
Abstract
Background:
Few studies have investigated the biomechanical performance of flat-braided suture tapes versus round-braided sutures after being knotted.
Purpose:
To compare the loop security and knot strength of a standard round-braided suture with 3 commercially available flat-braided suture tapes using 2 types of arthroscopic knots.
Study Design:
Controlled laboratory study.
Methods:
One standard suture (SS) and 3 suture tapes (T1, T2, and T3) were tied with the surgeon’s knot (SK) and the Tennessee slider (TS), 25 times each, by a single surgeon. Each combination of knots and sutures underwent a preload, cyclic loading, and load to failure. Outcomes were loop security (defined by loop stretch after a 5-N preload), load at clinical failure (3 mm of displacement), and load at ultimate failure (suture rupture or knot slippage). Two-way analysis of variance was used for analysis.
Results:
Overall, the SK group had greater overall loop security than that of the TS group (0.4 ± 0.3 vs 0.5 ± 0.3 mm of stretch, respectively; P = .020). The clinical failure load varied by suture type (P < .001) but not knot type (P = .106). For both knot types, the SS had the lowest mean ± SD clinical failure load (SK, 171 ± 49 N; TS, 176 ± 37 N), which was significantly less than that of T2 (247 ± 85 N; P < .001) and T3 (251 ± 96 N; P < .001) for the SK type and T2 (231 ± 67 N; P = .023) for the TS type. T2 sutures had the greatest ultimate failure load for both knot types (SK, 418 ± 45 N; TS, 461 ± 57 N), which was significantly greater than SS, T1, and T3 (P < .001 for all). The TS knot had greater overall ultimate failure load than the SK (375 ± 64 vs 350 ± 66 N; P < .001).
Conclusion:
Not all suture tape knots had the same biomechanical properties, although knot security and strength appeared to be adequate for all suture tapes as well as for SS. There was no evidence that suture tape knots are lower profile than SS knots.
Clinical Relevance:
Surgeons should not use suture tape based only on the assumption that it has superior biomechanical properties to a standard round-braided suture.
Keywords
Advances in orthopaedic implant design are not limited to materials such as metal and polyethylene but are fully encompassing. One such innovation relates to suture and the development of flat-braided suture tapes for use during soft tissue repair. Suture tapes have been developed as a stronger lower-profile alternative to standard round-braided suture. Biomechanical data have shown that suture tape has an improved ability to compress a tendon to bone and is less likely to pull through tendon fibers. 8,14 These properties are thought to improve tendon healing, and tapes have become popular for use in procedures such as rotator cuff repair. 8,11 As a result, the commercial availability of suture tapes has expanded rapidly with a marketing focus on specific design properties, such as suture tape handling, increased strength with decreased bulk, and ability to be knotted.
Although knotless techniques using suture tape for tendon repair are available, there is evidence to support the use of combining knot tying with tape during procedures such as arthroscopic rotator cuff repair. 11,13 While it has been shown that the tensile strength of tape itself is greater than that of standard suture (SS), little is known regarding tape knot strength and security. In general, arthroscopic knot tying is technically challenging; it requires education and repetition to create a reproducible effective technique. Furthermore, studies have shown that not all knot-tying techniques are equivalent in clinical or biomechanical failure. 9,16 Given the innumerable combinations of knot techniques coupled with the variety of suture materials available, uncertainty exists regarding the ideal combination that maximizes knot security. 9
To date, there are few investigations into the biomechanical performance of these novel suture tapes after being knotted. The primary purpose of this study was to compare the loop security and knot strength of a round-braided SS with 3 flat-braided suture tapes (T1, T2, and T3) across 2 types of arthroscopic knots. We hypothesized that there would be no significant difference in knot strength or loop security among suture types or knot types. The secondary purpose was to compare the size of the knot stack across suture types. We hypothesized that suture tape's knot stacks would be smaller than those of SS.
