
Abstract
Background:
The merits of a double-row rotator cuff repair (RCR) construct are well-established for restoration of the footprint and lateral-row security. The theoretical benefit of leaving the medial row untied is to prevent damage to the rotator cuff by tissue strangulation, and the benefit of suture tape is a more even distribution of force across the repair site. These benefits, to our knowledge, have not been evaluated in the laboratory.
Hypothesis:
Leaving the medial row untied and using a suture bridge technique with suture tape will offer more even pressure distribution across the repair site without compromising total contact force.
Study Design:
Controlled laboratory study.
Methods:
A laboratory model of RCR was created using biomechanical research-grade composite humeri and human dermal allografts. The pressure distribution in a double-row suture bridge repair construct was analyzed using the following testing matrix: double-loaded suture anchors with the medial row tied (n = 15) versus untied (n = 15) compared with double-loaded suture tape and anchors with the medial row tied (n = 15) versus untied (n = 15). A digital pressure sensor was used to measure pressure over time after tensioning of the repair site. A multivariate analysis of variance was used for statistical analysis with post hoc testing.
Results:
The total contact force did not significantly differ between constructs. The contact force between double-loaded suture anchors and double-loaded suture tape and anchors was similar when tied (P = .15) and untied (P = .44). An untied medial row resulted in similar contact forces in both the double-loaded suture anchor (P = .16) and double-loaded suture tape and anchor (P = .25) constructs. Qualitative increases in focal contact pressure were seen when the medial row was tied.
Conclusion:
An untied medial row did not significantly affect the total contact force with double-loaded suture anchors and with double-loaded suture tape and anchors. Tying the medial row qualitatively increased crimping at the construct’s periphery, which may contribute to tissue strangulation and hinder clinical healing. Qualitative improvements in force distribution were seen with double-loaded suture tape and anchors.
Clinical Relevance:
Both tied and untied medial rows demonstrated similar pressures across the repair construct.
Rotator cuff repair (RCR) is one of the most common arthroscopic procedures performed in the United States. 8 Successful RCR depends on multiple aspects of the fixation method: tension-free (or minimal tension) repair, re-establishment of the anatomic footprint, and biologically friendly repair of the rotator cuff to its humeral footprint. 6 –8,12,14,22,28,44 Several smaller studies have compared the contact pressure of RCR between single-row, double-row, and transosseous techniques. 31,34,42 Park et al 31 determined that the transosseous suture technique was superior to the single-row simple suture anchor and single-row mattress suture anchor techniques with respect to tendon-to-bone contact distribution and contact pressure in a bovine model. A later study in cadaveric shoulders demonstrated that the contact pressure and area were significantly increased using a transosseous-equivalent technique compared with the double-row and suture bridge techniques. 34 Tuoheti et al 42 reported that the double-row technique demonstrated superior contact areas and the second highest contact pressures compared with the transosseous and single-row techniques. Ostrander and McKinney 29 have argued in favor of using triple-row repair to increase the footprint contact area and pressure by demonstrating its superiority over both single-row and double-row repair.
Preservation of the structural integrity of rotator cuff tissue during repair is becoming increasingly recognized. Avoiding knots in delicate tissue is thought to improve healing, especially in revision surgery, and this approach has demonstrated success. 20,35 Continued debate exists on the optimal repair method, and knotless approaches have not demonstrated superiority in some studies. 11,16,17,21,26 Nevertheless, there has been an increasing trend in the use of knotless repair techniques over the past decade. 37 In cadaveric and animal studies, knotless transosseous-equivalent repair demonstrated superior self-reinforcement (greater progression of footprint compression with increasing tendon loads) compared with medial knot repair. 33,38 In smaller tears (≤1.0 cm), single-row repair has demonstrated good success, but the suture pattern and anchor location influence tendon morphology and footprint re-creation. 28,30 Park et al 30 demonstrated better tendon morphology and maintenance of the footprint dimensions with distal lateral anchor placement and an inverted mattress stitch. Barber and Drew 3 compared double-row repair with suture tape versus triple-loaded single-row repair in a cadaveric study and found that double-row repair with suture tape was biomechanically superior by minimizing footprint motion while maximizing footprint coverage. Using traditional sutures, these authors previously demonstrated that triple-loaded single-row repair was superior to double-row repair. 4 When considered in aggregate, an improved footprint contact area with distributed force pressures would theoretically yield a more biologically friendly environment for tissue healing.
