
Abstract
Background:
Fresh osteochondral allograft (OCA) is a treatment option that allows for the transfer of size-matched allograft cartilage and subchondral bone into articular defects of the knee. Although long-term studies show good functional improvement with OCA, there continues to be wide variability and a lack of consensus in terms of postoperative rehabilitation protocols and return to sport.
Purpose:
To systematically review the literature and evaluate the reported rehabilitation protocols after OCA of the knee, including weightbearing and range of motion (ROM) restrictions as well as return-to-play criteria.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
PubMed, EMBASE, Cumulative Index of Nursing Allied Health Literature, SPORTDiscus, and Cochrane databases were searched according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for studies on knee OCA. Studies were included if they reported return-to-play data or postsurgical rehabilitation protocols.
Results:
A total of 62 studies met the inclusion criteria, with a total of 3451 knees in 3355 patients. Concomitant procedures were included in 30 of these studies (48.4%). The most commonly cited rehabilitation protocols included weightbearing restrictions and ROM guidelines in 100% and 90% of studies, respectively. ROM was most commonly initiated within the first postoperative week, with approximately half of studies utilizing continuous passive motion. Progression to weightbearing as tolerated was reported in 60 studies, most commonly at 6 weeks (range, immediately postoperatively to up to 1 year). Of the 62 studies, 37 (59.7%) included an expected timeline for either return to play or return to full activity, most commonly at 6 months (range, 4 months to 1 year). Overall, 13 studies (21.0%) included either objective or subjective criteria to determine return to activity within their rehabilitation protocol.
Conclusion:
There is significant heterogeneity for postoperative rehabilitation guidelines and the return-to-play protocol after OCA of the knee in the literature, as nearly half of the included studies reported use of concomitant procedures. However, current protocols appear to be predominantly time-based without objective criteria or functional assessment. Therefore, the authors recommend the development of objective criteria for patient rehabilitation and return-to-play protocols after OCA of the knee.
Articular cartilage defects of the knee are relatively common, occurring in up to 60% of patients undergoing arthroscopic knee surgery. 71 These lesions can cause pain, locking, catching, swelling, and functional impairment. Untreated, articular cartilage defects can lead to osteoarthritis progression. 59,70 Cartilage defects pose a challenge in terms of treatment, in that they often occur in young, active patients who are eager to return to a high level of activity. Joint preservation with cartilage restoration is the mainstay of treatment in this patient population.
Multiple surgical options are available, including microfracture, autologous chondrocyte implantation, osteochondral autograft transfer, and osteochondral allograft (OCA) transplantation. OCA is a treatment option that allows for the transfer of size-matched allograft cartilage and subchondral bone into articular defects of the knee. 40,80 Advantages of this technique include the ability to treat larger lesions (>2 cm2), a lack of donor-site morbidity, the ability to transfer mature articular cartilage, and the fact it is a single-stage surgery. 29,71 OCA has demonstrated good results with significant improvements in clinical outcome scores and good durability with successful outcomes in 75% of patients up to 12 years after surgery. 3,19,25
Although long-term studies show good functional improvement with OCA, there continues to be wide variability and a lack of consensus in terms of postoperative rehabilitation protocols and return to sport. 3,11,19,22,30,40,42,48 A 2016 survey of 76 surgeons found significant heterogeneity in these protocols, ranging from immediate weightbearing as tolerated to nonweightbearing for 12 weeks, and time before returning to full activity ranging from 6 weeks to 6 months. 36 While these various protocols have been described, a standardized protocol that has been objectively evaluated against others has yet to be developed. Therefore, the purpose of this study was to systematically review the literature and evaluate the reported rehabilitation protocols, including weightbearing and range of motion (ROM) restrictions, as well as return-to-play (RTP) criteria after OCA of the knee. The authors hypothesized that weightbearing would be restricted for a mean of 6 weeks, ROM would be initiated immediately, and RTP would be delayed for 6 months after OCA of the knee.
Methods
Search Strategy
A systematic review was performed of studies with evidence levels from 1 to 4 regarding the rehabilitation protocols and RTP criteria after the use of fresh OCAs for knee cartilage injuries. A literature search was conducted using PubMed, EMBASE, Cumulative Index of Nursing Allied Health Literature, SPORTDiscus, and Cochrane databases from inception to March 2020. The investigation was completed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (Figure 1). Search terms included several combinations of the following: OCA, osteochondral allograft, and knee. Search results were gathered, and any duplicates were removed. Three independent reviewers (M.S., S.R., and B.G.) performed a title and abstract review of the articles under the direct supervision of a sports medicine–trained clinical fellow (R.A.J) to determine eligibility for full-text review. Full texts were then reviewed in a similar fashion to yield the final articles for inclusion. The references of the full texts were also reviewed for possible inclusion. Disagreements among the 3 reviewers were settled by the sports medicine clinical fellow and the senior author (K.B.F.).