Methods
Study Design
For this study, a standard No. 2 braided nonabsorbable suture (Arthrex FiberWire) was compared with 3 suture tape groups (T1, Arthrex FiberTape; T2, Smith & Nephew UltraTape; T3, Zimmer-Biomet Broadband) for loop security and knot strength as well as knot profile utilizing an arthroscopic surgeon’s knot (SK) 9 and a Tennessee slider (TS) knot, 4,6,9,15,16 followed by 2 half hitches (Figure 1). These are 2 knot configurations commonly used at our institution. This resulted in 8 testing groups, as shown in Table 1. For each knot and suture combination, we tested 25 samples for a total of 200 suture knots.
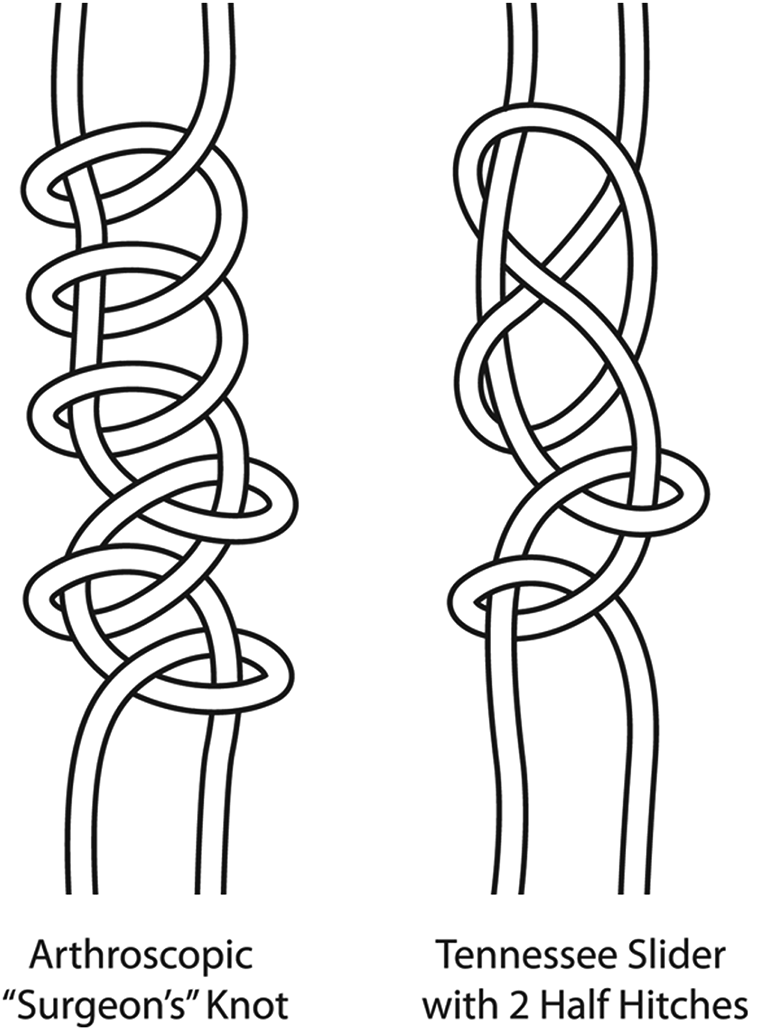
The arthroscopic surgeon’s knot (left) and Tennessee slider knot with 2 half hitches (right).
Testing Groups a

a For each group, n = 25.
Knot Preparation
All knots were tied by 1 fellowship-trained orthopaedic surgeon (C.M.R.) with experience in arthroscopic knot tying. The sutures were tied using an arthroscopic technique with an 8.5-mm arthroscopic cannula and knot pusher (FAST Arthroscopy Work Station, SKU 1711; Sawbones) (Figure 2) using either an SK or TS followed by 2 half hitches.
The sutures were tied around a 10-mm–diameter post to create a consistently sized suture loop. To ensure security in the knot and loop, steps were taken while tying, such as locking, removing twists and slack, and tensioning the suture limbs between the throws. 6,9 The tied sutures were presoaked in a normal saline bath for at least 5 minutes before testing.

The FAST arthroscopy training system used to tie sutures for this study.
