
Abstract
Objective
The aim of this study is to assess the variability of postoperative rehabilitation protocols used by orthopedic surgery residency programs for osteochondral autograft transplantation (OAT) and osteochondral allograft transplantation (OCA) of the knee.
Design
Online postoperative OAT and OCA rehabilitation protocols from US orthopedic programs and the scientific literature were reviewed. A custom scoring rubric was developed to analyze each protocol for the presence of discrete rehabilitation modalities and the timing of each intervention.
Results
A total of 16 programs (10.3%) from 155 US academic orthopedic programs published online protocols and a total of 35 protocols were analyzed. Twenty-one protocols (88%) recommended immediate postoperative bracing following OAT and 17 protocols (100%) recommended immediate postoperative bracing following OCA. The average time protocols permitted weight-bearing as tolerated (WBAT) was 5.2 weeks (range = 0-8 weeks) following OAT and 6.2 weeks (range = 0-8 weeks) following OCA. There was considerable variation in the inclusion and timing of strength, proprioception, agility, and pivoting exercises. Following OAT, 2 protocols (8%) recommended functional testing as criteria for return to sport at an average time of 12.0 weeks (range = 12-24 weeks). Following OCA, 1 protocol (6%) recommended functional testing as criteria for return to sport at an average time of 12.0 weeks (range = 12-24 weeks).
Conclusion
A minority of US academic orthopedic programs publish OAT and OCA rehabilitation protocols online. Among the protocols currently available, there is significant variability in the inclusion of specific rehabilitation components and timing of many modalities. Evidence-based standardization of elements of postoperative rehabilitation may help improve patient care and subsequent outcomes.
Keywords
Introduction
Osteochondral lesions of the knee are a frequent cause of pain and dysfunction.1-3 Although their true incidence is unknown, approximately 60% of patients undergoing knee arthroscopy were found to have osteochondral lesions.4-6 Without proper treatment, patients with chondral defects face an increased risk of osteoarthritis due to cartilaginous disruption and the risk for further injury propagation. 7
In the appropriate patient, these defects are treated surgically due to the poor restoration potential and avascular nature of cartilage.8,9 Of the many treatment options, two restorative procedures commonly performed are osteochondral autograft transplantation (OAT) and osteochondral allograft transplantation (OCA) where the primary goal is to restore the smooth gliding surface of hyaline cartilage at the articular surface.10-12 An analysis of reoperation rates following cartilage restoration of the knee found patients undergoing OAT or OCA procedures to have a lower incidence of reoperation compared with autologous chondrocyte implantation (ACI). The study also found patients undergoing OAT or OCA procedures to have a decreased rate of conversion to arthroplasty compared with microfracture procedures. 13 Furthermore, studies have shown significant improvements in both International Knee Documentation Committee (IKDC) and Lysholm scores following both OAT and OCA procedures.14,15
Successful surgical outcomes in orthopedics can be largely influenced by postoperative rehabilitation, with specific focus on restoring range of motion, strength, and a return to baseline function. Within current literature, individual rehabilitation guidelines for OAT versus OCA are scarce and, as such, have been difficult to analyze. More recent therapy programs are found to provide combined protocols for OAT and OCA procedures or are in the presence of concomitant procedures, such as ACI, mosaicplasty, and microfracture, yet little effort has gone into isolated analysis of these procedures.16,17 Although existing literature suggests that standardization of rehabilitation protocols could optimize therapy and decrease health care expenses, there are no standardized postoperative rehabilitation protocols for OAT or OCA.18,19
Postoperative rehabilitation for anterior cruciate ligament reconstruction, 20 medial patellofemoral ligament reconstruction, 21 meniscal repair, 22 proximal hamstring repair, 23 Achilles tendon repair, 24 ulnar collateral ligament reconstruction, 25 and microfracture 26 have been analyzed in previous studies and were noted to have considerable variation in content and timing for the initiation of different components of rehabilitation. The present study aims to assess the variability in OAT and OCA rehabilitation by utilizing online protocols published by academic orthopedic surgery programs in the United States. We hypothesize that significant heterogeneity in terms of rehabilitation exercises and their timing will be found among the published protocols, as well as deviations from current literature.
Method
Utilizing methods previously described to assess the variability of rehabilitation21-25 protocols, an online search was done for publicly available OAT and OCA rehabilitation guidelines from academic orthopedic surgery programs in the United States. A complete list of orthopedic surgery residency programs was obtained via https://residency.doximity.com. Searches and results specifically targeted academic institutions affiliated with a university or medical society to focus on the most evidence-based protocols available. Commercial websites, governmental and non-governmental organization (NGO) websites, and private practice physician websites were excluded to minimize bias, excessive variability, potential conflicts of interest, and other confounders. Similar to previous studies, a web-based query was performed in which the following 2 search terms were used: “[program name/affiliate hospital name/affiliate medical school name] osteochondral autologous transplantation rehabilitation protocol” and “[program name/affiliate hospital name/affiliate medical school name] OCA rehabilitation protocol.”21-25 Protocols specified to the skeletally immature population and patients undergoing concomitant procedures were excluded from the study. Procedures in the skeletally immature were excluded from the analysis as there is considerable variability in the management of osteochondral lesions in this population due to their increased healing potential in the setting of open physes. Protocols lacking clearly defined rehabilitation information, such as timing of the rehabilitation components, were also excluded from the study.