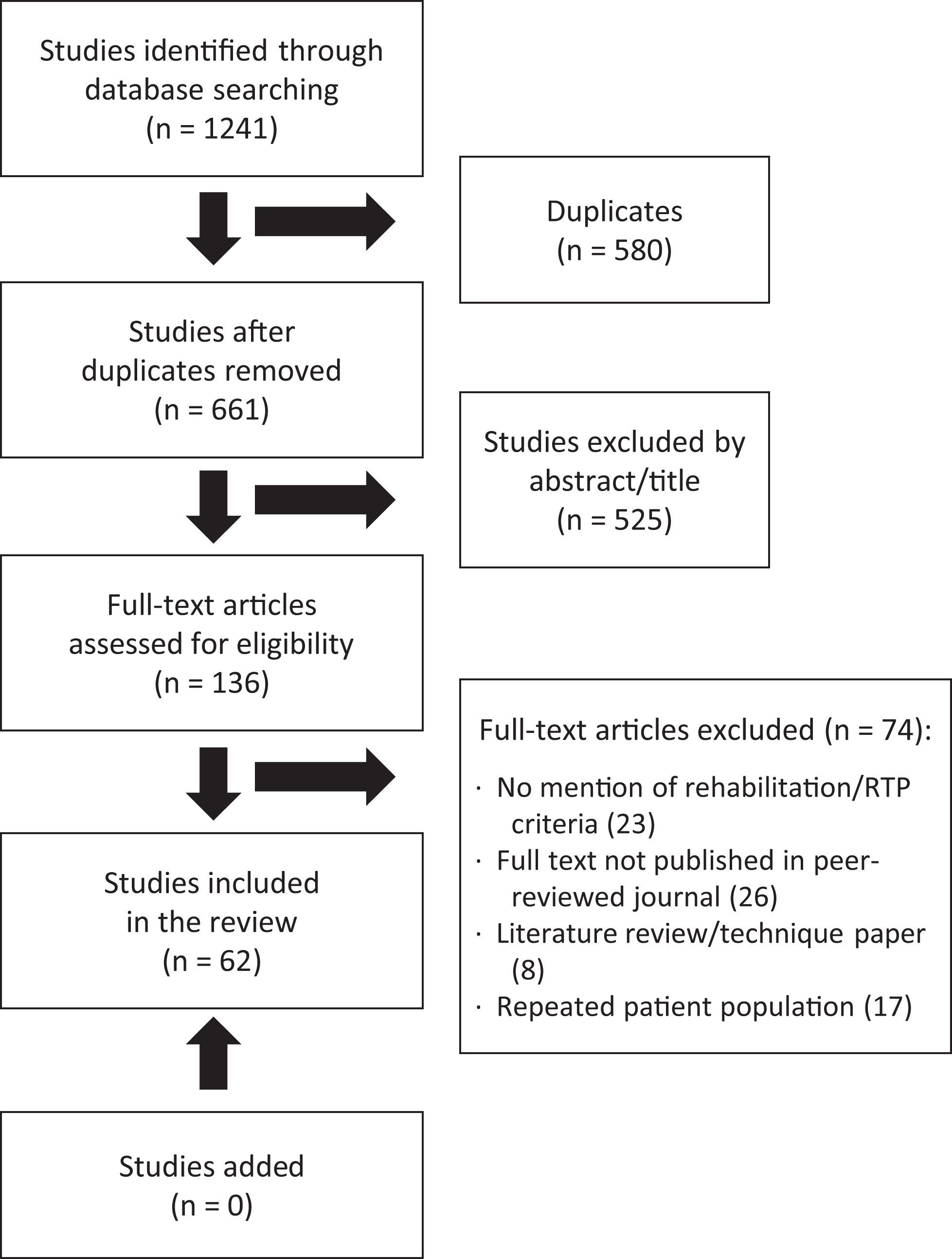
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) chart outlining the review of articles from the search. RTP, return to play.
Inclusion/Exclusion Criteria
Studies included were written in English and conducted on patients receiving OCA for knee cartilage defects and provided description of rehabilitation/RTP protocols. Excluded were literature reviews, case reports, technique articles, cadaveric studies, biomechanical studies, and studies that were not published in a peer-reviewed journal at the time the literature search was initiated. Additionally, in the event that multiple full-text articles used the same patient population, the single best representative article was used for data extraction, and the others were excluded. The search yielded 63 articles for inclusion in this investigation; these articles were compiled and extracted for data.
Data Extraction, Quality Assessment, and Analysis
From each study, we extracted the following details, when available: journal, year, study design, number of patients, demographics (age, sex, and body mass index), defect size, location of defect, number of grafts, rates and types of concomitant procedures, graft failure percentage, complication rates, postoperative rehabilitation protocols, RTP rates, RTP criteria, and outcome scores. We used the Coleman Methodology Score (CMS) to assess the methodological quality of the articles, reviewed independently by 2 authors (S.R. and B.G.). The CMS is composed of 10 questions designed to yield a score from 1 to 100, with higher scores indicating an article having a higher quality of evidence. 13 Data were collected and analyzed using Microsoft Excel.
Value Assessment of Rehabilitation and RTP Criteria
There is no validated measure to determine the adequacy of RTP protocols; however, this review used a 0 to 4 rating scale, previously described by Zaman et al. 79 Zero points indicates that the article did not include RTP criteria, while 4 points signifies well-defined RTP guidelines. One point was assigned for the presence of each of the following characteristics: rehabilitation protocol, timeline for return to activity, objective or subjective criteria, and specific measurements.
Results
Patient Characteristics and Quality Assessment
The mean CMS of the articles was moderate (57.8 ± 9.3) (Appendix Table A1). All included studies gave a detailed description of the surgical procedure, postoperative rehabilitation, and patient-selection process. Of the total articles, 45% reported follow-up out to 5 years, and only 1 study reported a follow-up of less than a year. However, 90% of studies were retrospective cohorts, and 84% had a study size of fewer than 100 patients.
Overall, 62 studies were included (Appendix Table A2). The studies analyzed 3451 knees in 3355 patients (1961 male, 1270 female, and 124 not reported) with a follow-up ranging from 6 months to 21 years. The mean patient age at the time of surgery ranged from 15.2 to 52.3 years. The indication for OCA in all studies was a chondral defect of the knee; however, the specific cause of the defect was reported in only 39 studies (62.9%). The most common reported cause was osteochondritis dissecans (n = 863). Additional causes were avascular necrosis (n = 145), degeneration (n = 240), trauma (n = 577), osteoarthritis (n = 93), and fracture (n = 13). The size of chondral defect was reported in 34 studies (54.8%), with a mean defect size ranging from 2.6 to 10.8 cm2. The location of the defect was reported in 50 studies, with the most common defect location being the medial femoral condyle (49.1%). Eight studies (12.9%) reported bipolar lesions of either the patellofemoral or tibiofemoral compartments.
Concomitant procedures were reported in 30 studies (48.4%). Concomitant procedures reported included high tibial osteotomy (HTO) (n = 254), meniscal allograft transplant (MAT) (n = 221), distal femoral osteotomy (DFO) (n = 122), anterior cruciate ligament reconstruction (ACLR) (n = 43), tibial tubercle osteotomy (TTO) (n = 38), hardware removal (n = 18), and medial patellofemoral ligament reconstruction (n = 7).
Rehabilitation Protocols
Continuous Passive Motion
The use of continuous passive motion (CPM) was included in 29 studies (46.8%); however, only 13 of those studies reported duration of postoperative CPM use. The most commonly reported timeline was 1 week, but this ranged from 1 to 8 weeks. Only 5 of the studies utilizing CPM detailed their protocol further (Table 1). LaPrade et al 40 described the most detailed protocol, with initiation of CPM immediately postoperatively, which was continued for 2-hour time intervals for a total of 10 hours per day for 8 weeks. Of those 5 studies reporting their protocol, the mean duration of CPM use was 7 hours, with a range of 4 to 10 hours daily.
