
Abstract
Purpose:
The objective of the study is to determine clinical and radiological outcomes of arthroscopic repair for delaminated tears versus non-delaminated tears.
Methods:
Consecutive 138 patients with full-thickness rotator cuff tear were retrospectively enrolled. They were divided into two groups based on the presence of delamination. All delaminated tears were repaired by en bloc technique (suturing both layers by single stitch). Delaminated tears were categorized into two types: (1) posterior type, delamination involving mainly infraspinatus and (2) complete type, delamination involving both supraspinatus and infraspinatus. Clinical assessments were done using pain visual analog scale (PVAS), functional VAS, American Shoulder Elbow Surgeons score, the Constant score, and range of motion. Postoperative MRI was performed at 6 months after surgery to determine repair integrity.
Results:
Of the 138 patients, 78 (56.5%) had delaminated tears, including 30 cases of posterior type and 48 cases of complete type. The retear rate was 6.7% (4/60) in the non-delamination group and 5.1% (4/78) in the delamination group, showing no significant difference between the two groups. There was no significant difference in Sugaya classification between the two groups. Clinical scores were improved significantly in both delamination and non-delamination groups postoperatively, showing no significant difference between the two groups. Delamination subgroup (posterior or complete type) showed no significant correlation with retear rate, Sugaya classification, or clinical outcome.
Conclusions:
Arthroscopic en bloc repair for delaminated rotator cuff tear showed no significant difference in clinical or radiological outcome from that for non-delaminated rotator cuff tear. The extent of delamination did not affect outcome either. Levels of Evidence: Level III, Retrospective comparative study.
Introduction
Arthroscopic rotator cuff repair has been reported to be successful, regardless of the tear size. 1 –5 Delaminated tear is a common finding in rotator cuff repair, with incidence ranging from 38% to 92%. 6 –10 Delaminated tear is thought to occur from intra-tendinous shear force between articular-sided and bursal-sided supraspinatus and infraspinatus tendon. 11 –13 Sonnabend et al. 14 demonstrated that there was a layer of synovial-like cells in the delaminated cuff. Boileau et al. 6 have reported that delaminated tear of subscapularis and infraspinatus is negatively associated with tendon healing. Flurin et al. 7 have shown that delamination is a negative prognostic factor in arthroscopic rotator cuff repair. However, several recent studies have shown that the presence of delamination does not affect the outcome of arthroscopic repair for massive rotator cuff tear 15 or mini-open repair. 16 Therefore, clinical evidence regarding the influence of delamination on arthroscopic rotator cuff tear is contradictory.
There are two popular surgical techniques for delaminated rotator cuff. The first is suturing each laminated layer separately, attaching the inner layer to the medial footprint while attaching the outer layer to the lateral footprint. 5 The other technique, so called “En bloc”, involves suturing both delaminated cuffs with a single stitch. 15 A recent study 17 has shown that there is no significant difference between separate repair and en bloc repair in delaminated tear. However, whether this delamination has negative effects on the outcome compared to non-delaminated tears is unclear.
Therefore, the purpose of this study was to compare clinical outcomes between delaminated tears and non-delaminated tears using en bloc repair technique. We hypothesized that delaminated rotator cuff tears would produce inferior results compared to non-delaminated cuff tears and that larger extent of delamination would produce inferior results.
Materials and methods
Patient selection
Our Institutional Review Board approved this retrospective study and waived the requirement for informed patient consent (IRB file No. 2015-03-052-001). This was a retrospective, consecutive, non-randomized, comparative study. Patients who underwent arthroscopic rotator cuff repairs in our center from May 2011 to December 2012 were retrospectively enrolled. Inclusion criteria were: (1) full-thickness rotator cuff tear, (2) arthroscopic complete repair (type I or type II repairs 18 ), and (3) patients received follow-up MRI in our center at 6 months postoperatively. Exclusion criteria were: patients with partial-thickness tear and massive-sized tear (>5 cm), incomplete repair (type III or type IV repairs 18 ), revision rotator cuff tear, fracture-related cases, isolated subscapularis tear, inflammatory joint disorder (rheumatoid arthritis, gout), infection, or neoplasm. Massive tears were also excluded to avoid selection bias because most of these tears were repaired incompletely. Patients with follow-up less than 2 years were also excluded.