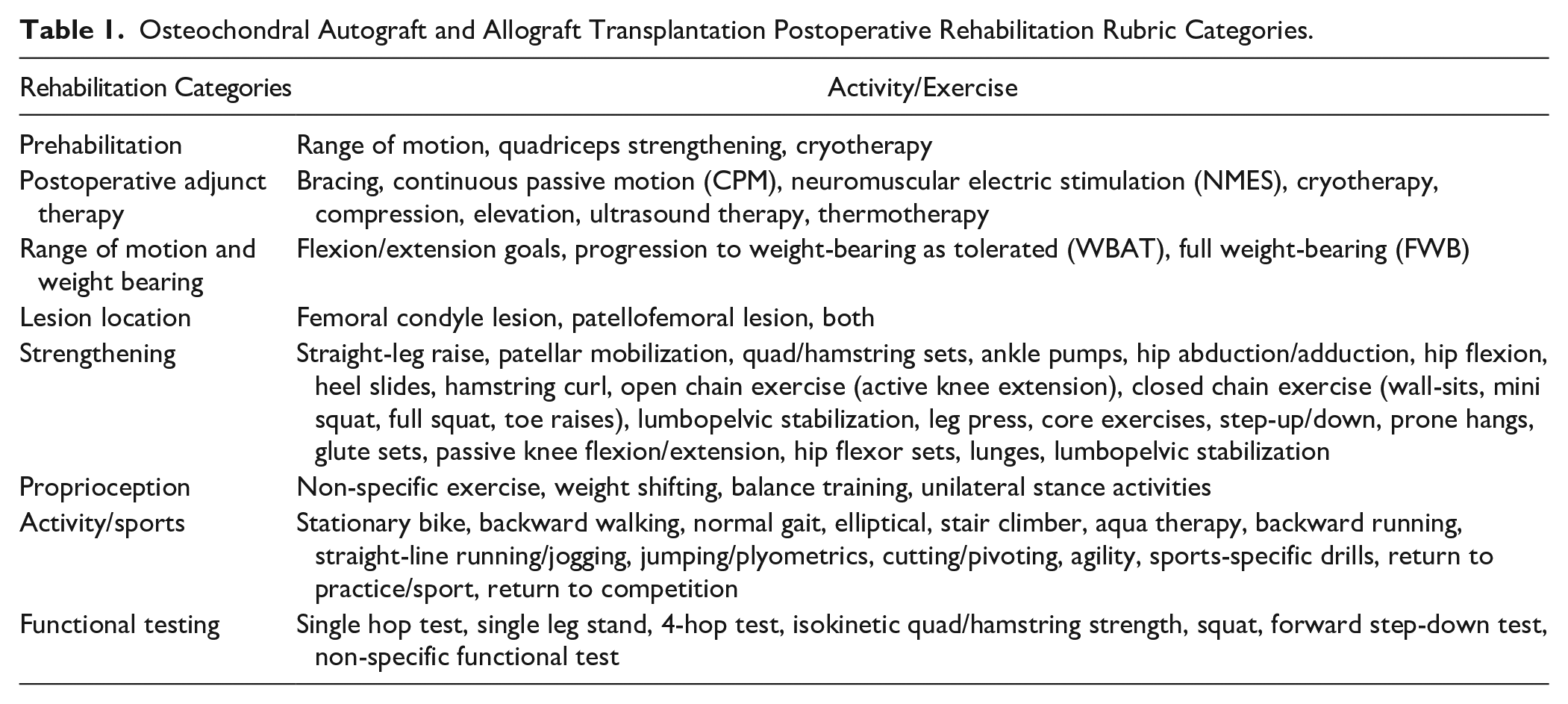
All collected protocols were transferred to a custom scoring rubric ( Table 1 ) with the following categories: timing and staging, prehabilitation, brace use, postoperative modalities, weightbearing status, non-ambulatory range of motion, lesion location, strengthening exercises, proprioceptive exercises, functional tests, return to basic activities, and return to athletic activities/sport. Protocols were then evaluated with binary coding for the presence or absence of the rehabilitation components listed above. Numerical scoring was utilized to evaluate the timing or range of timing for specifics within each component defined in the rehabilitation protocols themselves. The time of initiation for each modality in specified components was based on the earliest detailed time given in each protocol. The clinical appropriateness of each protocol for inclusion in the study was assessed by the authors with the senior author determining final inclusion of a protocol if a consensus was not obtained.
Osteochondral Autograft and Allograft Transplantation Postoperative Rehabilitation Rubric Categories.
Results
A total of 155 programs were included for review; 16 (10.3%) provided online academic protocols that met our eligibility criteria. Six institutions provided protocols for both OAT and OCA surgeries and 2 institutions provided multiple protocols (each attributed to different authors), producing a total of 35 protocols available for analysis. Of the 35 total protocols, 24 pertained to OAT in the following breakdown: 18 exclusive protocols for OAT and 6 applied to both OAT and OCA. Of the 35 total protocols, 17 pertained to OCA in the following breakdown: 11 exclusive protocols for OCA and 6 applied to both OAT and OCA
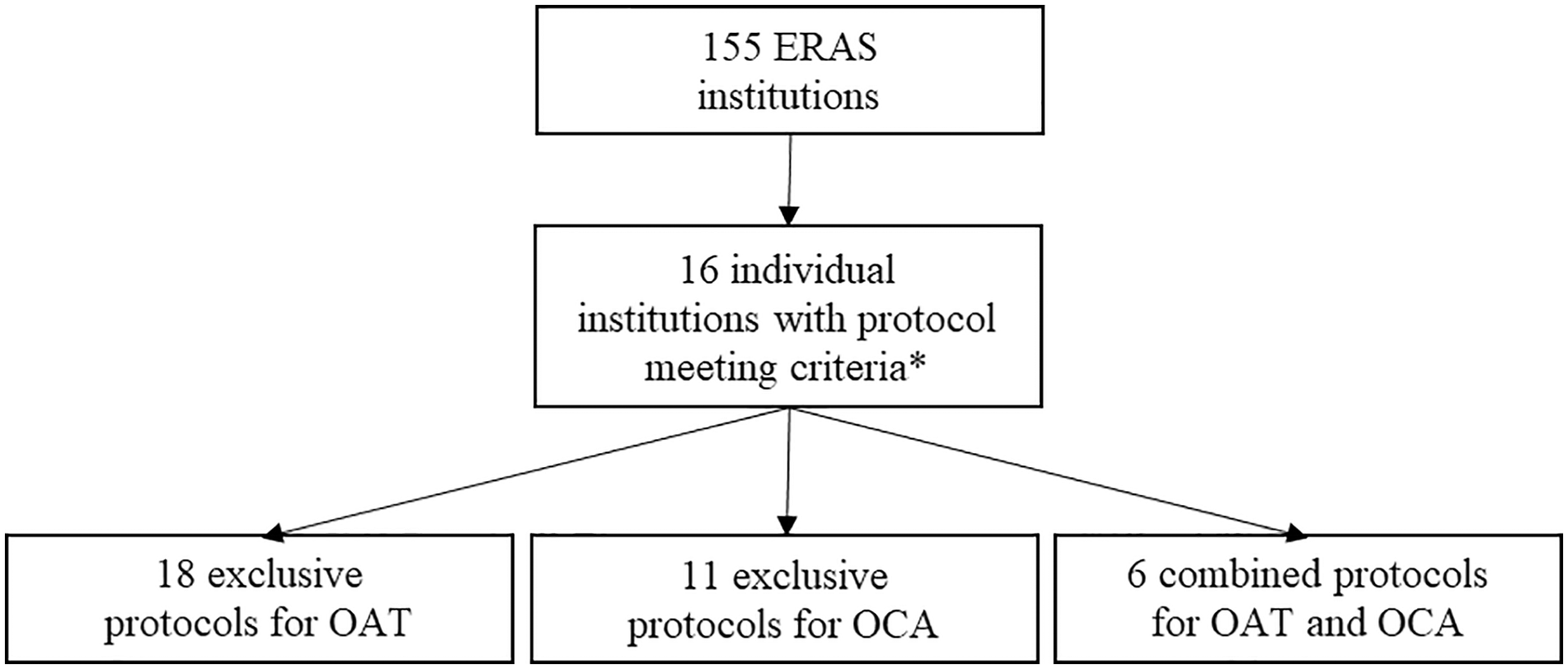
Collection of online postoperative rehabilitation protocols following OAT and OCA of the knee. The “*” refers to the eligibility criteria defined in our Methods section.
Prehabilitation
For OAT, 2 protocols (8.3%) recommended a preoperative rehabilitation program which included stationary cycling to maintain or improve range of motion (ROM) and 2 protocols (8.3%) provided recommendations on methods to decrease swelling with cryotherapy.
For OCA, no protocols recommended preoperative rehabilitation program.
