture system to perform motion analysis during a DVJ, has identified increased peak coronal abduction angle and decreased peak sagittal flexion angle to be significantly associated with an increased risk for ACL injury. ROC analysis with these data found that initial coronal angle was a good predictor of ACL injury, whereas peak coronal angle and peak sagittal angle were excellent predictors of ACL injury. Optimal cutoffs for each DVJ parameter yielded sensitivities of 80% and specificities ranging from 72% to 74% in the cohort in this study.
Footnotes
Acknowledgements
The senior author (P.A.M.) acknowledges the support of Consultation Semperform Inc to this research endeavor. The authors gratefully thank Patrik Abdelnour (McGill University, Canada) for their invaluable contributions toward developing and optimizing the motion analysis software that was used alongside the Microsoft Kinect device for this study.
Submitted February 1, 2022; accepted December 13, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: PAM (P.A.M.) would like to acknowledge the support of Consultation Semperform Inc to this research endeavor. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.