Rotator cuff tear was diagnosed by MRI and confirmed by intraoperative arthroscopic findings. Delamination was defined as horizontal tear occurring between layers of the rotator cuff. It was recognized by intraoperative arthroscopic findings. All patients were divided into two groups based on the presence of delamination in arthroscopic findings: delamination group and non-delamination group. Clinical and radiological results were compared between the two groups. The delamination group was subdivided into two groups based on the extent of delamination in video review: posterior type (delamination in infraspinatus only) and complete type (delamination in supraspinatus and infraspinatus). Clinical and radiological results were also compared between the two subgroups.
Surgical technique and postoperative rehabilitation
All surgical procedures were performed by a single surgeon. Under general anesthesia, the patient was placed in semi-lateral decubitus position with 30° posterior tilt. Evaluation of motion range was done and gentle manipulation was used when motion was limited. Posterior viewing portal was made and routine glenohumeral joint examination was done. After addressing glenohumeral joint pathology, an arthroscope was inserted into the subacromial space. Subacromial bursectomy was done and then acromioplasty was performed in cases showing evidence of impingement. Pathological tissue of the torn rotator cuff was debrided. Tear size was measured from anterior to posterior by introducing the probe via the posterior portal and from medial to lateral by introducing the probe via the lateral portal.
The presence of delamination and tear pattern were evaluated carefully from the lateral portal just prior to acromioplasty. Matsuki et al. 9 have reported that most delamination occurs posteriorly and proximally. Thus, we assessed rotator cuff tear by both the posterior viewing portal and the posterior lateral portal to identify the presence of delamination and further clarify its location. 8
In cases with delamination requiring repair, the tissue between the bursal and articular flaps was meticulously debrided with a shaver or curette. A suture hook was utilized to penetrate the bursal flap. The retracted articular flap was grasped, reduced, and then penetrated with the suture hook. The suture was then shuttled using a retrograde technique through both the articular and bursal flaps (en bloc technique; Figure 1). After the en bloc suture was performed on the delaminated rotator cuff, repair was performed similar to that performed for non-delaminated rotator cuff.

Arthroscopic images with 30° arthroscope depicting arthroscopic en bloc repair. This is a left shoulder in the lateral decubitus position. The right toward black arrow indicates posterior rotator cuff. Both bursal- and articular-sided delaminated cuffs were sutured with a single stitch.
Mobility and reparability were evaluated by pulling the tear-end to footprints with a grasper. All repairs were performed using the double-row trans-osseous equivalent technique. Decortication of footprint was done with a burr. Suture anchor was inserted just lateral to the cartilage margin (type I repair 18 ) or slightly medial to cartilage margin with decortication (type II repair 18 ). After tying mattress sutures individually, the lateral row of sutures was placed lateral to the footprint on the greater tuberosity of the humerus using tails of previously placed medial sutures.
Rehabilitation was performed similarly for all study subjects. Patients were immobilized for 5–6 weeks with a 30° abduction brace depending on the tear size (small/medium sized tears, 4–5 weeks; large tears, 6 weeks). During this period, patients were encouraged to perform active mobilization of hand, wrist, and elbow. After immobilization, passive range of motion (ROM) exercises were started. Subsequently, active ROM exercises were commenced after full passive ROM was acquired. Strengthening exercises with elastic bands were initiated at 2–3 months postoperatively.
Radiological assessment and arthroscopic video review
Patients underwent MRI at 6 months postoperatively to assess cuff healing. All MRIs were performed with a 3.0 T magnetic resonance imager (Gyroscan Interna Achieva, Best, the Netherlands). Oblique coronal, oblique sagittal, axial T2 weighted images and coronal proton density images were acquired. Two orthopedic fellows in training shoulder part reviewed MRI. Postoperative MRI was classified into five categories according to the criteria of Sugaya et al. 19 In the present study, MRI grades I to III were regarded as healed cuff while type VI and V were regarded as full-thickness retear.