Postoperative Adjunct Therapy
The 8 types of postoperative adjunct therapies assessed were bracing, continuous passive motion (CPM), neuromuscular electric stimulation (NMES), cryotherapy, compression, elevation, ultrasound therapy, and thermotherapy. For OAT, 23 protocols recommended CPM (96%), 10 recommended cryotherapy (42%), 7 recommended electrical stimulation (29%), 4 recommended elevation (17%) and soft tissue mobilization (17%), and 3 recommended compression (13%). All aforementioned modalities began in the immediate postoperative period. In terms of bracing, 21 protocols recommended immediate postoperative bracing (88%) with an average of 5.7 weeks (range = 0-8) of brace use. Locking of the brace in extension during ambulation was specifically mentioned in 15 of these protocols (63%). In the protocols that did not recommend bracing, there was no explicit recommendation either for or against bracing. Unlocking the brace during ambulation was recommended in 17 protocols (71%) at an average of 3.0 weeks (range = 0-7), postoperatively.
Fourteen protocols (58%) specified when to discontinue brace use. The most common criterion for brace removal was the ability to perform a straight-leg raise (SLR) without extension lag at the knee (29%). Other criteria included achieving a stable gait (8%) and sufficient quadriceps control throughout ROM (8%), both as determined by the treating provider.
Following OCA, 16 protocols recommended CPM (94%), 4 recommended immediate cryotherapy (24%), 3 recommended elevation (18%) and soft tissue mobilization (18%), and 2 recommended compression (12%). In terms of bracing, 17 protocols recommended immediate postoperative bracing (100%) with an average of 6.5 weeks (range = 0-8) of brace use. Locking of the brace in extension during ambulation was specifically mentioned in 14 protocols (82%). In the protocols that did not recommend bracing, there was no explicit recommendation either for or against bracing. Unlocking the brace during ambulation was recommended in 16 protocols (94%) at an average of 2.8 weeks (range = 1-7), postoperatively.
Ten protocols (59%) specified when to discontinue brace use, with SLR without extension lag (35%), followed by stable gait (12%) and sufficient quadriceps control throughout ROM (6%) as criteria for brace discontinuation.