The purpose of our study was to assess the contact area and pressure with double-row suture bridge repair constructs comparing the traditional knot-tying suture technique and a knotless technique. We also sought to evaluate contact pressure differences between traditional suture and suture tape constructs. We hypothesized that the maximal contact area and even distribution of contact pressure would be best achieved using the double-row transosseous-equivalent technique with the medial row untied using suture tape.
Methods
Experimental Design
A standardized RCR model was created using biomechanical research-grade humeri (Sawbones). These were chosen because of uniformity compared with cadaveric specimens, which may differ in bone and tissue quality. Preparation of the Sawbone models was performed by an orthopaedic surgery resident (A.V.S., T.D.L.) under the supervision of double fellowship–trained sports medicine and shoulder/elbow orthopaedic faculty (M.T.F.). The humerus was clamped at 0° of flexion, abduction, and external rotation as outlined by Park et al 31 and was anchored to a fixed table (Figure 1). Medial-row anchor holes were predrilled along the articular margin in the supraspinatus footprint with a standard template. Medial-row anchors were then placed using either double-loaded suture anchors or double-loaded suture tape and anchors (5.5-mm PEEK Healicoil; Smith & Nephew). The lateral row was drilled bicortically along the greater tuberosity and medially through the surgical neck. An acellular human dermis allograft (Matrix HD; RTI Surgical) served as the rotator cuff graft that was fixed to the humerus model. The graft was attached medially to a clamp that was connected to a tension sensor and force transducer. The 11 × 11–mm pressure sensor (Tekscan) was placed under the graft tissue within the boundaries of the 4 suture anchors and attached to a transducer. The lateral-row sutures were pulled through the surgical neck of the humerus model medially and attached to a tensioner. To ensure consistent lateral-row fixation during all trials, an examiner (A.V.S.) maintained a constant tension of 8 N (∼1.8 pound-force) for 5 seconds. The contact force over the footprint during this time frame was measured. Contact pressure was calculated as the contact force divided by the surface area of the pressure sensor. A total of 4 groups were used to assess the pressure distribution using the following testing variables: double-loaded suture anchors with the medial row tied (n = 15) versus untied (n = 15) and double-loaded suture tape and anchors (1 tape and 1 suture) with the medial row tied (n = 15) versus untied (n = 15).

Demonstration of the testing apparatus with the sutures passed and secured.
Statistical Analysis
A power calculation was completed based on previously published mean pressures. 31,34,42 Park et al 31 previously reported that the mean contact pressure in their cadaveric model using transosseous repair was 0.32 ± 0.05 MPa, which was significantly different from RCR using simple suture anchors (0.26 ± 0.04 MPa) or mattress suture anchors (0.24 ± 0.02 MPa). To detect a difference of 0.05 MPa of contact pressure with β = 0.8 and α = 0.05, a minimum of 9 per group was required. Data analysis was performed using 2-way analysis of variance with appropriate post hoc tests as indicated. Significance was set at P ≤ .05. The center of pressure (COP) was calculated using the following equations:


where x is the x-coordinate, y is the y-coordinate, F is force, d is the distance from the origin (dx is along the x-axis, and dy is along the y-axis), and n is the number of sensel measurements.
Results
The contact force did not significantly differ between constructs (Figure 2). The contact force between double-loaded suture anchors and double-loaded suture tape and anchors was similar in both the tied (P = .15) and untied (P = .44) conditions. An untied medial row resulted in similar contact forces in both the double-loaded suture construct (P = .16) and the double-loaded suture and tape construct (P = .25), although qualitatively, focal increases in contact pressure were seen when the medial row was tied (10-15 pound-force per square inch) (Figure 3).