Details of Continuous Passive Motion Protocol From 5 Studies

Bracing
The use of bracing was reported in 37 studies (59.7%). The timeline of use of the brace was reported in 35 studies (56.5%) and ranged from 1 week to greater than 6 months. Figure 2 further details the various timelines and how commonly they were used by the studies in this review. The majority of studies had a timeline cutoff for removal of the brace, but 5 (8.1%) studies reported objective criteria for brace removal. 16,27,60,62,76 The objective criterion noted in all 5 studies was the return of quadriceps strength. This was evaluated by the patient’s ability to perform a straight leg raise without an extension lag as well as the demonstration of quadriceps strength adequate to support ambulation.
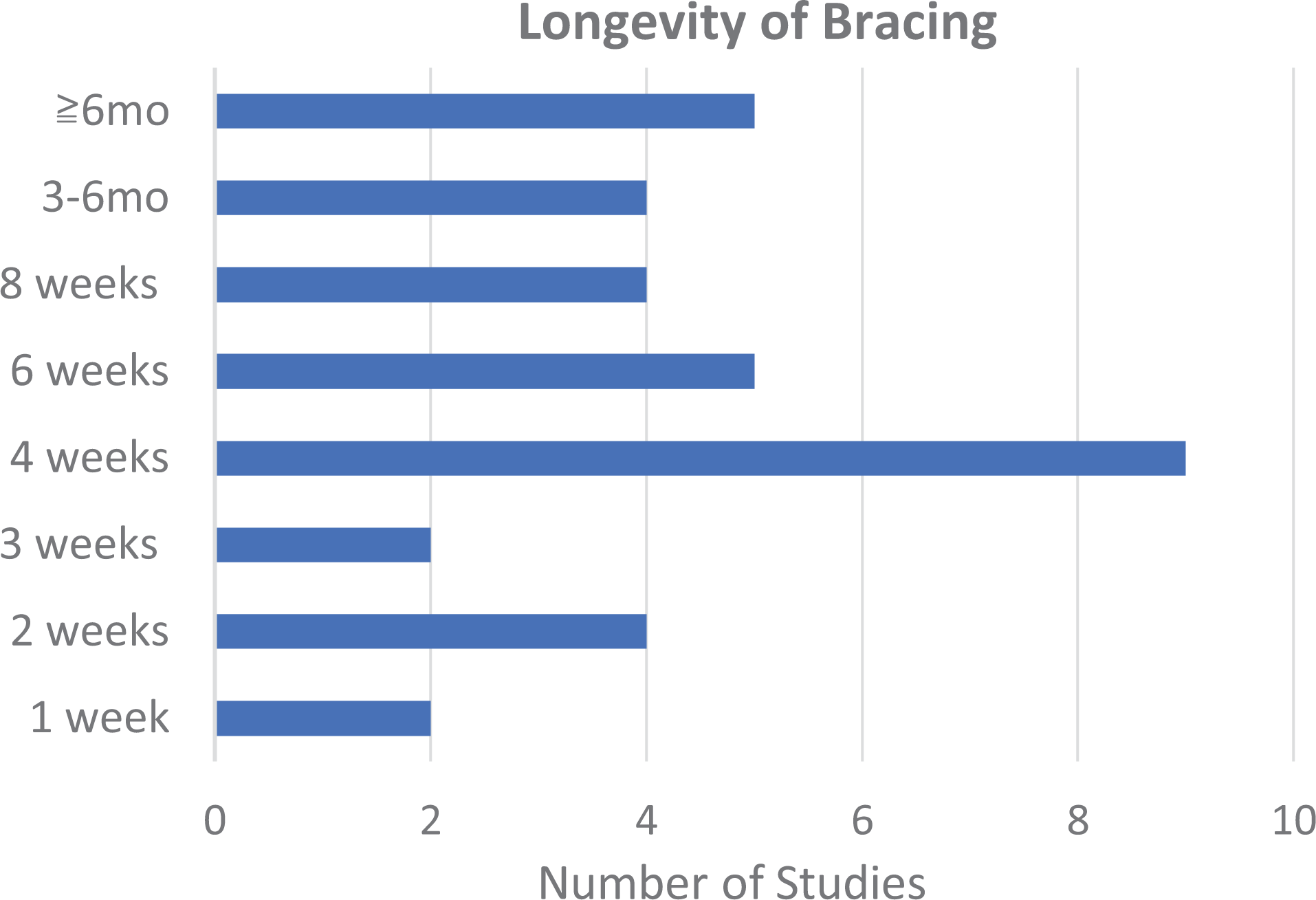
Timelines for length of brace use among articles reviewed.
Range of Motion
The time to initiate ROM was reported in 56 studies (90.3%) (Figure 3). ROM was most commonly initiated within 1 week, with 44 studies (71.0%) reporting this. Nine studies (14.5%) initiated ROM during the second postoperative week. The remaining 3 studies (4.8%) reported initiation of ROM during the fourth postoperative week. The majority of studies allowed for unrestricted ROM at the respective time points; however, 5 (8.9%) studies gave more detailed ROM protocols. 9,16,24,27,51 These studies included restricting ROM to certain degrees of motion, and most were specifically in patients who had patellofemoral OCA. A detailed breakdown of these restrictions is listed in Table 2.

Timelines to initiating range of motion (ROM) reviewed.
