
Abstract
Background:
Patellofemoral instability (PFI) has several known anatomic factors, including trochlear dysplasia and patellar maltracking. While studies have documented altered lower-extremity gait biomechanics in patients with PFI, the relationship between these biomechanical abnormalities and anatomy has not been thoroughly investigated, particularly during sport-related tasks.
Purpose/Hypothesis:
The purpose of this study is to examine the associations between preoperative anatomic characteristics and lower-extremity kinematics at sports clearance in adolescents after medial patellofemoral ligament reconstruction for PFI. It was hypothesized that patellar maltracking, trochlear dysplasia, and frontal plane malalignment would strongly correlate with abnormal lower-extremity biomechanics.
Study Design:
Descriptive laboratory study.
Methods:
Patients aged 10 to 18 years who underwent primary medial patellofemoral ligament reconstruction for PFI between 2019 and 2023 were tested at sports clearance visits. Joint angles of the hip and knee were calculated during descent of a drop vertical jump. Preoperative radiographs and magnetic resonance imaging were utilized to record tibial tuberosity–trochlear groove (TT-TG) distance, tibial tubercle–posterior cruciate ligament (TT-PCL) distance, trochlear width (TW), trochlear sulcus depth (TSD), lateral inclination angle, patellar tilt angle (PTA), Caton-Deschamps Index (CDI), and femorotibial angle. Spearman correlations assessed relationships between preoperative anatomy and drop vertical jump kinematics.
Results:
In total, 17 participants were tested (8 male, 15 unilateral; mean ± SD age, 15.5 ± 1.4 years; height, 166.3 ± 11.4 cm; weight, 65.1 ± 19.4 kg; days after surgery, 199.9 ± 30.8). TT-PCL, TT-TG, and TSD were not significantly correlated with kinematics. Greater dynamic pelvic obliquity (r = 0.672; P = .004) and internal pelvic rotation (r = 0.508; P = .044) were positively correlated with femorotibial angle. Pelvic obliquity was negatively correlated with CDI (r = −0.710; P = .007). Greater severity of patellar malalignment and trochlear dysplasia (decreased TW, r = −0.486 [P = .048]; increased PTA, r = 0.689 [P = .002]) was associated with greater hip abduction. TW (r = 0.503; P = .040) and CDI (r = −0.608; P = .028) were also correlated with internal hip rotation. Greater knee flexion during landing was correlated with decreased PTA (r = −0.547; P = .023) and CDI (r = −0.560; P = .046). Greater dynamic knee valgus was positively correlated with TW (r = 0.483; P = .049), and greater internal knee rotation was positively correlated with lateral inclination angle (r = 0.513; P = .035).
Conclusion:
Larger degree of patellar maltracking, trochlear dysplasia, and frontal plane malalignment correlated to distinct biomechanical patterns during dynamic movements. Statistically significant associations were found with internal knee and hip rotation, pelvic instability, hip abduction, and knee stiffness. Conversely, TT-PCL, TT-TG, and TSD demonstrated no significant association with postoperative kinematic patterns in patients with PFI.
Clinical Relevance:
Understanding how anatomic abnormalities relate to postoperative biomechanics can help clinicians identify adolescents at risk for persistent movement deficits after medial patellofemoral ligament reconstruction. These findings highlight the importance of incorporating individualized anatomic considerations into postoperative rehabilitation and return-to-sport assessments.
Patellofemoral instability (PFI) occurs when the patella is dislocated from the trochlear groove, resulting in symptoms of pain, hemarthrosis, and redislocation. 35 Acute PFI affects 1:1000 children between the ages of 9 and 15 years, 15 with recurrence in adolescence as high as 80%. 16 As such, the ongoing nature of PFI presents difficulty for athletes attempting to return to sport without persistent pain and fear of redislocation. Treatment for PFI includes nonoperative and operative management, with recurrent PFI frequently addressed operatively. One such procedure is medial patellofemoral ligament (MPFL) reconstruction, given the MPFL's role in lateral stabilization of the knee. 41 This procedure demonstrates safe and effective outcomes in children and adolescents,13,18,26 reducing the risk of recurrent instability to <5%.7,33
Associations with PFI include patellar maltracking, trochlear dysplasia, and abnormal limb alignment.15,16,28 Primarily, trochlear dysplasia and patella alta have been implicated as concerns for recurrent instability. 29 Trochlear sulcus depth (TSD)32,39 and trochlear asymmetry, measured as lateral inclination angle (LIA), 36 represent some methods of quantifying trochlear dysplasia. Patellar tilt angle (PTA) 27 and frontal plane malalignment of the lower extremity 29 are also anatomic indicators of PFI risk. Finally, tibial tuberosity–trochlear groove (TT-TG) distance is identified as a risk factor for PFI, 21 with Dickens et al 10 reporting 12.1 mm in patients with PFI as compared with 8.5 mm in healthy young adults.