Although the presence of delamination was prospectively recorded during surgery, video review was performed again to define the location of delamination. Two orthopedic shoulder fellows examined the arthroscopic operation on video (available for all patients) for each case. We classified delaminated tears into two subgroups according to the degree of delamination (posterior type, delamination localized in infraspinatus only; complete type, delamination presents as whole cuff including the supraspinatus and infraspinatus; Figure 2).

“Posterior type” and “complete type” delamination. These are right shoulders in the lateral decubitus position. The posterior type (a) shows delamination focalized in infraspinatus only, while the complete type (b) shows delamination in both supraspinatus and infraspinatus.
Two orthopedic shoulder fellows who were blinded to patient information, surgical findings, and clinical results reviewed postoperative MRI and arthroscopic records. Kappa coefficient (k) was used to determine interobserver variation in assessing radiological assessment and arthroscopic video review. For statistical analysis, results from one of the two shoulder fellows were used.
Clinical assessment
Clinical evaluations were performed the day before surgery and postoperatively at 6 months, 1 year, and at final follow-up (a minimum of 24 months after the postoperative period). Pain visual analog scale (PVAS), functional visual analog scale (FVAS), American Shoulder Elbow Surgeons scores (ASES), 20 and Constant scores 21 were used for assessment and results were compared. ROM was measured in forward elevation, abduction, external rotation at side, and internal rotation in vertebral level. For statistical analysis, we converted vertebral level to a number: T1–T12 to 1–12, L1–L5 to 13–17, sacrum to 18, and buttock to 19. Clinical evaluations were performed by a single physiotherapist who was unaware of this study.
Statistical analysis
To compare preoperative and postoperative continuous variables, paired t-test or Wilcoxon signed rank test was used depending on the normality of difference. To compare data between two groups, two-sample t-test was used for continuous variables while χ 2 test was performed for categorical variables. Fisher’s exact test was performed for low expected frequency. Linear by linear associations were performed for three or more categorical variables. All statistical analyses were performed with IBM SPSS statistics 20.0 software (IBM-SPSS, Armonk, New York, USA). The confidence interval was set at 95%.
Results
A total of 411 patients with rotator cuff tear were operated, of which 148 with partial-thickness and massive-sized tears were excluded. Of the remaining 263 cases, 189 (71.9%) patients who had postoperative MRI were included. Seven revision cases, five fracture-related cases, six isolated subscapularis tear cases, seven insufficient arthroscopic records cases, one associated Bankart repair case, one patch graft augmentation case, and 14 incomplete repair cases were excluded. Ten patients with follow-up less than 2 years were also excluded, leaving 138 cases eligible for inclusion in this study.
Delaminated rotator cuff was found in 78 (56.5%) cases. The incidence of delaminated rotator cuff was not affected by age, duration of symptom, underlying diabetes mellitus and thyroid disease, or preoperative tear size distribution. The proportion of women in the delamination group was higher (p = 0.048) than that in the non-delamination group. Delamination occurred more frequently in the dominant arm (p = 0.046). Type of repair, combined procedures (biceps tenotomy or tenodesis, subscapularis debridement or repair, capsular release, acromioplasty), and mean follow-up periods showed no significant differences between the two groups (Table 1). Posterior type and complete type of delamination had 30 and 48 cases, respectively. Kappa coefficient for interobserver variation in judging the type of delamination was 0.752.
Delamination group versus non-delamination group.