Mechanical Testing and Data Collection
After the saline bath, the height and width of the knot were sequentially measured 3 times each by an engineer, using digital calipers (resolution, 0.0005 inches; CD-6-inch CSX Absolute Digimatic Caliper [Mitutoyo]). Width was measured as the widest part across the knot, and height was the tallest portion from top to bottom. The 3 measurements were averaged and recorded for the knot height and width. The suture was then mounted to a materials testing frame (MTS Insight 5) by placing the loop around 2 parallel steel dowel rods, with the knot positioned centrally between the rods (Figure 3). Using a custom fixture, the lower rod was fixated to the bottom of the test frame, and the upper rod was attached to the actuator.

Test frame with the suture loop placed around dowel pins and submerged in a saline-filled environmental test chamber. The upper rod was attached to the actuator.
A custom environmental test chamber was utilized for testing to allow the sutures to remain submerged in saline throughout the entire test to simulate an in vivo environment (Figure 3). The saline bath was at room temperature. Sutures were subjected to a mechanical testing protocol, which was developed according to previous literature. 2,10,16 Time, load, and crosshead displacement were all recorded by the test frame software at 100 Hz, and the data were processed using a custom data analysis program (MATLAB; MathWorks).
First, the loop security was determined by preloading the suture to 5 N for 5 seconds, as previously described. 16 The crosshead displacement during this test was recorded and used to calculate the change in circumference in the loop. 1,2,4 –6,9,10,15,17 Loop security was reported as the amount of loop stretch in millimeters at the end of the preload, with less stretch indicating a more secure loop.
After the preload, the suture was then subjected to cyclic loading with 1000 sinusoidal cycles from 5 to 45 N at a frequency of 1 Hz. These cyclic parameters have been reported to represent the repetitive loads that a patient would experience during rehabilitation after a rotator cuff repair. 16,18 After the cyclic testing was completed, the sutures were loaded to failure at a constant rate of 0.5 mm/s.
Data from the load-to-failure test were used to calculate the clinical failure load and ultimate failure load. Clinical failure load was defined as the force applied when the crosshead was displaced to 3 mm relative to the original starting point, based on the determination that a 3-mm gap between the tendon and bone can lead to failure of tendon-to-bone healing. 1,2,4 –6,9,10,12,16 Ultimate failure load was the maximum force applied to the knot during mechanical testing, which occurred either when the suture ruptured completely or when the knot began to slip. The failure mechanism (suture rupture or knot slippage) was observed and recorded during testing. If a knot failed during cyclic testing, its clinical failure and ultimate failure loads were derived from the cyclic test instead of the load to failure.
Statistical Analysis
An a priori sample size analysis was conducted, and it was determined that 25 samples of each knot and suture combination were required to ensure 80% power, an alpha of 0.05, and an effect size of 0.275. Testing data were assessed for normality. Continuous variables (knot height and width, loop security, and clinical and ultimate failure loads) were compared using a 2-way analysis of variance, with the 2 factors being knot type and suture type. A post hoc Sidak test was used for significant factors. A chi-square test was used to compare groups based on failure mode. For all tests, significance was defined as P < .05. Statistical analyses were performed using SPSS (Version 22.0; IBM).
Results
Knot Profile
The knot height varied significantly by suture type and knot type (P < .001 for both). The TS knot had a lower height overall (mean ± SD, 4.3 ± 0.6 mm) than the SK (5.2 ± 0.7 mm). Within the TS group, T2 had the greatest knot height, which was significantly higher than SS (P < .001), T1 (P < .001), and T3 (P = .003) (Table 2). Within the SK group, SS and T2 had greater height than T1 (P = .009 and P < .001, respectively) and T3 (P = .001 and P < .001).
Knot Height and Width Based on Suture and Knot Type

The knot width varied only by suture type (P < .001); no difference was observed in knot width based on knot type (P = .813). For the TS knot, SS and T2 were significantly wider than T1 (P = .013 and P < .001, respectively) and T3 (P = .017 and P < .001) (Table 2). For the SK knot, T2 had the greatest width by 0.2 mm and was significantly greater than T1 (P < .001) and T3 (P = .010). SS did not vary significantly from any tape when using the SK.