Beyond anatomic variation, a number of investigations have described movement abnormalities in patients with PFI; however, these reports have focused solely on simple movement tasks, such as gait. Specifically, gait analyses have indicated that PFI elicits increased knee flexion, decreased hip flexion, and variable ankle mechanics.1,16,25 Patients with PFI also tend to decrease quadriceps recruitment and walk with decreased speed and stride length. 16 Dewan et al 9 postulated this to be an avoidance of simultaneous early knee flexion, external tibial rotation, and quadriceps contraction, which they identified as a high-risk period of the gait cycle for dislocations. As greater stride length and speed correspond to larger joint moments, 2 it is likely that those with PFI adapt their movement patterns to avoid redislocation, possibly even after surgical treatment.
While alterations of lower-extremity biomechanics have been documented in patients with PFI, correlation with dysplasia and extensor mechanism malalignment has not been well studied.4,8,31 Sport-related tasks such as the drop vertical jump (DVJ) may yield particularly informative data, as kinematics associated with patellofemoral pain may be identified. 3 For those planning to return to sport, correlations of preoperative anatomic characteristics and functional task joint mechanics at time of return to play may provide insight for athletes and coaches regarding patient-specific physical therapy targets to reduce known kinematic risk factors to which they are anatomically predisposed.4,40 Therefore, the purpose of this exploratory study was to investigate associations between preoperative anatomic characteristics and lower-extremity kinematics collected at sports clearance in adolescent patients after MPFL reconstruction for PFI. It was hypothesized that patellar maltracking, trochlear dysplasia, and frontal plane malalignment would strongly correlate with abnormal pelvis, hip, and knee biomechanics during dynamic movements.
Methods
Study Design and Participants
A prospective cohort of adolescent patients between 10 and 18 years of age treated with primary MPFL reconstruction for PFI was recruited between 2019 and 2023. Recruited participants were seen for a single visit in a motion capture laboratory at the time of sports clearance (ie, physician provided permission to return to sport activities without restrictions). Patients with PFI with nonsurgical treatment plans and those treated surgically who had not yet been cleared for sport by their medical provider were excluded. Before testing commencement, study approval was obtained from a regional institutional review board (approval 2019-0973), and all participants and parents provided informed assent and/or consent. Participants were tested in comfortable clothing and their athletic footwear of choice.
Procedures
Participants were instrumented with retroreflective markers placed on relevant bony landmarks of the lower extremities, including marker clusters placed on the lateral thigh and anterior shank.1,2 A 14-camera motion capture system (Vicon Motion Systems Ltd) with a collection frequency of 240 Hz was used to capture 3-dimensional kinematic data of a DVJ. The starting platform for the DVJ was a plyometric box 31 cm tall, with a landing area composed of two 60 × 60–cm squares. The assigned jump distance was equal to one half the participant's height, measured from the front of the box to the center of each square. The verbal instructions to the participant were to “jump horizontally, landing with one foot in each square, and then perform a maximum vertical jump.” Practice trials were encouraged to verify participant understanding of and comfort with the given instructions. Following practice trials establishing participant comfort with the task, 3 successful trials were collected for the DVJ, with unsuccessful trials defined and resulting in exclusion from analysis if the participant did not land with 1 foot in each square or did not complete the maximum vertical jump. Dynamic variables of interest included pelvic obliquity, internal pelvic rotation, hip abduction, internal hip rotation, knee flexion, knee valgus, and internal knee rotation. Internal knee rotation quantifies rotation of the tibia relative to the femur.