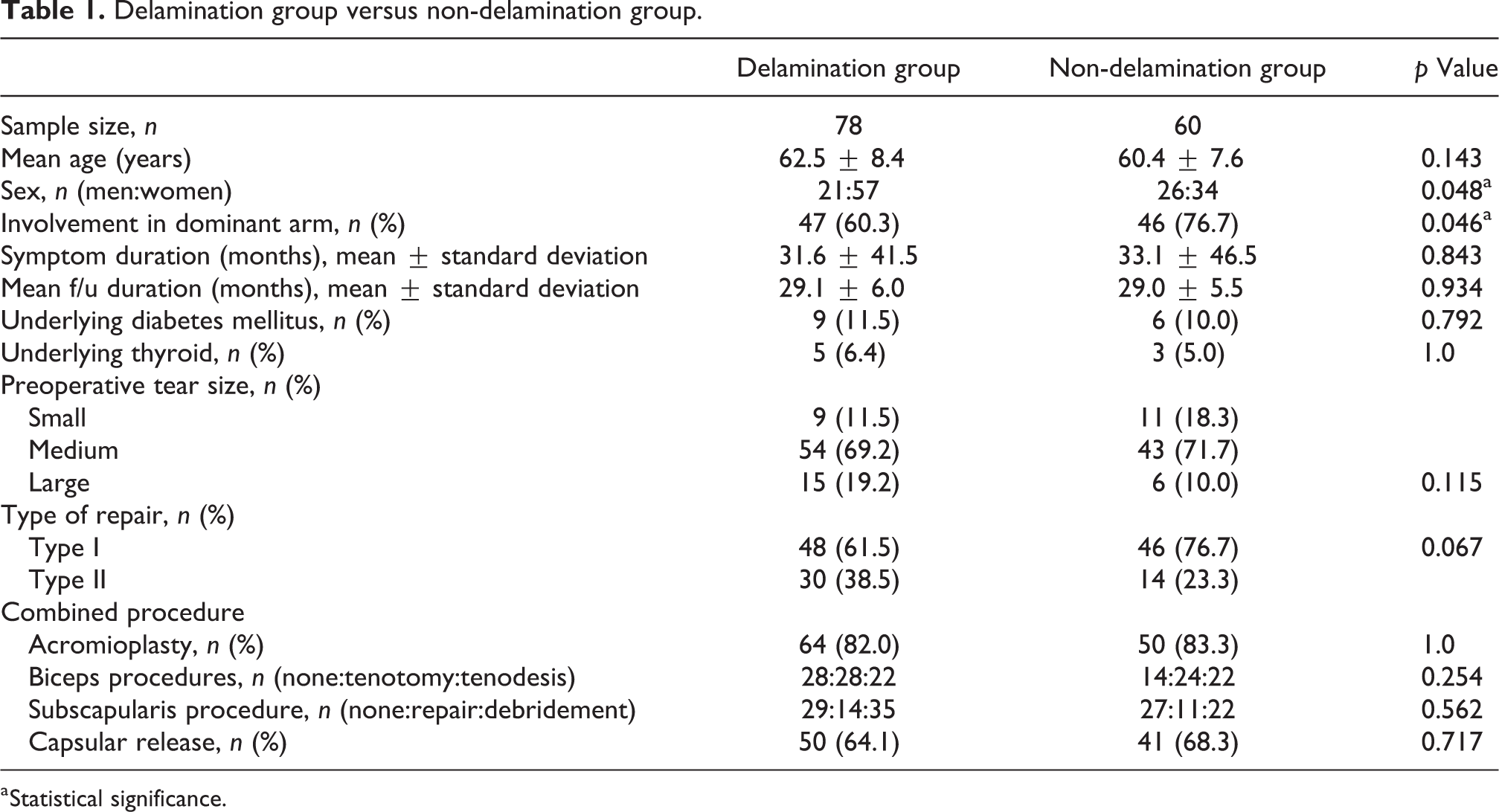
a Statistical significance.