Range of Motion, Weight Bearing, and Femoral Condyle versus Patellofemoral Lesions
All 24 OAT protocols prohibited any knee flexion in the immediate postoperative period, with 22 protocols (92%) allowing 90° of flexion at an average of 1.7 weeks (range = 0-6), 18 (75%) permitting 110° of flexion at an average of 3.4 weeks (range = 1-8), and finally 21 protocols (88%) specified full flexion at an average of 7.0 weeks (range = 2-13) postoperatively. Five protocols (21%) had clearly outlined weightbearing progressions to full weight-bearing (FWB). Five protocols (21%) permitted immediate weight-bearing as tolerated (WBAT) after surgery. The average WBAT date was 5.2 weeks (range = 0-8). The average proposed time to FWB was 6.9 weeks (range = 0-9)
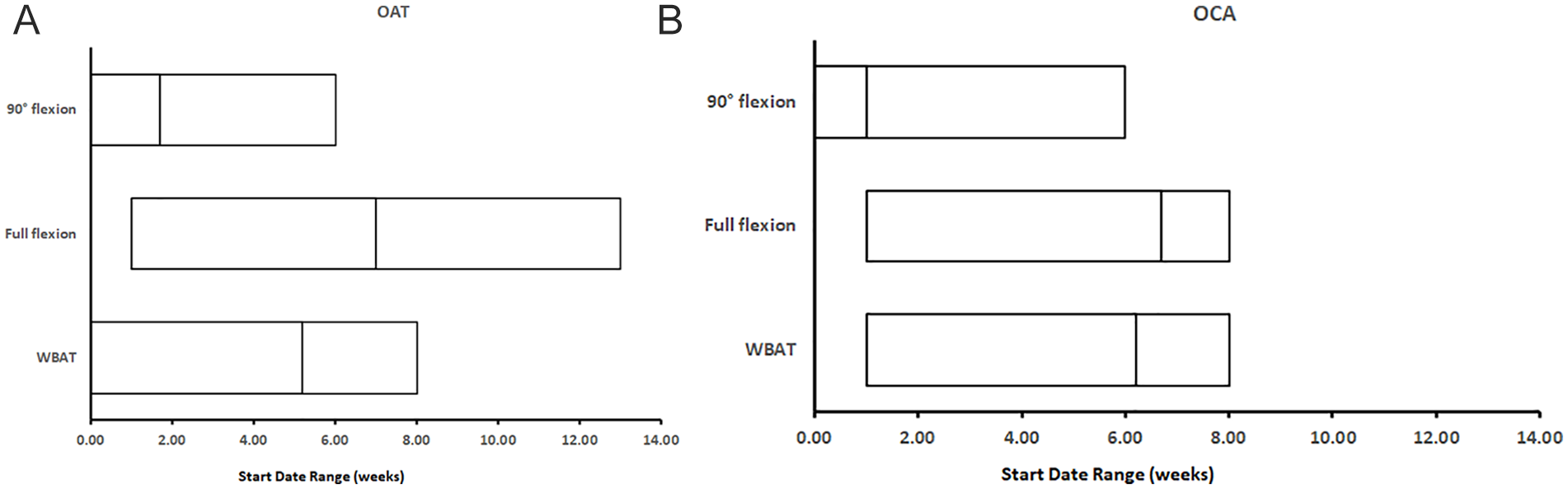
Range of motion and weight bearing. The numbered line within each range represents the mean of the data set. OAT = osteochondral autograft transplantation; OCA = osteochondral allograft transplantation; WBAT = weight-bearing as tolerated.
For OAT, 6 protocols (25%) specified rehabilitation for femoral condyle lesions and 7 protocols (29%) for patellofemoral lesions. The average WBAT date for femoral condyle lesions was 6.2 (range = 6-7) weeks, and the average WBAT date for patellofemoral lesions was 2.8 (range = 0-7) weeks. In terms of brace use, 4 protocols (66%) recommended immediate postoperative knee immobilization for femoral condyle lesions, and 7 protocols (100%) recommended immediate postoperative knee immobilization for patellofemoral lesions.
Similarly, all 17 OCA protocols prohibited knee flexion immediately postoperatively, while 17 protocols (100%) specified 90° of flexion at an average of 1.0 weeks (range = 0-6), 8 protocols (47%) allowed 110° of flexion at an average of 4.4 weeks (range = 1-6), and finally 17 protocols (100%) recommended full flexion at an average of 6.7 weeks (range = 1-8). Five protocols (29%) outlined weightbearing progression to FWB. Two protocols (12%) permitted immediate WBAT, while the average WBAT date was 6.2 weeks (range = 1-8). The average FWB goal date was 7.7 weeks (range = 6-12)
For OCA, 3 protocols (18%) specified rehabilitation for femoral condyle lesions and 3 protocols (18%) for patellofemoral lesions. The average WBAT date for femoral condyle lesions was 6.3 (range = 6-7) weeks, and the average WBAT date for patellofemoral lesions was 3.5 (range = 1-6) weeks. In terms of brace use, 6 protocols (100%) recommended immediate postoperative knee immobilization for both femoral condyle and patellofemoral lesions.
Strengthening