Details of ROM Protocol in 5 Studies a
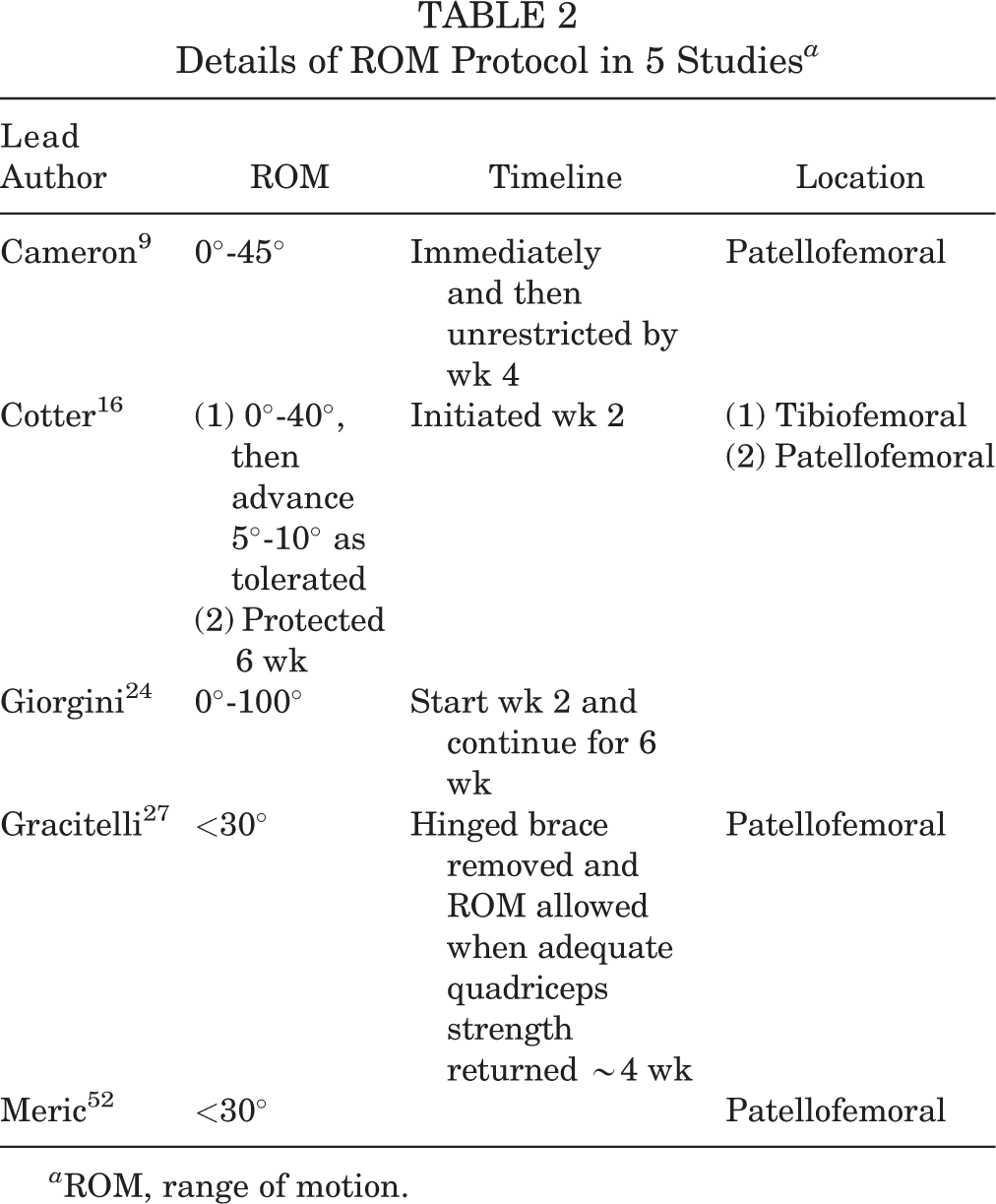
a ROM, range of motion.
While most studies maintained consistent postoperative ROM protocols for all patients, outside of changes due to lesion location (ie, patellofemoral), there was 1 study by Meyers et al 54 that altered them because of graft stability. The authors did not have specific criteria for assessing this; rather, they stated that a stable graft allowed nonweightbearing ROM, while a graft that had questionable stability would be placed in a long-leg cast in extension for 3 weeks. 54
Weightbearing
Time to weightbearing was reported in all 62 studies. Initiation of partial weightbearing was reported in 19 studies (30.6%), with a mode of 2 weeks and a range of immediately postoperatively to 6 weeks. Progression to weightbearing as tolerated was reported in 60 studies (96.8%), with a mode of 6 weeks and a range of immediately postoperatively to a delay of up to 1 year. The time point at which full weightbearing was initiated for each study is detailed in Figure 4.
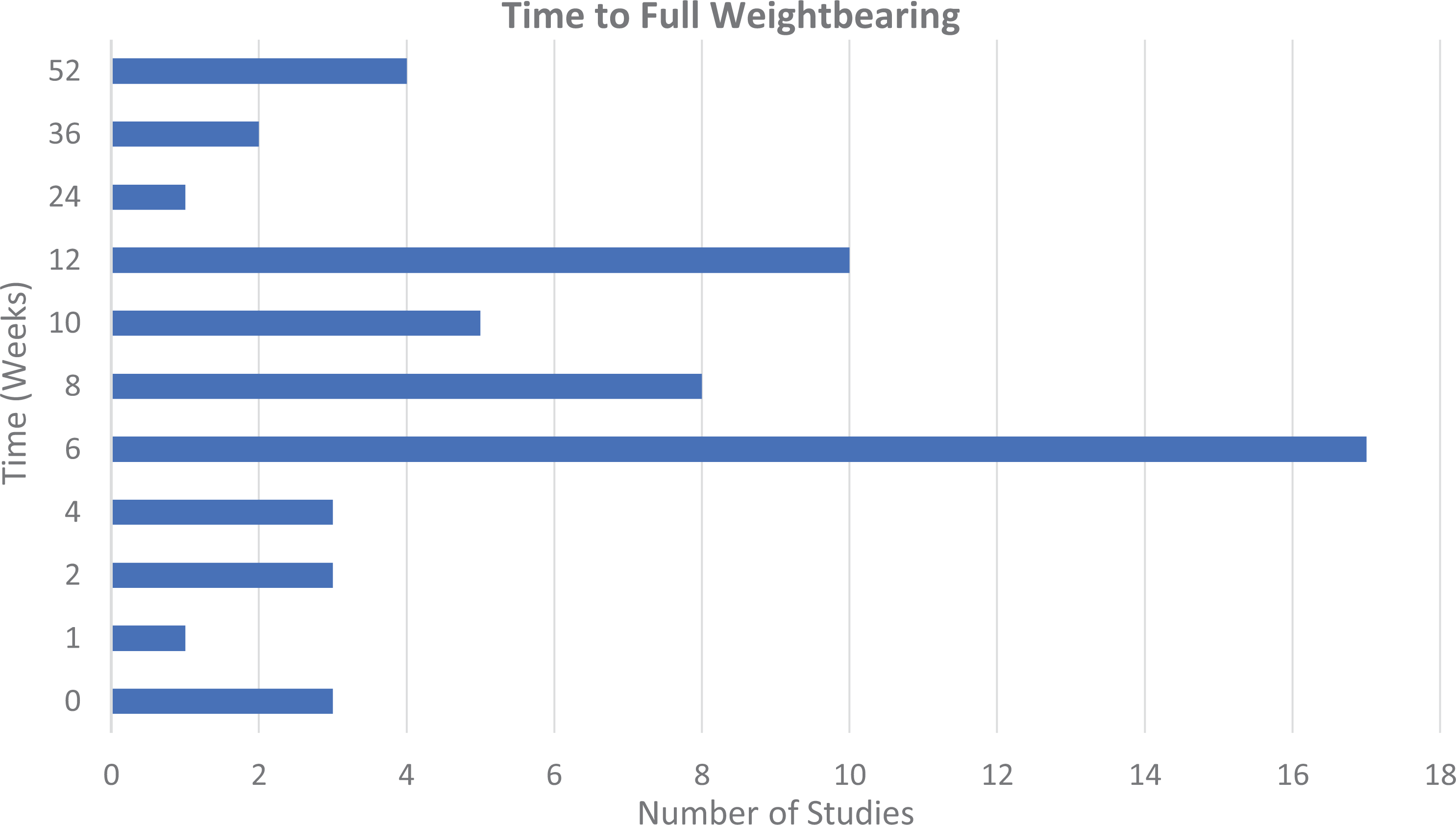
Timelines for allowance of full weightbearing among articles reviewed.