Radiological results
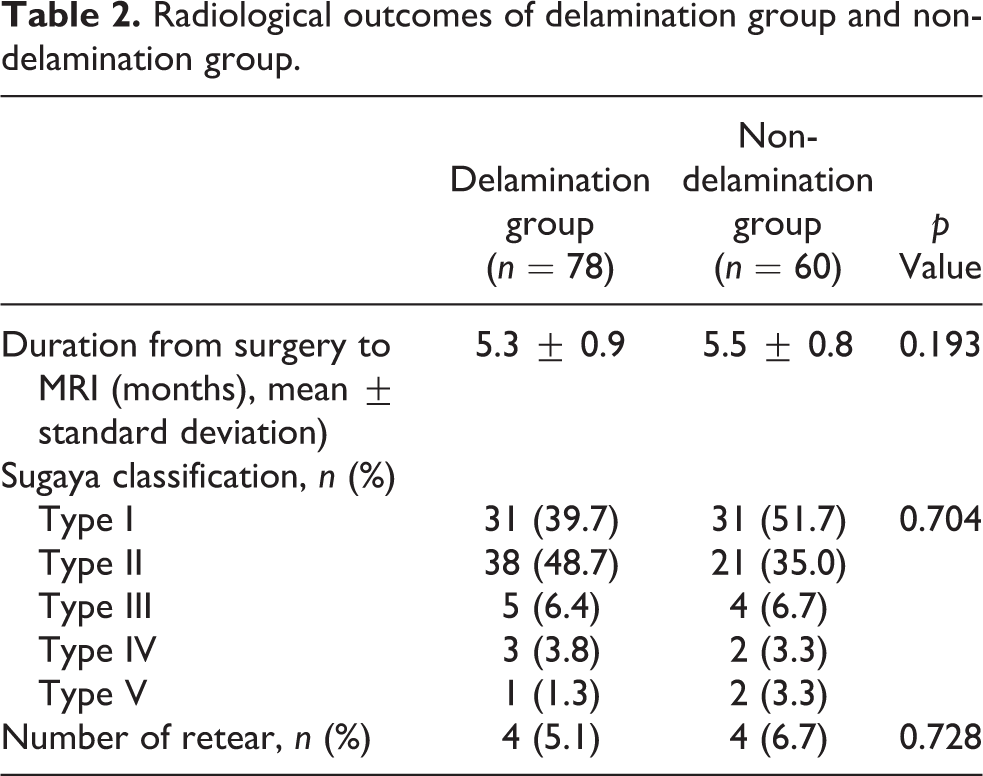
The kappa coefficient for interobserver variation in assessing full-thickness retear (Sugaya classification grades IV and V) was 0.882. The retear rate was 6.7% (4/60) in the non-delamination group and 5.1% (4/78) in the delamination group, showing no significant (p = 0.728) difference between the two groups. There was no significant difference in Sugaya classification between the two groups (Table 2). Each delamination subgroup (posterior and complete types) had two retear cases. The extent of delamination did not have any significant correlation with retear rate or Sugaya classification (Table 4).
Radiological outcomes of delamination group and non-delamination group.
Clinical results
Of the 148 patients, 138 (93.2%) were followed up for more than 2 years. Eighty-nine (64.5%) of the 138 patients were available for final follow-up at our outpatient clinic at a minimum of 2 year postoperatively. Forty-nine (35.5%) patients were followed up by phone survey to evaluate PVAS, FVAS, and ASES scores at the 2-year time point. PVAS, FVAS, and ASES were analyzed for 138 patients, including those by phone surveys. Constant score and ROM were analyzed for 89 patients who visited the outpatient clinic at the last follow-up.
Clinical results of the delamination group and the non-delamination group are presented in Table 3. Clinical scores were improved significantly in both groups postoperatively at the final follow-up, showing no significant difference between the two groups. In both groups, the ROM, but not external rotation, was significantly increased after surgery. The internal rotation showed better results in the non-delamination group at the final follow-up.
Clinical outcomes of delamination group and non-delamination group.a

PVAS: pain visual analog scale; FVAS: functional visual analog scale; ASES: American Shoulder Elbow Surgeons scores; ROM: range of motion.
a Values are presented as mean ± standard deviation.
b Constant score and ROM were analyzed in 89 patients (delamination: 78, non-delamination: 60).
Delamination subgroups (posterior and complete types) showed similar results (Table 4). Clinical scores were significantly improved after surgery in both subgroups, showing no significant difference between the two subgroups.