Preoperative anatomic characteristics of each participant were collected via radiographs and magnetic resonance imaging with a field strength of 3.0 T. Magnetic resonance imaging axial images were used to measure the TT-TG, tibial tubercle–posterior cruciate ligament distance (TT-PCL), trochlear width (TW), TSD, LIA, PTA, and Caton-Deschamps Index (CDI). Radiographs were used to determine the femorotibial angle (FTA). All image measurements were made by a single investigator with 20 years of orthopaedic experience. To measure the TT-TG, a line was first drawn from the midpoint of the tibial tubercle tangent to the posterior femoral condylar line. Parallel to this line, a second line was drawn through the trochlear groove at its deepest point on the first axial image, in which it was visible with the full medial and lateral extent of trochlear cartilage visible. In the axial plane, the TT-TG distance was the distance from the second line to the midpoint of the tibial tuberosity (Figure 1A). 3 TT-PCL was measured as the mediolateral distance between the midpoint of the insertion of the patellar tendon on the tibial tubercle and the medial border of the PCL tangent to the posterior tibial condylar line (Figure 1B). 34 TW was measured as the distance between the medial and lateral trochlear parallel lines, both drawn at the maximum trochlear cartilage width and tangential to the femoral posterior condylar line (Figure 1A). 37 TSD was measured as the mean of the maximum anterior-posterior distance of the medial and lateral femoral condyles minus the distance between the deepest point of the trochlear groove and the line parallel to the posterior condylar surfaces (Figure 1A). 19 LIA was measured as the angle between a line tangential to the subchondral bone of the posterior aspect of the femoral condyles and a line along the lateral trochlear facet (Figure 1C). 19 PTA was measured as the angle between the line where the posterior femoral condyles were largest and the maximal patellar width (Figure 1C). 19 CDI was measured as a ratio of the distance from the inferior margin of the patellar articular surface to the nearest point on the tibial plateau over the length of the articular surface (Figure 1D). 4 FTA was measured on full-length standing EOS radiographs (EOS Imaging) as the angle formed between the anatomic axes of the tibia and femur, defined by a line drawn from the anatomic axis of the femur to the knee center and a line drawn from the center of the ankle to the same knee center, subtracted from neutral alignment (180°). 4 Thus, a greater FTA indicates greater genu valgum. All distance measures were recorded in millimeters. Upright EOS radiography was used as it provides more accurate lower limb measurements and significantly less radiation exposure than computed tomography scanograms and conventional radiographs. 14

Anatomic measurements. CDI, Caton-Deschamps Index; LIA, lateral inclination angle; PTA, patellar tilt angle; TSD, trochlear sulcus depth; TT-PCL, tibial tubercle–posterior cruciate ligament; TT-TG, tibial tuberosity–trochlear groove; TW, trochlear width.
Data Processing and Analysis
All motion capture trials were processed in Vicon Nexus (OMG plc). Marker trajectories were filtered through a Woltring filter with a predicted mean square error of 10 mm2. A custom MATLAB model (MATLAB 2022a) was used to compute the segment and joint angles for the pelvis, hip, and knee, with the angle of the pelvis segment defined relative to the global coordinate system. DVJ task events were marked by a custom MATLAB code that identified the descent phase of the DVJ, defined as the period between initial contact with the ground and the lowest position of the ipsilateral hip joint center. Segment and joint angles were analyzed across the descent phase of the DVJ and then computed by a custom MATLAB code.
Given a lack of normality, nonparametric analyses were performed. Specifically, Spearman correlations were utilized to identify relationships between preoperative anatomy and DVJ kinematics of the affected limb. For cases in which the patient was bilaterally affected, the limb most recently treated surgically was included for analysis. Statistical tests were run by using SPSS Statistics for Windows (Version 224.0; IBM), and statistical significance was determined with an alpha value of .05.