Nine studies specified an altered rehabilitation protocol when treating patellofemoral lesions. § The majority of these studies allowed immediate weightbearing as tolerated; however, the patient was placed in a brace locked in knee extension to prevent articulation of the repaired surface. Despite many of these studies allowing early weightbearing, there were still a few that required a period of nonweightbearing ranging from 6 weeks to 3 months. 9,16,51
While most studies maintained consistent postoperative weightbearing protocols for all patients, outside of changes due to lesion location (ie, patellofemoral), there was 1 study that altered them because of defect size. Garrett 22 altered the weightbearing protocol based off of the size of the graft restricting weightbearing for 6 weeks in lesions <3 cm and 3 to 4 months in lesions ≥3 cm.
Closed- and Open-Chain Exercises
As part of the rehabilitation process, many patients undergo physical therapy and perform various exercises focusing on strengthening and regaining function. Often, this requires utilization of closed- and open-chain exercises. Fifteen studies listed a time point when patients were able to initiate closed-chain exercises with a mode of 4 weeks postoperatively and range from 2 to 8 weeks. ∥ One study, however, did not mention a time point but stated that patients could initiate closed-chain exercise once the surgical wound had healed. 68 With regard to open-chain exercises, only 6 studies commented on a time point with a mode of 8 weeks and a range from immediately to 8 weeks postoperatively.
Imaging
Many studies mention obtaining some form of imaging over the postoperative course of treatment; however, only 7 studies required radiographic findings to progress patients through the postoperative rehabilitation protocol. The authors of these studies required radiographic signs of healing or osseous integration of the allograft to allow patients to bear weight. 14,18,25,42,54,56,58 The time point for which they obtained these radiographs ranged from 6 weeks to 1 year, with the most commonly reported time point being 3 months.
Modified Rehabilitation for Concomitant Procedures
Thirty studies reported the use of concomitant procedures, yet only 4 studies reported modification of rehabilitation and RTP protocols based on concomitant procedures. In 1 study, the longevity of bracing was increased in those patients who had either HTO or MAT, but the increased duration was not specifically defined. 8 Another study added a hinged knee brace for 3 weeks to delay full ROM in those undergoing any kind of ligament reconstruction or osteotomy, when typically their protocol called for no brace and immediate ROM. 17 In the additional 2 studies, the authors instituted a delay in RTP from 6 months to 8 to 12 months when 1 of the concomitant procedures performed was MAT, HTO, DFO, TTO, or ACLR. 21,53
RTP Criteria
All 62 studies contained rehabilitation protocols. Specific timelines for return to sport or activity were included in 41 studies (66.1%), and 13 studies (21.0%) included objective or subjective criteria for RTP. The mean RTP rating scale score overall was 1.9 ± 0.7, with no studies receiving a rating of either 0 or 4 (Table 3). In publications with RTP timelines, 18 studies reported timelines for return to running, with a mode of 6 months and a range from 3 months to 1 year. Two studies delayed RTP from 6 months to 8 to 12 months when MAT, HTO, DFO, TTO, or ACLR was performed in addition to OCA. 21,53 Twelve publications included time to return to jumping or plyometric activity, with a mode of 6 months and a range of 6 months to 1 year. The timeline to return to sport/return to activity without restriction was reported in 37 studies, with a mode of 6 months and a range of 4 months to 1 year (Table 4).
Results of RTP Rating Scale a

a From Zaman et al. 79 RTP, return to play.
RTP Timelines in the Studies Reviewed a
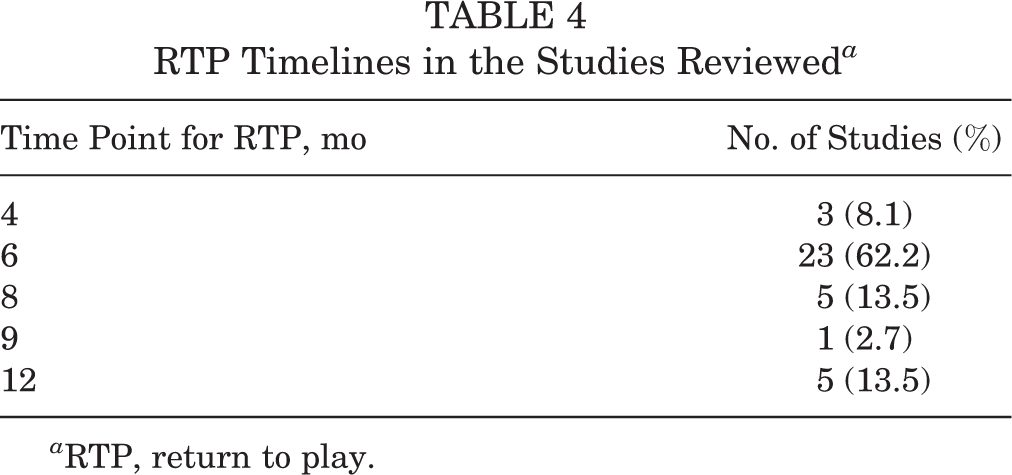
a RTP, return to play.
Objective and Subjective Criteria
Thirteen studies reported some form of objective or subjective RTP criteria for their patients. Twelve of the 13 studies utilized some form of objective criteria, while only 1 study utilized subjective criteria in determining readiness for RTP.
Four of the 12 studies utilized imaging as part of their RTP criteria. These studies required evidence of graft incorporation on radiographs to allow patients to progress to full activity. 24,43,61,64 One study, by Giorgini et al, 24 utilized both computed tomography (CT) and magnetic resonance imaging (MRI) scans throughout the postoperative course. They obtained CT scans at 3 months to assess cancellous and subchondral bone integration. Then, at 6 and 12 months, they obtained MRI of the knee to assess cartilage integration. Both of these imaging studies, with adequate integration of the graft, were required to progress their patients to full activity at 1 year.