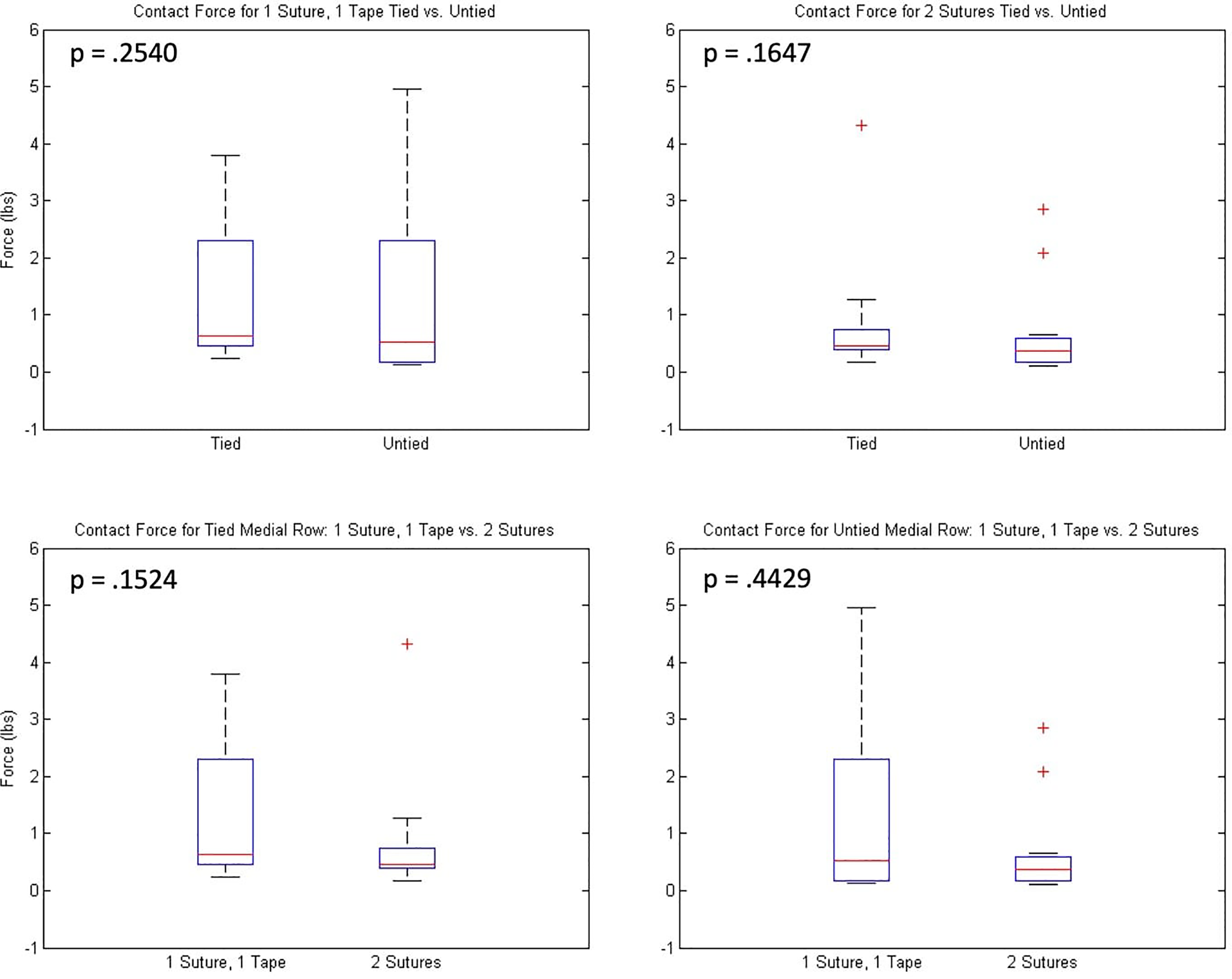
Box and whisker plots of total contact force with tied and untied medial-row constructs. The red line in the box indicates the mean, the top and bottom of the box indicate interquartile range, the error bars represent 95% CIs, and the “+” sign indicates outliers.

Pressure maps of double-loaded suture anchors with the medial row tied and untied (top row) and double-loaded suture tape and anchors with the medial row tied and untied (bottom row). The top edge of each figure represents the medial row, whereas the bottom row represents the lateral row. Pressure is seen with the scale to the right of each map and is reported as pound-force per square inch (psi). A gradient of colors from blue to yellow represent the psi values recorded by the sensor, with blue and green colors being favorable. Evenly distributed pressure is demonstrated with a predominance of blue to light blue, with yellow indicating focally greater pressure.