Results
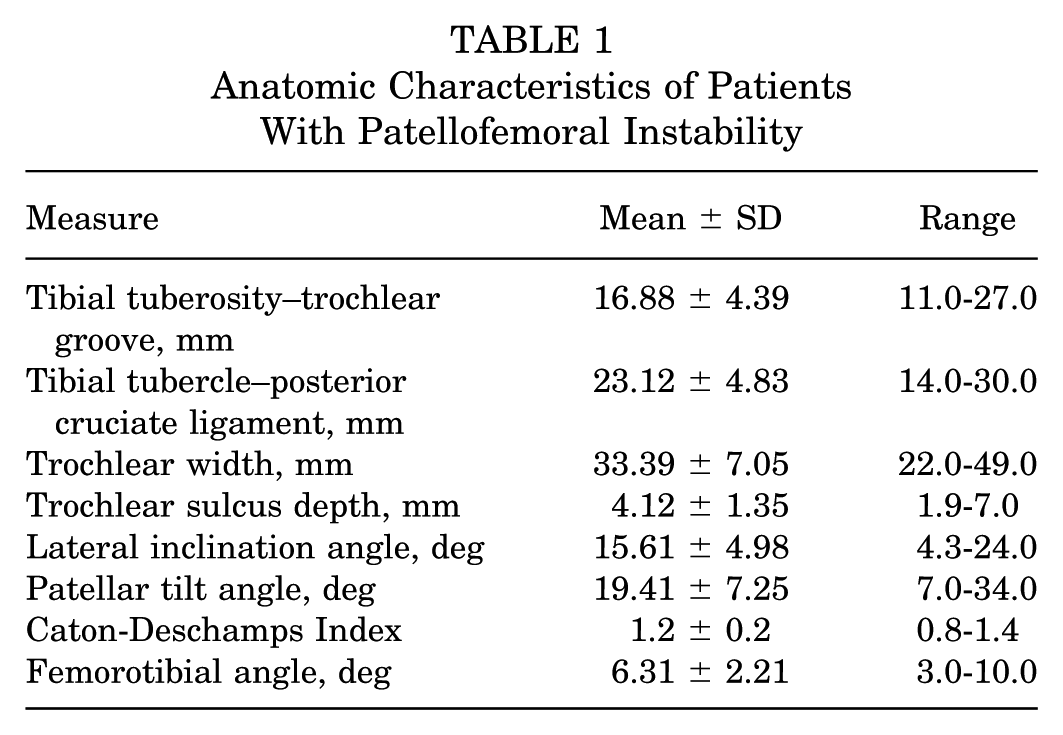
A total of 17 participants were tested (8 male, 15 unilateral; mean ± SD age, 15.5 ± 1.4 years; height, 166.3 ± 11.4 cm; weight, 65.1 ± 19.4 kg). Participants were 199.9 ± 30.8 days postoperative at the time of testing. Mean anatomic characteristics are presented in Table 1. TT-PCL, TT-TG, and TSD were not significantly correlated to any kinematic variable. Four patients had incomplete CDI data and were not analyzed for CDI subanalyses.
Anatomic Characteristics of Patients With Patellofemoral Instability
Greater pelvic obliquity (r = 0.672; P = .004) and internal pelvic rotation (r = 0.508; P = .044) were positively correlated with FTA, which represented the magnitude of inherent genu valgum. These patients exhibited biomechanical signs of pelvic asymmetry, specifically pelvic drop and leading on the affected side and thus potential unsteadiness upon landing. Greater pelvic obliquity was also negatively correlated with CDI (r = –0.710; P = .007).
Similarly, at the hip, increased abduction was negatively correlated with TW (r = −0.486; P = .048) and positively correlated with PTA (r = 0.689; P = .002). As such, greater severity of trochlear dysplasia and extensor malalignment (decreased TW and increased PTA) was associated with the knee joint moving farther away from the midline, causing greater hip abduction across the descent phase. Internal hip rotation was also positively correlated to TW (r = 0.503; P = .040) and negatively correlated to CDI (r = −0.608; P = .028), indicating that patients with a wider femoral trochlea and less patella alta exhibited greater internal hip rotation throughout descent.
For the knee joint, greater flexion during landing was negatively correlated with PTA (r = −0.547; P = .023) and CDI (r = −0.560; P = .046), indicating that patients with more severe PTA and patella alta exhibited stiffer landings. Furthermore, greater dynamic knee valgus was positively correlated with TW (r = 0.483; P = .049), and greater internal knee rotation was positively correlated with LIA (r = 0.513; P = .035).
Discussion
The purpose of this study was to assess correlations between preoperative knee anatomy and postoperative kinematics in PFI that may serve as foundational data to assist athletes and coaches in expectance of knee performance upon return to play and identify risk management opportunities after treatment for patellar instability with MPFL reconstruction. These results indicated that many measures of preoperative knee anatomy were moderately associated with pelvic instability, coronal plane misalignment at the hip and knee, stiffer landing, and more internal hip and knee rotation during landing. However, TT-PCL, TT-TG, and TSD were not significantly correlated to kinematic abnormalities in the current study. Ultimately, these results suggest that severity of preoperative anatomic abnormality is associated with biomechanical patterns consistent with PFI during dynamic movement even after surgical intervention.