The remaining 8 studies utilizing objective criteria were all based off of the functional recovery of the patient. 6,7,39,57,60,74,75,78 Factors most commonly cited included restoration of normal gait, quadriceps strength, coordination, and performance of sport-specific skills. Authors typically stated that this was the result of adequate progression through the physical therapy and rehabilitation protocols.
Finally, only 1 study cited any subjective criteria for RTP. Lee et al 41 proposed that RTP posed minimal risk to the allograft if the patient’s pain relief and function were acceptable for his or her specific sport. They also state that this point of recovery most typically occurs at 6 to 8 months postoperatively.
RTP Rates and Timelines
The RTP rate was reported in 7 studies and ranged from 75.2% to 100%. 6,15,37,39,44,47,57 RTP at the same level was reported in only 4 studies and ranged from 50% to 80%. 6,15,39,47 Patient-reported time to RTP was reported in 5 studies and ranged from 6 months to more than 2 years. 6,15,39,44,47
Discussion
At the time of this writing, rehabilitation and RTP criteria after OCA of the knee have not been standardized in the literature. This systematic review identified 62 studies reporting rehabilitation protocols after OCA of the knee. Of these, 41 studies reported time-based rehabilitation criteria, and 13 studies included objective or subjective rehabilitation criteria. Time to weightbearing was reported in all studies and ranged from 0 to 6 weeks. By summarizing the currently available literature, our goal was to outline specific criteria or consensus for both postoperative rehabilitation protocols and RTP protocols based on the best available literature.
Weightbearing guidelines were reported in all studies, and those protocols most commonly permitted partial weightbearing by 2 weeks postoperatively; however, this ranged from immediately postoperatively to 6 weeks. Early weightbearing can be advantageous by encouraging early mobility, which has been shown to be both psychologically and physically beneficial to the rehabilitation process after articular cartilage repair. 31 However, these benefits need to be balanced with protecting the graft site, as earlier weightbearing can potentially put excess strain on the site, leading to early failure. It is still unclear which time point is appropriate to allow full weightbearing. This was further demonstrated by this review with the most common time to allow full weightbearing being 6 weeks but ranging from immediately postoperatively to up to 1 year. The presence of bracing, a supplemental factor to weightbearing, was reported in 59.7% of studies. Overall, bracing was most commonly utilized for 4 weeks, but this too had a wide range from a minimum of 2 weeks postoperatively to greater than 6 months in some studies.
ROM timelines were reported in 90.3% of studies. The majority of studies (71.0%) allowed for initiation of ROM within the first postoperative week. This tendency to allow early ROM is supported by the clinical knowledge that prolonged immobilization can cause atrophy and stiffness as well as basic science research that suggests that early ROM is related to improved cartilage healing. 59 Approximately half of the studies in this review utilized CPM. However, the description of the CPM protocols was largely limited to the overall longevity of use, which was described in 44.8% of studies, with even fewer specifying the duration, frequency, and/or initial ROM used. Previous animal studies have demonstrated the benefit of CPM use with improved chondrogenesis and reduced cartilage breakdown; however, there is a general lack of clinical data available to support this. 20,38,66,76
The studies evaluated predominantly used time-based protocols, with very few utilizing measurements or patient-specific metrics as checkpoints for progression. RTP timelines were reported inconsistently, and there was notable variation within the reported timelines. The most common time to allow running activity was 6 months. Patients were permitted to progress to plyometric activity approximately 1 month later, and release to sport or activity without restrictions occurred at a similar time postoperatively. While time-based protocols do offer a framework within which adequate healing is able to occur, rehabilitation is highly patient dependent. Individualized criteria are suggested by the American Academy of Orthopaedic Surgeons regarding rehabilitation after ACLR, but no criteria exist for OCA. 46
Using the rating scale described by Zaman et al, 79 we found that with regard to providing objective or subjective criteria that a patient must meet to RTP, only 13 of the 62 studies fulfilled this category. Some of the most commonly cited criteria were restoration of normal gait and quadriceps strength, coordination, and graft healing demonstrated by imaging. However, almost all studies failed to define these criteria in objective, reproducible terms. Additionally, no studies received an overall rating of 4. By this evaluation metric, none of the studies included in this review sufficiently define their RTP protocol. The data extracted from these protocols, however, provide insight into the factors that are important to physicians postoperatively after OCA. Given the increase in fresh OCA transplantation in the young and athletic population, the authors recommend the creation of an RTP checklist similar to that of other common sports medicine procedures.
Most studies mention obtaining imaging at some point along the postoperative course; however, only 12 studies specifically mentioned utilizing imaging as criteria for progressing patients through rehabilitation and/or RTP protocols. Of those 12 studies, only 1 utilized advanced imaging such as CT and MRI. 24 With advances in imaging technology and access to 3-T MRI becoming more widely available, there has been establishment of scoring systems evaluating the quality of cartilage repair healing, specifically Osteochondral Allograft MRI Scoring System for OCAs. 10 This scoring system addresses cartilage signal, fill, and integration, as well as features of subchondral bone, and has been shown to correlate with clinical outcomes. 52,77 While this scoring system has been evaluated by multiple authors, there is no agreed-upon time point at which to obtain MRI postoperatively, and to date, no study has utilized this scoring system or any similar tool as a criterion to assess readiness for RTP. We cannot recommend for or against postoperative imaging for RTP decision-making. Additional dedicated studies are needed to determine whether advanced imaging is useful in this context.
Another factor highlighted by this review was the lack of standardized rehabilitation protocols for concomitant procedures with OCA despite concomitant procedures being reported in almost half of all studies on OCA. While the authors believe that major concomitant procedures such as ACLR or MAT likely significantly influence the rehabilitation course and RTP after OCA, few studies have specifically delineated to what extent or how the protocols were altered. Overall, 30 studies reported an incidence of concomitant procedures; however, only 4 of these reported how they affected the rehabilitation and RTP protocols. The most commonly reported concomitant procedures were MAT and HTO. In the 4 previously mentioned studies, patients who had undergone concomitant MAT or HTO had increased duration of bracing and/or delays in returning to play of up to 4 months. It is possible that the authors of the other 26 studies instituted similar modifications; however, it was not reported in any of their postoperative guidelines. This further illustrates the lack of detail and clarity with regard to appropriate rehabilitation of patients undergoing OCA.