Loop Security
Loop security, measured by the amount of stretch in the knot during a 5-second 5-N preload, did not vary by the association between suture type and knot type (P = .718). Loop security was not significantly different according to suture type (P = .123) but was significantly different by knot type (P = .021). Overall, the SK knot had greater loop security (ie, less overall stretch) during the preload (0.4 ± 0.3 vs 0.5 ± 0.3 mm) (Figure 4).

Loop security (ie, stretch during preload) varied significantly by knot type, with the surgeon’s knot having overall less stretch and therefore greater loop security (P = .021). Suture type had no significant effect on loop security (P = .123). Values are presented as mean ± SD.
Clinical and Ultimate Failure Loads
The clinical failure load (ie, the load at 3 mm of displacement) showed no statistically significant interaction between knot and suture type (P = .561). The clinical failure load varied significantly by suture type (P < .001) but not knot type (P = .106). Within the SK group, T2 and T3 had a significantly greater clinical load to failure than the SS (P < .001 and P < .001, respectively) (Table 3). In the TS group, T2 had significantly greater clinical load to failure than the SS (P = .023). For both knot types, there was no difference in clinical failure load between any of the suture tapes.
Clinical and Ultimate Failure Loads Based on Suture and Knot Type

The ultimate failure load showed no statistically significant association between knot and suture (P = .071) but varied significantly by suture type (P < .001) and knot type (P < .001). For suture type, T2 had the greatest ultimate failure load for both knot types; within both knot types, it had a significantly higher failure load than the SS (P < .001), T1 (P < .001), and T3 (P < .001) (Table 3). The ultimate failure load for the SS did not vary from that of T1 or T3. Overall, the TS knot had a greater ultimate failure load (375 ± 64 vs 350 ± 66 N).
Failure Modes
In the SK group, only T1 had a failure by complete rupture during cyclic loading, which occurred in 2 instances (8% of group) (Table 4). For these 2 cases, the exact clinical and ultimate failure loads were derived from the cyclic test. In the SK group, each SS failed by suture breakage but did not have knot slippage like in the T2 and T3 groups. There was no significant difference between suture type and failure type when using the SK (P = .071) or the TS (P = .546).
Percentage of Failure Mechanisms Based on Suture Type Within Each Knot Type a

a Data are reported as % (No.).
Discussion
Suture knots used for arthroscopic procedures must have adequate strength to avoid rupture and ensure tissue approximation. In this study, we sought to independently investigate claims that flat-braided suture tape knots are stronger and lower profile than knots using a standard round-braided suture. We found that not all suture tape knots were stronger than an SS knot. Loop security under a small preload did not vary by suture type. The clinical failure load did vary according to suture type, with 2 of the 3 suture tapes (T2 and T3) being stronger than the SS when using the SK knot and with 1 tape (T2) being stronger than the SS when using a TS knot. Only 1 tape (T2) had a significantly greater ultimate failure load than the SS, which was seen for both knot types. T2 also had a greater ultimate failure load than the other 2 tapes.
The testing protocol in this study was based on those established in previously published studies. 2,10,16 Loop security represents the ability of the knot to maintain its integrity as it is tied. While loop security did not vary by suture type in our study, it did vary per knot type, with the SK groups having statistically less stretch during the preload than the TS groups by a mean of 0.1 mm. However, it is likely that such a slight difference would not make a clinical impact on the security of the knots. The knots were then tested under cyclic loading, which is designed to represent loads undergone during rehabilitation. 16,18 Two T1 knots from the SK group failed in this phase of testing, indicating that the suture knot could have failed early, during rehabilitative exercises.