A total of 25 different strengthening exercises were included in the custom rubric. For OAT, on average, each protocol mentioned 13.7 (range = 0-14 weeks) strengthening exercises. Four exercises were recommended in more than 80% of all protocols, which included closed chain exercises, quadriceps/hamstring sets, SLRs, and calf pumps. There was a wide variation in timing to initiate common strengthening exercises. The largest ranges were found in the timing of quadriceps extension (range = 0-14 weeks), followed by hip adduction (range = 0-12 weeks), hamstring curl (range = 1-13 weeks), and core exercises (range = 1-13 weeks), which were all started over a 12-week range
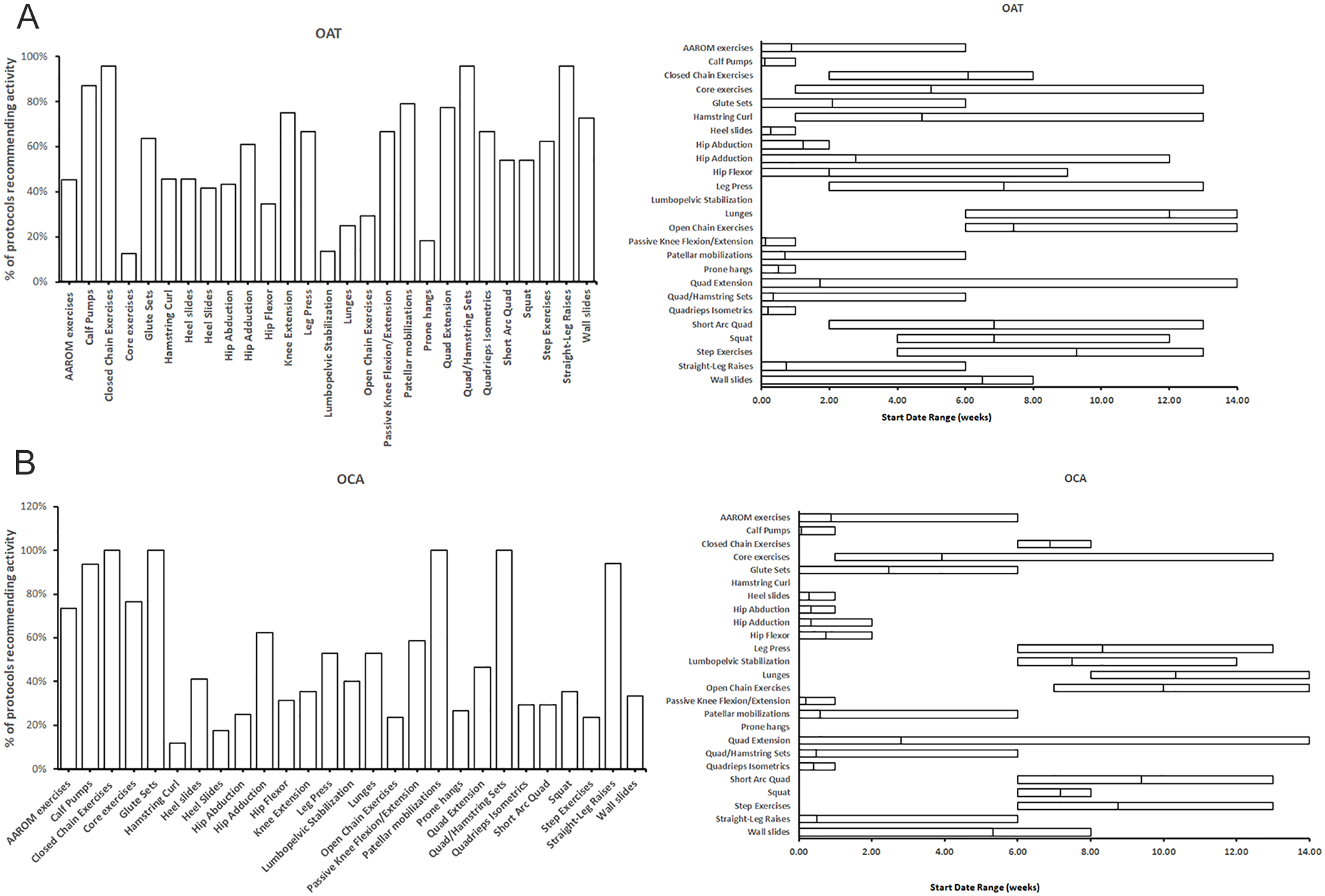
Strengthening exercises. (
For OCA, on average, each protocol included 13.2 (range = 0-14 weeks) strengthening exercises. Six exercises were recommended in more than 80% of protocols: closed chain exercises, quadriceps/hamstring sets, glute sets, patellar mobilizations, SLRs, and calf pumps. There was also a wide variation in timing to initiate common strengthening exercises. The largest ranges were found in the timing of quadriceps extension (range = 0-14 weeks), followed by core exercises (range = 1-13 weeks) and wall slides (range = 0-8 weeks)
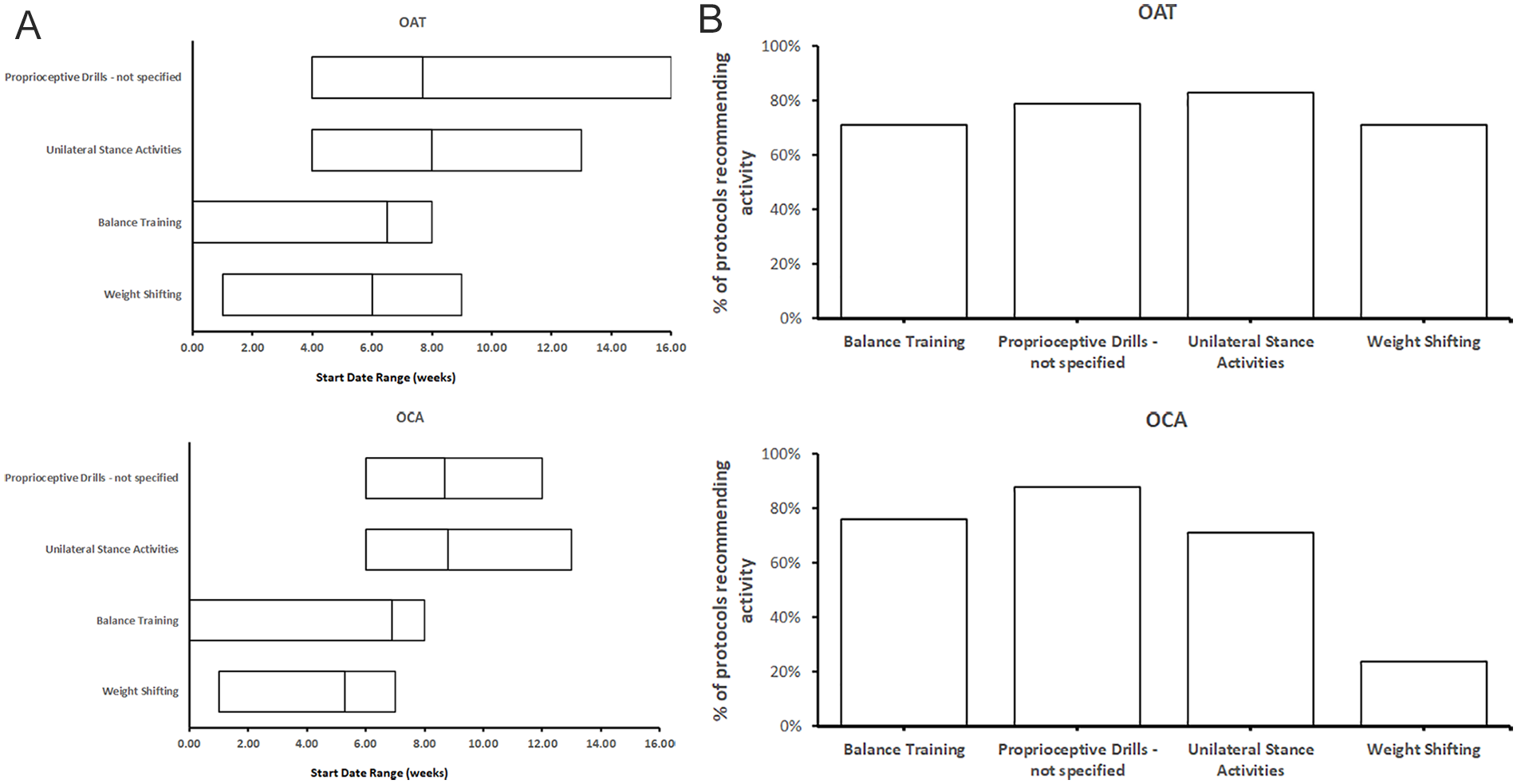
Proprioception and Functional Testing
Four different proprioceptive exercises were found in our analysis; weight shifting, balance training, unilateral stance activities, and unspecified proprioceptive drills. For OAT, at least one proprioceptive exercise was recommended by 22 protocols (92%), and the average number of proprioceptive drills recommended was 2.7 per protocol. Unilateral stance activities were recommended in 24 protocols (83%), unspecified proprioceptive drills were recommended in 19 protocols (79%), balance training was recommended in 17 protocols (71%), and weight shifting was recommended in 9 protocols (38%)
(
For OCA, at least one proprioceptive exercise was recommended by 17 protocols (100%), and the average number of proprioceptive drills recommended was 2.6 per protocol. Unspecified proprioceptive drills were recommended in 15 protocols (88%), balance training was recommended in 13 protocols (76%), unilateral stance activities were recommended in 12 protocols (71%), and weight shifting was recommended in 4 protocols (24%)
Although weight shifting was recommended at an earlier average time (6.0 weeks for OAT, 5.3 weeks for OCA), there was a similar starting range for the rest of the proprioceptive activities (unilateral stance training, balance training, and unspecified proprioceptive drills), with a combined average starting time of 7.4 weeks for OAT and a combined average starting time of 8.1 weeks for OCA.