Additionally, graft “crimping” was qualitatively identified in the constructs with tied medial rows (Figure 4). Crimping was defined as excessive compression at the suture sites with narrowing of the width of the graft.

Comparison of tied versus untied transosseous-equivalent constructs. (A) Representative image demonstrating a tied medial row with tape and suture and crimping at the medial knot sites (arrowheads). Mild crimping is also noted at the lateral footprint (arrows) in both constructs as the tape and suture construct is being pulled under tension. (B) Demonstration of an untied medial row with tape and suture with less medial-row crimping and lateral-row suture distribution.
No statistically significant difference was identified in the center of pressure measurements between tied and untied graft constructs and those with and without suture tape, signifying that pressure was distributed similarly over the entire graft and footprint in the 4 different constructs (Figure 5).
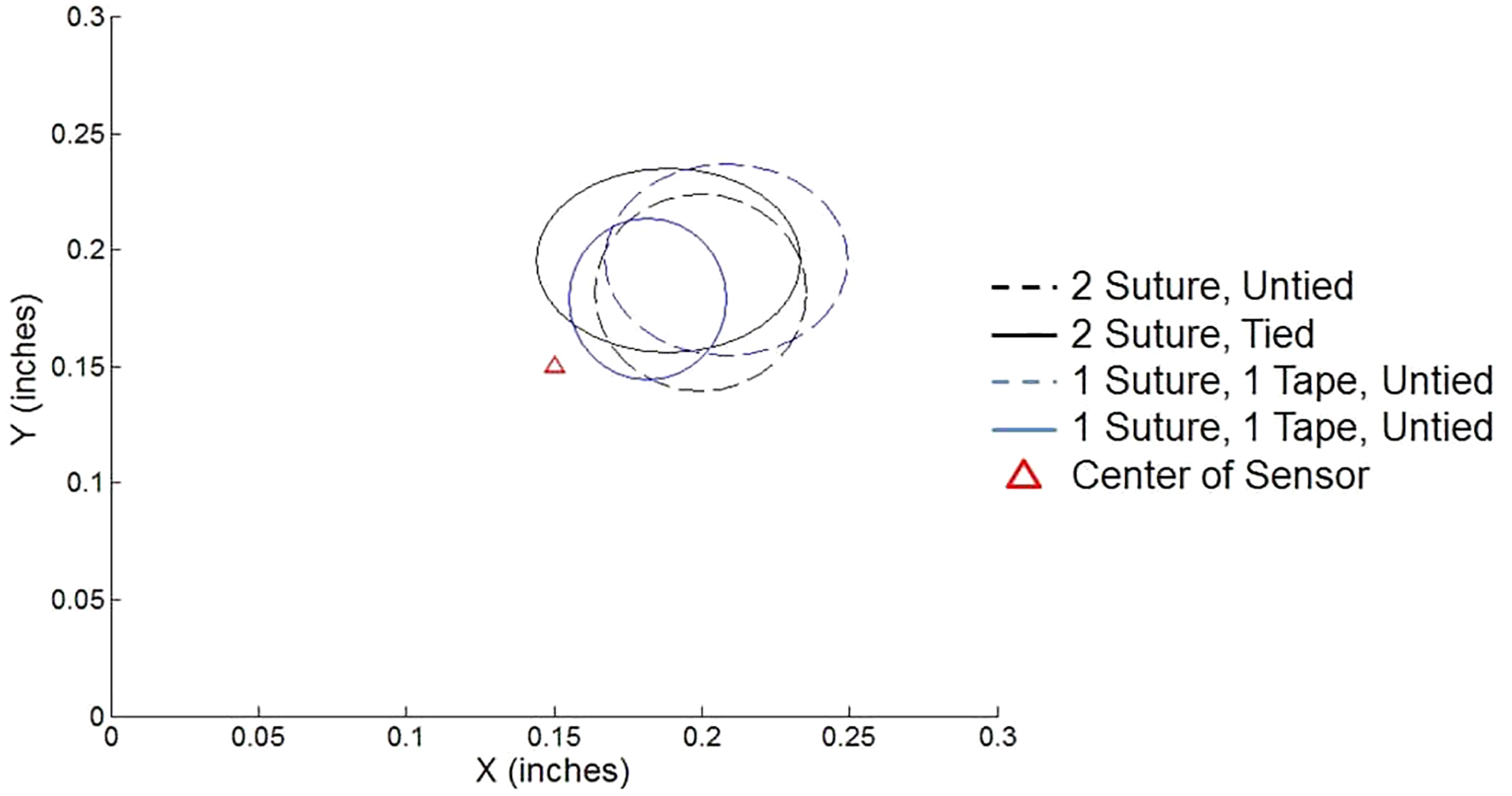
Center of pressure distribution showing a substantial amount of overlap between the 4 constructs.