The clinical failure is based on the determination that a 3-mm gap between the tendon and bone can lead to failure of tendon-to-bone healing, which has been widely used in previous studies. 1,16 While the SS had the lowest mean clinical failure load, the loads needed for failure were still high, with a mean of approximately 170 N, which is much greater than the physiological loads expected on an individual knot; according to calculations by Riboh et al, 16 the load on each knot is approximately 60 N. A recent study by Leishman and Chudik 7 also compared suture tape with round-braided suture using only an SK and Arthrex FiberWire and SutureTape (SS vs T1 in this study). They found no difference in load at 3 mm of displacement, which is consistent with our study—only T2 and T3 were significantly stronger than the SS.
Ultimate failure in most cases represents a traumatic tear. The TS knot had consistently greater ultimate strength than the SK, and T2 was overall the strongest suture, with no differences detected among the SS, T1, and T3. However, failure attributed to trauma is less common than failure from subfailure loading over time; therefore, it is arguable that all sutures had adequate ultimate failure strength. In the study by Leishman and Chudik, 7 they found the SS to have a lower load to failure than the suture tape. The load to failure for the SS in their study was lower than that in our study (mean, 257 vs 331 N). This could be because of differences in loading rates or subtle differences in knot-tying technique. In our study, knots were hand tied by 1 surgeon for consistency, but previous studies have shown that methods and knot strength vary surgeon to surgeon.
Most failures occur by the suture pulling out of the tendon rather than by the suture rupturing. 3 It was not possible to test suture pull-through strength within the scope of our study. However, with clinical and ultimate failure loads being adequate for all groups, this is one way that suture tape could be advantageous, given its broad compression as compared with standard braided suture.
In addition to differences in security and strength, we secondarily wanted to assess the knot profile by knot and suture types, since it is commonly thought that suture tape has a lower profile. The knot is a foreign body within the joint and has the potential to cause inflammatory reactions or mechanical impingement; therefore, a larger knot may be detrimental to outcomes. 7 To assess the knot profile, we measured the height and width of all suture and knot combinations. For both knot types, T2 had the greatest height. The SS had a greater height than T1 and T3 when using an SK. We also found that the knot type was more determinant of profile than the suture itself, with the SK having a greater overall knot height than the TS by about 1 mm. It is unknown whether these differences are clinically significant.
There are several limitations to this study, the first being that this is an in vitro biomechanical study and cannot account for the variability that occurs in vivo. To best simulate in vivo conditions, the knots in this study were tied through an arthroscopic cannula with a standard pusher and were bathed and tested in saline. However, the saline was not at body temperature. Furthermore, as with all biomechanical studies, these results represent failures only at the time of repair. As tendon healing occurs, the need for knot strength diminishes. Second, because of laboratory constraints, not all the knots were tested on the same day that they were tied. The differences in storage time may have slightly changed the properties of the sutures. Third, when calculating loop security, we assumed that the knots did not change circumference when transferred from the arthroscopic knot post to the test bench; however, a previous study 16 noted a slight contraction of the knots after their removal from the post. In addition, knot height and width were assessed with calipers; measurements would have been more accurate using microscopy. Finally, there are other potential advantages to suture tape that could not be evaluated in this study, such as whether the flatter profile of tape can improve tendon healing, reduce vascular restriction, and decrease the likelihood of suture pulling through tendon fibers.
Conclusion
Knot security and strength vary by knot type and suture type. Not all suture tape knots have the same biomechanical properties, although knot security and strength appear to be adequate for all suture tapes as well as for SS. Furthermore, there is no evidence that suture tape knots have a lower profile than SS knots.
Footnotes
Final revision submitted June 8, 2021; accepted June 16, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.M.R. has received education payments from Arthrex and hospitality payments from Integra LifeSciences, Smith & Nephew, and Wright Medical. J.K. has received education payments from Pinnacle and hospitality payments from Stryker and Zimmer-Biomet. B.W. has received education payments from Arthrex and hospitality payments from Encore Medical, Smith & Nephew, Stryker, TriMed, and Zimmer-Biomet. J.M.W. has received grants from DJO; education payments from Arthrex and Pinnacle; consulting fees from DePuy, Ignite Orthopedics, Lima, TechMah Medical, and Zimmer-Biomet; nonconsulting fees from Arthrex; royalties from Smith & Nephew. J.M.W. also has stock/stock options in Catalyst. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.