Clinical and radiological outcomes of posterior type and complete type in delamination group.a

PVAS: pain visual analog scale; FVAS: functional visual analog scale; ASES: American Shoulder Elbow Surgeons scores.
a Values are presented as mean ± standard deviation.
b Constant score was analyzed in 50 patients (posterior type: 21, complete type: 29).
Discussion
The principal finding of this study was that delamination in rotator cuff tears did not affect the clinical or radiological outcome in arthroscopic repair despite unfavorable circumstances for healing. The extent of delamination did not affect clinical or radiological outcomes either. Although this was a retrospective study of two different cohorts, it showed that the en bloc technique could lead to good results.
Several studies have previously reported results on delaminated rotator cuff tears. Boileau et al. 6 have determined supraspinatus repair healing after arthroscopic repairs and found that delamination tearing of subscapularis and infraspinatus is negatively associated with tendon healing. In the current study, delamination did not affect clinical outcome or healing rate. In a report on mini-open rotator cuff repair, MacDougal et al. 16 have shown that delamination does not affect clinical score or physical symptoms. Zilber et al. 22 have reported that infraspinatus delamination does not affect supraspinatus retear rate or clinical outcomes in open repair. Results of our study showed that delamination did not affect clinical outcome or healing rates after arthroscopic repair. Previous studies did not address the effect of the extent of delamination. We hypothesized that the extent of delamination would affect healing rate and clinical outcomes. However, there was no significant difference in clinical outcome or healing rate between “posterior type” and “complete type” of delamination.
Delamination occurred in just over 50% of our cases. In contrast, some studies have reported higher incidences. 8,16 Han et al. 8 have reported that the incidence of delamination is 88%, while MacDougal et al. 16 have reported an incidence of 71%. We excluded partial-thickness tears while other studies 16 categorized “high-grade partial tears” as delaminated tears and excluded massive-sized tears which could also have had delamination. As a result, several cases were excluded. If we had included partial-thickness tears and massive-sized tears, the incidence of delamination might have been higher.
Delamination is considered to a degenerative intra-substance tear. Matsuki et al. 9 have reported that the articular layer which consists of posterior oblique fibers of the infraspinatus is thicker and more retracted and degenerated than the bursal layer which consists of a combination of transverse fibers of the infraspinatus and supraspinatus. They also suggested that secure fixation of the articular layer is a key to achieving successful repair. Sugaya et al. 5 have reported favorable results with the double row technique, in which the repair of each layer is conducted separately for anatomical restoration. However, the double row technique is limited because the shear force between delaminated layers is still problematic. In contrast with the double row technique, the en bloc technique unites the delaminated cuff as a single construct for resolving shear forces in interlaminated layers and cover footprints. However, we did not compare separate repair with en bloc repair techniques. In a prospective comparative study by Kim et al., 17 separate repair and en bloc repair showed similar healing rates, although separate repair resulted in lower pain scores in the early (<1 year) postoperative period.
This study has several limitations. First, it was a retrospective study. Second, the outpatient clinic follow-up rate at 2 years was not high (64.5%). Hence, the constant score and ROM data might be prone to selection bias at 2 years follow-up. However, for patients who did not return at final follow-up, a single physiotherapist carefully collected data in the same way by phone survey. Third, our postoperative MRI follow-up rate was >70%. Only those patients who had MRI were included in the study. Thus, there is selection bias. Fourth, the clinical result of our study pertains to the en bloc technique done by a single surgeon which might be different from other techniques. Fifth, despite two separate evaluations of the video by two different shoulder-fellowship–trained orthopedic surgeons, reading errors could still be introduced, especially in the classification of subgroups. Finally, patients with small tears usually have less severe symptoms which may limit the comparison for the effect of delamination.
Conclusion
Arthroscopic en bloc repair for delaminated rotator cuff tear showed no significant difference in clinical or radiological outcome from that for non-delaminated rotator cuff tear. The extent of delamination did not affect the outcome either.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.