Discussion
The principal finding of our study was that an untied medial row did not significantly differ in overall contact force or pressure when compared with a tied medial row. Qualitatively, tying the medial row increased focal contact pressure and crimping at the construct’s periphery; however, the amount of crimping was not quantitatively assessed. No pressure difference or force distribution existed between double-loaded suture anchors and double-loaded suture tape and anchors. The goal of this study was to establish that a knotless medial row is at least as good in maintaining and distributing contact pressure as the traditionally tied medial row. Our results support the hypothesis that an untied medial row does not reduce the total contact force in a double-row RCR construct.
Our model offers several advantages over conventional studies. While other authors have looked at re-establishment of the rotator cuff footprint, those who have focused on pressure distribution have relied on less accurate methods of pressure acquisition, such as pressure-sensitive film. 31,32,42 Electronic pressure measurements can not only assess pressure in real time, but they may also determine the maximal pressure during knot tying in addition to detecting endpoint pressure after all anchors have been placed and knots tied. The use of pressure-sensitive film only identifies the maximal pressure, which would not detect the potential decrease in pressure after all knots are tied and the footprint is re-established.
We also sought to eliminate any variability in materials or the testing design to isolate the effects of the suture construct. Controlled variables included biomechanically identical research-grade Sawbones, clinically approved and homogeneous graft material, consistent anchor and suture placement, and controlled graft and suture knot tension, which were verified throughout the data acquisition process. With this measured approach, we were better able to quantify subtle differences in suture construct pressure at the tissue-bone interface.
The primary goal of RCR is to maximize the healing potential by restoring the anatomic footprint; our study aimed to provide evidence for a repair construct that is considered biologically favorable. Failure of RCR has been well-documented in biomechanical and clinical studies, along with the mechanisms of failure. In arthroscopic repair, the 4 most common sites of failure include the knot, suture-tendon interface, 1,9,23 anchor-suture interface, 5,10 and bone-anchor interface. 2,25 Excess tension on tissue, damage to the rotator cuff induced by braided suture, and overloading at the suture-tendon interface have specifically been implicated in failure of medial-row repair. 11,13,17,43 The suture bridge technique is well-established as improving contact area and force compared with a traditional double-row construct. 34 The knotless suture bridge technique was reported by Hug et al 15 to be equivalent to the medial-row knot-tying technique in terms of clinical and radiographic outcomes. These authors found that the likelihood of gap formation was greater with “perforation” with an untied medial row but argued in favor of a more biologically friendly suture construct that could theoretically reduce medial musculotendinous junction failure. 15 Our study did not demonstrate evidence that an untied medial row reduced contact pressure in the RCR model.
The preservation of medial rotator cuff tissue integrity was supported by a lower retear rate with knotless constructs (5.9%) compared with a traditional knot-tying suture bridge technique (18.6%) in a retrospective comparison study by Rhee et al. 35 Furthermore, these authors found that the majority of retears occurred at the musculotendinous junction. Medial-row failure attributed to the knot has been reported in both biomechanical models and clinical studies. 27,35,40,46 In an in vitro study published in 2019, Sun et al 39 identified that nonabsorbable suture knots migrate to the articular side of the tear in a rat model. Migration caused chronic inflammation and weakening of the tendon and bone healing, which the authors proposed is a potential mechanism of repair failure. 39 Our finding of similar contact pressures may support the use of a knotless medial row in an effort to avoid the aforementioned failures, at least as it relates to adequate tissue contact pressure.