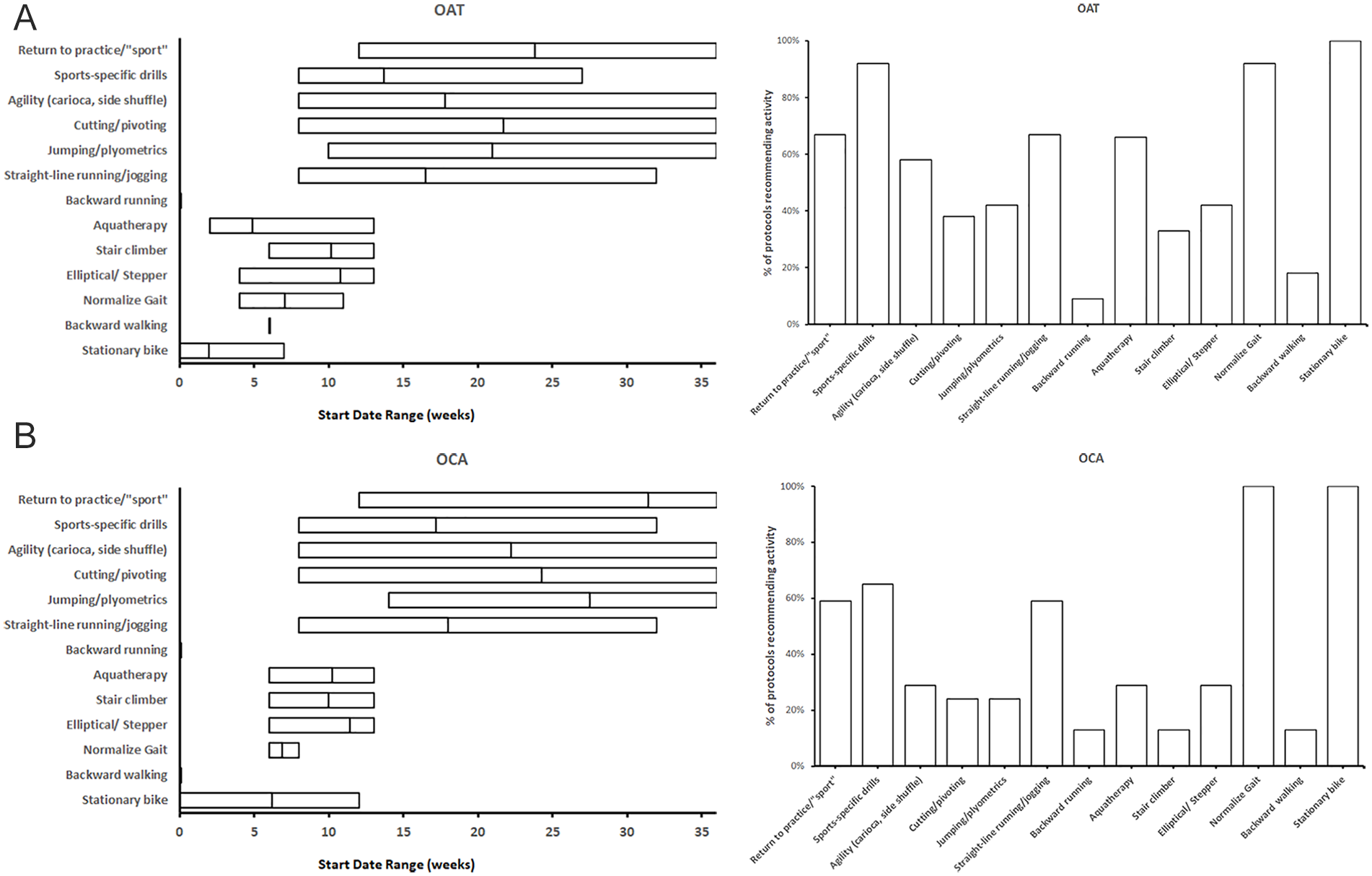
Return to Basic Activities and Sports
For OAT, common modalities recommended for returning to basic activities were stationary bike (100%) at an average of 2.0 weeks (range = 0-7), elliptical/stepper use (42%) at an average of 10.8 weeks (range = 4-13), hydrotherapy (67%) at an average of 4.9 weeks (range = 2-13), straight-line running (67%) at an average of 16.5 weeks (range = 8-32), stair climber (33%) at an average of 10.2 weeks (range = 6-13), and a normalized gait (92%) at an average of 7.0 weeks (range = 4-11). In terms of athletic activities, the most common exercise recommended was sports-specific drills (92%) beginning at an average of 13.7 weeks (range = 8-27). Agility drills (58%) were recommended at an average of 17.8 (range = 8-36) weeks, followed by jumping/plyometrics (42%) at an average of 21.0 (range = 10-36) weeks and cutting/pivot activities at an average of 21.7 (range = 8-36) weeks. Sixteen protocols (67%) specifically mentioned return to practice or sport as a postoperative goal at an average of 23.8 (range = 12-36) weeks. The criteria for return to sport was physician clearance in 6 protocols (25%) followed by use of functional testing in 2 protocols (8%). No protocols discussed return to competition
(
To expand on functional testing for OAT, 13 protocols (54%) recommended balance testing with the single leg stance, 11 protocols (46%) recommended squat testing, 10 protocols (42%) recommended unspecified testing activities, 8 protocols (33%) recommended isokinetic quadriceps strength testing, 7 protocols (29%) recommended isokinetic hamstring strength testing and forward step-down testing, 4 protocols (17%) recommended single hop testing, and 3 protocols (13%) recommended the 4-hop test. Functional testing overall was recommended in later stages of rehabilitation with an average start time of 12.0 (range = 0-24) weeks.