Pelvic Instability
In investigating the movement strategies of a patient population with PFI, it was initially hypothesized that patellar maltracking, trochlear dysplasia, and frontal plane malalignment would be strongly linked to dysfunctional pelvic, hip, and knee kinematics during dynamic movements. Given that, we expected weightbearing strategies to vary considerably from normative movement patterns, as patients employ diverse adaptive mechanisms to manage their conditions and avoid redislocation. As patella alta correlated with less pelvic drop in this cohort, knee extensor strength and/or flexibility could play a role upon landing, particularly if less overall stability on the affected side led to contralateral pelvic drop. In considering FTA, it is reasonable to postulate that inherent valgum could exacerbate dynamic valgus during the landing phase of a jump. 42 However, dynamic knee valgus was not associated with FTA but rather biomechanical signs of pelvic instability. Specifically, the current study revealed that increased FTA (ie, greater genu valgum) was associated with greater pelvic drop and leading on the affected limb during landing. Thus, a potential compensation technique to reduce the weight loaded onto the knee joint involved positioning the ipsilateral pelvis down and more anterior and the contralateral pelvis up and more posterior. This pelvic asymmetry could also be a consequence of poor hip abductor strength and/or trunk control. 23 In patients with patellofemoral pain, it has been theorized that one compensation strategy to adapt to this weakness is elevating the contralateral pelvis,11,30 thus creating an illusion of pelvic drop on the affected limb, but relevant literature on pelvis and trunk compensations is conflicting.
Poor Coronal Plane Alignment
Literature focused on alternative knee injuries that occur in youth sports, such as injury to the anterior cruciate ligament, has established dynamic knee valgus as a strong predictor of injury. 17 Dynamic knee valgus is a combination of movements across all 3 planes, including coronal plane measures of hip adduction and knee valgus. For a PFI population, previous research has demonstrated that hip adduction can impose stress on the iliotibial band and provoke lateral patellar displacement. 22 Thus, a compensation technique employed by these patients may involve greater hip abduction during a dynamic task, as observed in the current study. Specifically, patients who exhibited greater hip abduction during landing had narrower TWs and more severe PTAs. Additionally, patients with narrower TWs exhibited reduced dynamic knee valgus during landing, likely in conjunction with greater hip abduction as the knee joint moved farther away from the midline throughout descent.
Knee Stiffness During Landing
The current study revealed several noteworthy findings related to patients with PFI landing with a stiffer knee. Notably, patients with a greater PTA and patella alta exhibited reduced knee flexion during landing. This observation aligns with previous research indicating that patients with PFI tend to exhibit reduced knee flexion as compared with healthy controls during a single-leg drop, 20 likely as a protective or cautious movement strategy. This landing pattern might serve as a way to prevent patellar subluxation, since knee flexion is often a precursor to subluxation events. 21 Importantly, the current methodology introduced a more dynamic, challenging task as compared with previous research, such as the study by Lucas et al, 25 in which patients did not demonstrate differences in peak knee flexion or extensor moment when compared with controls during gait. Thus, the current study contributes to the understanding of knee flexion patterns in patients with PFI and highlights the importance of dynamic, functionally relevant assessments in elucidating the complex biomechanical factors associated with the condition.
Knee External Rotation and Hip Internal Rotation
A previous study tested healthy controls and 2 groups of patients with PFI with different levels of instability. It identified that the degree of tibiofemoral external rotation on magnetic resonance imaging increased from healthy controls to the moderate stability PFI group and was highest among patients with PFI with the greatest level of instability. 24 Thus, it may be postulated that patients with greater risk of dislocation employ compensatory movements in the transverse plane to adapt to a more neutrally aligned position during movement that avoids patellar dislocation. Upon finding that trochleae with a normal LIA demonstrate greater internal knee rotation (tibial rotation relative to the femur), we suggest that a flattened dysplastic trochlea would correlate with more external knee rotation upon landing. A secondary compensation in the transverse plane could stem from the hip given the association between hip and knee rotation; however, internal hip rotation was not associated with LIA. Instead, greater internal hip rotation was associated with a wider TW and less patella alta. In previous work analyzing gait, peak hip internal rotation angles were not significantly different between patients with PFI and controls. 1 Therefore, the current study unveils novel insights into the dynamic biomechanics of PFI, emphasizing the importance of considering a range of factors beyond static anatomic measurements in understanding and managing this complex condition.