In double-row transosseous-equivalent repair, the medial row functions as a tension-bearing row, which concentrates stress during recovery and is theorized to lead to medial-row failure. 11,41,45,46 A cadaveric biomechanical study demonstrated that the tied medial row of double-row repair failed first during cyclic loading. 27,36 The force concentration from a tied medial row is further suggested by low stress seen at the lateral-row interface. 36 A cadaveric study using a modified Mason-Allen technique further demonstrated greater mean contact area and interface pressure specifically at the medial row when the medial row was tied compared with knotless medial-row transosseous-equivalent repair. 18 During the knot-sliding process in arthroscopic repair, overtensioning of knots can further introduce small tears into soft tissue and generate a high concentration of stress, especially on the medial row. 36 Furthermore, braided suture has been reported to have higher abrasive properties through rotator cuff tissue when compared with monofilament sutures. 19 Suture tape, however, has demonstrated a greater mean load to failure and greater contact area at the suture-tendon interface, facilitating even pressure distribution. 43 These reports in aggregate suggest that tying of the medial row with suture, combined with the inherently reduced vascular supply of transosseous-equivalent repair, may risk tissue strangulation. Ultimately, this approach can compromise the ability of the repair construct to generate the appropriate biological environment necessary for long-term tendon-to-bone healing.
Conversely, gap formation after cyclic loading is decreased with knotted suture bridge constructs compared with knotless constructs. 24 One explanation is that tying the medial row provides an anchor point to prevent tissue liftoff when abducting the humerus. While we anticipated seeing a significant difference in focal contact pressures between suture and suture tape, our study did not identify any difference in the pressure distribution along the tape path in the repair construct. Despite using a highly sensitive measurement device, the ability to resolve a millimeter difference in contact area across a 3 mm–thick graft was not possible. We conclude that if the suture tape construct is not inferior, and there is evidence to support suture tape as a biologically friendly construct, then the use of suture tape in repair could be encouraged.
Limitations
The present study does carry the common limitations of laboratory models. The human dermal allograft tissue in our study was neither diseased nor vascularized and has different mechanical properties from rotator cuff tendons. The allograft tissue also precludes the evaluation of vascularization and biological friendliness between each of the techniques. The shoulder models used were synthetic rather than cadaveric. Human tissue, especially a diseased rotator cuff, may respond differently to suture materials, which prompts further investigation in cadaveric and clinical studies. Furthermore, the amount of crimping that was qualitatively assessed may not reflect how diseased rotator cuff tissue behaves in vivo. The grafts were also not attached anteriorly and posteriorly, which may have contributed to extra crimping. Depending on surgeon technique and preference, lateral-row anchors will have a wide range of tension clinically, and our data may not be applicable to personal preferences in lateral-row tension. Additionally, our study examined time-zero findings. Without evaluating the effects of cyclic loading and load to failure, we were unable to assess for gap formation or tissue liftoff between tied and untied constructs or loosening of knots and sutures over time, as one may expect in the human shoulder. We advocate, however, that despite these limitations, our study was carefully designed to examine suture constructs and adds valuable biomechanical data to the literature.
Conclusion
The specific RCR construct did not significantly change the contact force when the medial row was tied versus untied or when only suture and not suture tape was used. Qualitative analysis demonstrated increased focal pressure along the periphery of the footprint when the medial row was tied as well as greater “crimping” of the graft tissue. While the biological impact of these findings is not explored in this study, we have identified that an untied medial row was not inferior to a tied medial row with respect to contact force.
Footnotes
Final revision submitted December 12, 2019; accepted January 10, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a research grant from Smith & Nephew. The Matrix HD human acellular allograft was donated by RTI Surgical. A.V.S. has received research support from Arthrex and Smith & Nephew; educational support from Arthrex, Smith & Nephew, and Medwest; and hospitality payments from Stryker and Wright Medical. M.T.F. has received research support from DJO, Regeneration Technologies, and Smith & Nephew and consulting fees and speaking fees from Integra and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.