For OCA, common modalities recommended for returning to basic activities were stationary bike use (100%) at an average of 6.2 weeks (range = 0-12), elliptical/stepper (29%) at an average of 11.4 weeks (range = 6-13), hydrotherapy (29%) at an average of 10.2 weeks (range = 6-13), straight-line running (59%) at an average of 18.0 weeks (range = 8-32), stair climber (24%) at an average of 10.0 weeks (range = 6-13), and a normalized gait (100%) at an average of 6.9 weeks (range = 6-8). In terms of athletic activities, the most common exercise recommended was sports-specific drills (65%) at an average of 17.2 weeks (range = 8-32). Agility drills (29%) were recommended at an average of 22.2 (range = 8-36) weeks, followed by jumping/plyometrics (24%) and cutting/pivot training at an average of 27.5 (range = 14-36) and 24.3 (range = 8-36) weeks, respectively. Ten protocols (59%) specifically mentioned return to practice or sport as a postoperative goal at an average of 31.4 (range = 12-36) weeks. The criteria for return to sport was physician clearance in 8 protocols (47%) followed by a functional testing battery in 1 protocol (6%). No protocols discussed return to competition
For functional testing for OCA, 5 protocols (29%) recommended balance testing with the single leg stand and the squat test, 4 protocols (24%) did not specify the constituent activities, 3 protocols (18%) recommended isokinetic quadriceps strength testing, 2 protocols (12%) recommended isokinetic hamstring strength testing and forward step-down testing, 3 protocols (18%) recommended single hop testing, and 3 protocols (18%) recommended the 4-hop test. Functional testing overall was recommended later in rehabilitation with an average start time of 12.0 (range = 0-24) weeks.
Discussion
The results of this study demonstrate that a small number of academic orthopedic programs publish OAT and OCA rehabilitation protocols online. There was variability in both the nature and timing of recommended rehabilitation modalities and benchmarks, indicating that a standardized protocol does not exist. The most common modalities recommended in the reviewed protocols were the usage of CPM (96% for OAT and 94% for OCA), restricted postoperative knee flexion (100% for both OAT and OCA), and brace use (88% for OAT and 100% for OCA). While the majority of protocols recommended strength and proprioceptive training, there was variability in the specific exercises included and their timing of initiation. In addition, variation existed across postoperative weightbearing restrictions, brace parameters, and their subsequent timing. Lastly, weightbearing progression, return to sport timing, and the use of functional assessments for return to sport were included in a minority of protocols.
Weightbearing restrictions are applied following surgery to protect the transplanted graft from both compressive and shear forces. 16 However, several animal studies caution against lengthy immobilization and excessively cautious weight bearing due to associated thinning of articular cartilage and decreased synthesis of proteoglycan.27-31 From the protocols analyzed in this study, following OAT, patients achieved FWB status on average at 6.9 weeks postoperatively with the time ranging from 0 to 9 weeks. Following OCA, patients achieved FWB status on average at 7.7 weeks postoperatively with the time ranging from 6 to 12 weeks. Following OAT, current literature supports strict non-weight bearing for the first 2 weeks, as a 44% reduction in push-in and pull-out strength has been observed 1 week after surgery, 32 followed by toe-touch weight bearing from weeks 4 to 6, and FWB from weeks 6 to 8.17,32,33 In contrast, a more recent retrospective study recommends immediate return to FWB for small lesions (<1 cm2). 34 While some literature suggests non-weight bearing following OCA for the first 8 weeks with advancement to FWB between 8 and 12 weeks postoperatively, 16 other studies have reported good clinical outcomes with FWB at 6 weeks for OCA, providing some support to protocols recommending early weight bearing.35,36
When comparing present literature to the findings of our analysis of protocols from academic institutions, there were clear differences noted regarding when FWB status should be achieved. A systemic review on outcomes after articular cartilage surgery by Schmitt et al. 37 suggests using objective criteria of adverse tissue healing, such as increased effusion or strength deficits, rather than time-based criteria for weightbearing progression. However, optimal loads to facilitate articular cartilage remain unknown. While there is no consensus on the optimal timing of postoperative weight bearing, this rehabilitation milestone is clearly critical to avoid damaging healing graft sites and warrants future investigation. This underscores the importance for academic orthopedic surgery programs to recommend consistent, evidence-based protocols to instruct patients on weightbearing progression to minimize confusion and recovery time. Standardized clinical care pathways which follow evidence-based guidelines have been shown to improve the quality and efficacy of patient care as well as limit health care expenses. In patients undergoing total joint arthroplasty, following a standardized protocol has been shown to decrease complication rates and hospital length of stay, and improve efficiency of hospital and community resources.18,38-45 Similarly, following a standardized protocol of manual physical therapy and exercise selection has been shown to improve Harris Hip Scale scores, pain, and range of motion in both the short term and long term in individuals treated with hip osteoarthritis. 19 Although it is unknown if standardizing rehabilitation protocols following cartilaginous surgery of the knee, specifically in OAT and OCA, improves outcomes, these studies provide a basis for researchers to investigate this topic in the future.