Overall, this study has many strengths. It provides a comprehensive review of the literature for rehabilitation and RTP criteria after OCA of the knee. Moving forward, this will help serve as the baseline for the development for comprehensive criteria for returning to play after OCA of the knee.
There are also several limitations, many of which are inherent to all systematic reviews. The quality is subject to the level of evidence and biases of the studies included, thus limiting the conclusions that can be drawn from this analysis. Certain important athlete characteristics, including the level of the athlete, sport of the athlete, or number of athletes versus the general population, are unknown. Another key limitation for this study was that the assessment of RTP criteria and rehabilitation depended exclusively on what the authors reported in their papers. Nearly half of the studies included in this review included use of concomitant procedures, yet only 4 of 30 described how those procedures altered their rehabilitation or RTP protocols. It is possible that authors modified their own general rehabilitation protocols based on their own clinical judgment; however, this only stresses the need for the creation of a standardized, comprehensive list of guidelines. Additionally, this review included studies published as early as 1980, which allows variation because of general industry or practice changes. Last, because of the significant heterogeneity of data, a meta-analysis was not attempted.
Conclusion
There is significant heterogeneity for postoperative rehabilitation guidelines and an RTP protocol after OCA of the knee in the literature. With respect to articles including concomitant procedures, only 4 of the 30 studies made mention of alterations in their protocols, making it difficult to conclusively determine the extent to which the additional procedures may have contributed to the heterogeneity observed in this study. Therefore, we recommend that future studies describe the effect concomitant procedures have on their rehabilitation and RTP process. We also recommend the development of objective criteria for patient rehabilitation and returning to sports after OCA of the knee. These objective criteria should include a combination of imaging, subjective and objective functional assessment, and sport-specific criteria. By completing these goals, patients can confidently return to activities after OCA of the knee in a safe manner and ideally return to a preinjury level of function.
Footnotes
Notes
Final revision submitted January 3, 2021; accepted February 15, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.T. has received research support from DePuy Synthes, GID, and Pacira; consulting fees and speaking fees from Mitek, DePuy Synthes, and Pacria; educational support from Vericel and Liberty Surgical; and hospitality payments from Stryker, Smith & Nephew, Medical Device Business Services, Flexion Therapeutics, and Dynasplint; and holds stock in Johnson & Johnson. S.H. is an employee and holds stock in Johnson & Johnson and has received educational support from Liberty Surgical and Arthrex and hospitality payments from Smith & Nephew, Aastrom Biosciences, DePuy Synthes, Horizon Pharma, Ferring Pharmaceuticals, Anika Therapeutics, and Vericel. K.B.F. has received consulting fees from DePuy Synthes, Vericel, and Medical Device Business Services; educational support from Liberty Surgical; honoraria, speaking fees, and nonconsulting fees from Vericel; and hospitality payments from Smith & Nephew, Ferring Pharmaceuticals, Arthrex, Cumberland Pharmaceuticals, and Flexion Therapeutics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Patient Information and Rehabilitation and RTP Protocols for the Included Studies

| Lead Author | LOE | N | Mean Age, y | Mean Follow-up, y | RTP Criteria Score | RTP Criteria b | CPM c | Bracing c | Timeline to ROM | Timeline to WBAT |
|---|---|---|---|---|---|---|---|---|---|---|
| Ackermann 1 | 3 | 63 | 34.4 | 0.5 | 2 | Rehab, time | 4 wk | 4 wk | 1st wk | 4 wk |
| Anderson 2 | 3 | 38 | 52.3 | 3.7 | 1 | Rehab | Yes | 1 wk | 1st wk | 2 wk |
| Aubin 4 | 4 | 60 | 27 | 10 | 1 | Rehab | Yes | ≥6 mo | 2nd wk | 1 y |
| Bakay 5 | 4 | 33 | 48 | 1.6 | 1 | Rehab | 1 wk | 4 wk | 1st wk | 12 wk |
| Balazs 6 | 4 | 11 | 22.8 | NR | 3 | Rehab, time, gait/strength | No | 4 wk | 1st wk | NR |
| Balazs 7 | 4 | 46 | 26.2 | 3.25 | 3 | Rehab, time, gait/strength | 1 wk | 4 wk | 1st wk | NR |
| Brown 8 | 4 | 34 | 34.5 | NR | 1 | Rehab | No | 1 wk | 1st wk | Immediately |
| Cameron 9 | 4 | 28 | 30.2 | 7 | 2 | Rehab, time | No | Yes | 4th wk | 8 wk |
| Chu 11 | 4 | 55 | 35.6 | 6.25 | 1 | Rehab | 1 wk | No | 1st wk | 12 wk |
| Cinats 12 | 4 | 20 | 33 | NR | 1 | Rehab | No | No | 1st wk | 6 wk |
| Convery 14 | 4 | 36 | 35 | 5.5 | 2 | Rehab, radiograph | 1 wk | No | 1st wk | 12 wk |