In previous studies attempting to predict the risk of recurrent patellar instability with multiple measures of trochlear dysplasia, an excessive TT-PCL was not as predictive as other measures, as many patients with a low TT-PCL sustained recurrent dislocations.5,6 Thus, in dynamic tasks such as DVJ, the consequences of a high preoperative TT-PCL may not have the same biomechanical influence as other metrics. Similarly, TT-TG did not correlate to biomechanical variables, which is possibly due to its poor inter- and intraobserver reliability among patients with severe dysplastic trochleae. 12 TSD, among other radiographic parameters, may also vary according to the axial slice chosen. 38 As the TSD does not perfectly align with the plane of the femur, imaging with a fully extended knee could lead to a suboptimal axial measurement and partially explain the lack of a significant relationship, although it is unlikely to play a significant role.
Limitations
This study has limitations to note in that the sample size was modest with only 17 participants, 4 of which lacked data allowing patella alta measurement; furthermore, it included patients with bilateral PFI, which may have a specific influence on the preoperative anatomy and return-to-play biomechanics. Additionally, the generalizability of this study's findings to other tasks remains unknown. Another limitation is the lack of postoperative alignment measurements, particularly for PTA, which can change significantly after surgery. Additionally, assessing postoperative patellar lateral shift relative to the trochlear groove could provide valuable insights into surgical outcomes and biomechanical adaptations. Additional anatomic variations such as ligament laxity or muscle strength were not assessed and may have contributed to PFI biomechanics. Motion capture technology has limitations in accuracy, as kinematic changes <3° are considered within the range of error, which was not accounted for in our study. A strength of this study, however, is that it focuses on DVJ in patellar instability rather than gait in patellofemoral pain syndrome, which provides specificity into the performance of dynamic movements in this population.
Given the sparse literature on dynamic movement patterns in patients with PFI, considerable research in this area is needed. Apart from elucidating the association between preoperative anatomy and postoperative DVJ mechanics, future inquiries should identify biomechanical patterns during other tasks, such as a sidestep, squat, single-leg hop, and lateral shuffle. It may also be useful to identify how inherent anatomy modulates postoperative muscle activation and whether these patterns persist later in the postoperative course, such as the 24-month mark. Additionally, a comparison of nonoperative and operative interventions would indicate the influence that pretreatment anatomy has on subsequent biomechanics. Last, further research is needed to determine whether these motion patterns in patients with PFI can improve after strength and neuromuscular training or if these patients reach a plateau in their recovery that markedly differs from patients with optimal biomechanical patterns.
Conclusion
Our study demonstrated that with greater preoperative anatomic abnormality, participants display distinct biomechanical patterns during dynamic movement. Specifically, these patterns include larger degrees of dynamic hip abduction and external knee rotation during descent with less severe dynamic knee valgus and knee flexion during landing. These data provide valuable insights into how extensor mechanism anatomy can associate with movement strategies. Compensatory mechanisms may develop to mitigate instability risk attributed to patellar maltracking, trochlear dysplasia, and frontal plane malalignment. However, if kinematic abnormalities are compensatory, they may also be targets of improvement during the recovery period after surgical mitigation of predisposing factors to instability. These results underscore the importance of further investigation into the relationship of anatomic abnormality with a range of dynamic tasks, such as cutting, jumping, and lateral movements. Understanding these movement patterns could improve rehabilitation strategies, surgical decision-making, and postoperative functional outcomes in patients with PFI.
Footnotes
Final revision submitted July 2, 2025; accepted July 16, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.B.E. receives speaking fees from OrthoPediatrics; support for education from Pylant Medical; nonfinancial support for education from Arthrex; and grants paid to his institution from the Pediatric Orthopaedic Society of North America, American Orthopaedic Society for Sports Medicine, and US Department of Defense–Washington University at St Louis. H.B.E. is also the past president and a current board member of the Texas Orthopaedic Association; an executive committee member of the American Academy of Orthopaedic Surgeons Board of Councilors; an unpaid consultant for Smith & Nephew; and the treasurer of Pediatric Research in Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Texas Southwestern Institutional Review Board (approval 2019-0973).