Stiffness and flexion contractures are common complications following knee surgery. Following OAT and OCA, scars and adhesions may develop and restrict range of motion. 16 Prolonged immobilization increases the risk of stiffness and has been shown to impede cartilage healing.27,31 In the protocols analyzed in this study, CPM was recommended in approximately 95% of protocols for both OAT and OCA. In addition, the majority of protocols permitted passive knee range of motion but restricted immediate knee flexion postoperatively. Currently, literature on early ROM after cartilaginous surgeries has focused on animal studies with mixed results,46-48 but there is no consensus on the clinical utility of CPM.8,30,49,50
Protecting the transplanted graft postoperatively is paramount to allow for creeping substitution or the slow resorption of the graft with concurrent deposition of new bone. 51 Lesions on the femoral condyle must avoid compressive forces on the knee’s weightbearing surface while patellofemoral lesions must avoid shearing forces to protect the healing graft site. 52 For patellofemoral lesions, current literature recommends restricting knee flexion to 30° to 45° with a brace for the first 4 to 6 weeks postoperatively following OAT or OCA.53-55 This is done to protect the graft site from damaging forces, as the median ridge of the patella is prevented from contacting the trochlear groove.17,35 In contrast, graft sites on the femoral condyle are less susceptible to damage. Therefore, knee flexion is less strict and typically allowed as quadriceps strength returns.55,56 In our study sample, brace use was recommended in the majority of protocols. However, a relatively small quantity of protocols specified rehabilitation guidelines based on lesion location (54% of OAT and 35% of OCA protocols), despite the evidence in favor of this approach. This further highlights the need for evidence-based protocols to guide patients on knee bracing based on their graft location.
Functional assessments were used in a minority of academic orthopedic surgery programs in their return to play criteria with just 8% of protocols for OAT and 6% of protocols for OCA including this recommendation. In addition, no protocols discussed timing or criteria for return to competition. Current literature notes overall return to play following OAT to be approximately 88.2% with an average time of 4.9 (range = 2.7-11.1) months. 57 For OCA, overall return to play was noted to be 75% to 79% with a variable range of 4 to 20 months.58-61 Literature on return to competition following OAT and OCA is relatively sparse. In one study of college and professional basketball players following OCA, the overall return rate to competition was noted to be 80% at a median time of 14 months. 62 Rather than time-based recommendations for return to play, functional assessments may be used as recent studies, specifically following anterior cruciate ligament (ACL) reconstruction, have supported functional performance testing as a superior method for return to sports and athletic activities.63-66 Currently, there is a paucity of data for functional testing as return to play criteria following OAT and OCA of the knee. As an athlete is planning to return to practice/sport, patients should exhibit their readiness at the end of rehabilitation through functional and athletic activities.
Overall, this study found heterogeneity among published protocols as well as deviations from current literature. Our results support the opportunity to standardize care and treatment practices following common orthopedic surgery procedures to improve patient outcomes.39,67-70 The lack of standardization observed in academic protocols highlights the necessity to optimize recovery following OAT and OCA surgery for osteochondral defects of the knee to improve clinical results. The rapid growth of the self-informed patient utilizing the Internet for their medical needs has increased the importance of clarity in health care information. 71 This systematic review reveals that there is currently a lack of publicly available ERAS protocols for the OAT and OCA procedures, as only 10.3% of all US orthopedic academic programs were found to have protocols. Even with this limited number of protocols, considerable variability was still evident. Explicit expectations and comprehensive explanations that are accessible to patients are imperative for safe and effective patient care and outcomes. We believe standardization of certain rehabilitation protocols can serve to benefit both physicians and patients as the patient mind-set has progressed from passive listener to active decision-maker. 68 By normalizing data from these academic institutions, we hope to optimize therapeutic treatment and improve the clinical success of these surgeries.
Limitations
This study has several limitations. Despite reviewing all 155 academic orthopedic surgery programs, only 35 protocols met qualification criteria and were included. Furthermore, this likely represents a minority of postoperative OAT and OCA rehabilitation protocols available online, as non-academic and individual surgeons may also upload protocols for patients. To focus on evidence-based rehabilitation modalities and their initiation, this study focused on protocols associated with academic institutions as performed in previous investigations.21-26 While many online protocols provide general guidelines, surgeons may individualize rehabilitation protocols based on patients’ preoperative condition and intraoperative findings. These protocols are often given to patients and physical therapists and, therefore, are not available online. Last, the details included in the rehabilitation protocol examined in the study varied widely. Many protocols used ranges in place of specified dates for parameters such as weight bearing, brace use, and strengthening exercises. Although these modalities were recommended between patients and physicians on an individualized basis, it emphasizes the need to improve the quality of information that is available on the Internet.
Conclusion
A small number of US academic orthopedic surgery programs publish OAT and OCA rehabilitation protocols online. There is considerable variability in the inclusion of specific rehabilitation modalities and the initiation of their timing. Patient care and outcomes may be improved with evidence-based standardization of postoperative rehabilitation.
Footnotes
Acknowledgments and Funding
We thank Cherry Aung, BBA, for her help with data analysis.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bryan M. Saltzman reports publishing royalties, and financial or material support from Nova Science Publishers. Charles A. Popkin reports financial or material support, and research support from Arthrex, Inc.; financial or material support from Smith & Nephew; and is a Board or Committee member for USA Hockey Safety and Protective Equipment Committee. The remaining authors, Stephen G. Crowley, Anthony Pedersen, Thomas A. Fortney, Hasani W. Swindell, and David P. Trofa, declare there is no conflict of interest to the prepared work.
Ethical Approval
The author(s) did not seek ethical approval for this study.