| Cotter 16 | 4 | 26 | 31.9 | 7 | 2 | Rehab, time | No | 2 wk | 2nd wk | 6 wk |
| Cotter 15 | 4 | 37 | 26.01 | 7.3 | 3 | Rehab, time, strength | No | 4 wk | 2nd wk | 6 wk |
| Davidson 17 | 4 | 8 | 32.6 | 3.4 | 2 | Rehab, time | 3 wk | No | 1st wk | 6 wk |
| Early 18 | 4 | 25 | 25 | 11 | 3 | Rehab, time, radiograph | No | No | 1st wk | 12 wk |
| Emmerson 19 | 4 | 64 | 28.6 | 7.7 | 2 | Rehab, time | 1 wk | No | 1st wk | 12 wk |
| Frank 21 | 4 | 180 | 32.7 | 5 | 3 | Rehab, time, strength | No | 4 wk | 1st wk | 4 wk |
| Garrett 22 | 4 | 17 | 20 | 3.5 | 2 | Rehab, time | 1 wk | No | 1st wk | 6 wk |
| Ghazavi 23 | 3 | 123 | 35 | 7.5 | 1 | Rehab | Yes | ≥6 mo | 1st wk | 1 y |
| Giorgini 24 | 4 | 11 | 34 | 2.2 | 3 | Rehab, time, CT/MRI | No | 2 wk | 2nd wk | 10 wk |
| Görtz 25 | 4 | 22 | 24.3 | 5.6 | 3 | Rehab, time, radiograph | No | No | NR | 12 wk |
| Gracitelli 26 | 3 | 46 | 27.5 | 9.7 | 2 | Rehab, time | Yes | 4 wk | 1st wk | 10 wk |
| Gracitelli 27 | 4 | 27 | 33.7 | 9.7 | 3 | Rehab, time, strength | No | No | 4th wk | Immediately |
| Gracitelli 28 | 4 | 163 | 32.6 | 8.5 | 2 | Rehab, time | No | No | 1st wk | 10 wk |
| Gross 30 | 3 | 60 | 27 | 10 | 1 | Rehab | No | ≥6 mo | 8 wk | |
| Hannon 32 | 3 | 36 | 36.2 | 4.5 | 2 | Rehab, time | 1 wk | No | 1st wk | 6 wk |
| Harris 33 | 4 | 35 | 29.6 | 3.65 | 2 | Rehab, time | 6 wk | 6 wk | 1st wk | 6 wk |
| Hohmann 34 | 4 | 9 | 32.1 | NR | 2 | Rehab, time | No | Yes | 1st wk | 6 wk |
| Jamali 35 | 4 | 18 | 42 | 7.8 | 2 | Rehab, time | Yes | No | 1st wk | 12 wk |
| Karataglis 37 | 4 | 5 | 29.8 | 2.7 | 1 | Rehab | No | No | 1st wk | 12 wk |
| Krych 39 | 4 | 43 | 33 | 2.5 | 3 | Rehab, time, gait/strength | Yes | No | 1st wk | 4 wk |
| LaPrade 40 | 4 | 23 | 30.9 | 3 | 3 | Rehab, time, gait/strength | 8 wk | No | 1st wk | 8 wk |
| Lee 41 | 3 | 68 | 34.5 | 5.2 | 3 | Rehab, time, gait/strength | No | No | 4th wk | 8 wk |
| Levy 42 | 3 | 122 | 32.8 | 13.5 | 2 | Rehab, time | No | No | 1st wk | 10 wk |
| Locht 43 | 4 | 17 | 47.6 | 3.9 | 1 | Rehab | No | 3-6 mo | 9 mo | |
| Lyon 44 | 4 | 11 | 15.2 | 2 | 2 | Rehab, time | No | 6 wk | 1st wk | 10 wk |
| Mahomed 45 | 4 | 91 | 41.9 | 5.7 | 1 | Rehab | Yes | 3-6 mo | 1st wk | 1 y |
| McCarthy 47 | 3 | 13 | 19.2 | 5.9 | 1 | Rehab | 6 wk | 4 wk | 1st wk | 10 wk |
| McCulloch 48 | 4 | 25 | 35 | 3 | 1 | Rehab | Yes | No | 1st wk | 6 wk |
| McDermott 49 | 3 | 100 | 48 | 3.8 | 1 | Rehab | No | ≥6 mo | 2nd wk | 6 mo |
| Melugin 50 | 4 | 19 | 31 | 3.5 | 2 | Rehab, time | No | 6 wk | 1st wk | 6 wk |
| Meric 51 | 4 | 46 | 40 | 7 | 2 | Rehab, time | No | 3-6 mo | NR | 12 wk |
| Merkely 53 | 4 | 26 | 36.2 | 3.1 | 2 | Rehab, time | No | 6 wk | 1st wk | 6 wk |
| Meyers 54 | 4 | 39 | 38.7 | 3.6 | 2 | Rehab, radiograph | No | 3 wk | NR | 12 wk |
| Mirzayan 55 | 3 | 14 | 28.9 | 2.7 | 1 | Rehab | Yes | 8 wk | 1st wk | 8 wk |
| Murphy 56 | 4 | 39 | 16.4 | 8.4 | 3 | Rehab, time, radiograph | No | No | NR | 10 wk |
| Nielsen 57 | 4 | 142 | 31.2 | 6 | 3 | Rehab, time, gait/strength | No | No | 1st wk | 6 wk |
| Nuelle 58 | 3 | 75 | 34.2 | 1.6 | 3 | Rehab, time, radiograph | Yes | 8 wk | 1st wk | 8 wk |
| Rauck 60 | 3 | 33 | 36 | Minimum 2 | 3 | Rehab, time, gait/strength | Yes | 2 wk | 1st wk | 1 wk |
| Raz 61 | 4 | 63 | 28 | 21.8 | 3 | Rehab, time, radiograph | No | 3-6 mo | 2nd wk | 9 mo |
| Riff 62 | 3 | 88 | 35.4 | 3.7 | 3 | Rehab, time, gait/strength | Yes | 2 wk | 1st wk | 6 wk |
| Rucinski 63 | 3 | 162 | 38.7 | 1 | 2 | Rehab, time | Yes | 6 wk | 1st wk | 6 wk |
| Sadr 64 | 4 | 135 | 21 | 6.3 | 3 | Rehab, time, gait/strength, radiograph | No | No | 1st wk | 8 wk |
| Salai 65 | 4 | 6 | 45 | 15 | 1 | Rehab | No | 3 wk | NR | 12 wk |
| Scully 67 | 3 | 18 | 26.7 | 3.4 | 1 | Rehab | No | No | 1st wk | 6 wk |
| Shaha 68 | 4 | 38 | 29.83 | 4.1 | 2 | Rehab, time | Yes | No | 2nd wk | 6 wk |
| Shasha 69 | 3 | 60 | 27 | 10 | 1 | Rehab | No | ≥6 mo | 1 y | |
| Tírico 72 | 4 | 187 | 31 | 6.7 | 2 | Rehab, time | No | No | 1st wk | 6 wk |
| Torga Spak 73 | 4 | 11 | 36.5 | 10 | 1 | Rehab | Yes | No | 1st wk | Immediately |
| Wang 74 | 3 | 173 | 33 | 2.7 | 3 | Rehab, time, gait/strength | Yes | 4 wk | 1st wk | 2 wk |
| Wang 75 | 4 | 113 | 34.2 | 4.5 | 3 | Rehab, time, gait/strength | No | 4 wk | 1st wk | 2 wk |
| Williams 78 | 4 | 19 | 34 | 4 | 3 | Rehab, time, gait/strength | 6 wk | 8 wk | 1st wk | 8 wk |
a CPM, continuous passive motion; CT, computed tomography; LOE, level of evidence; MRI, magnetic resonance imaging; NR, not reported; ROM, range of motion; RTP, return to play; WBAT, weightbearing as tolerated.
b ”Rehab” indicates that a rehabilitation protocol was in place. “Time” indicates a timeline criterion was in place. “Strength/gait/radiograph” all were subjective/objective criteria required for RTP.
c The duration of CPM/bracing use is documented if it was reported in the study; otherwise, it is documented as “yes” or “no” for the presence or lack of CPM/bracing.