
Abstract
Background:
Although the most common injury mechanism for pectoralis major (PM) tears is an eccentric loading mechanism typically caused by bench pressing, within the military, there is a unique injury mechanism associated with airborne operations. The results of operative repair for these parachute-induced PM tears have not been previously reported.
Purpose/Hypothesis:
To assess the functional outcomes in military servicemembers undergoing operative repair of parachute-induced PM tears. We hypothesized that functional recovery would be impaired with delayed surgical intervention.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were active duty military servicemembers who underwent operative repair for PM tears caused by a parachute-induced mechanism. Charts were reviewed to identify characteristic, injury, and surgical variables. Patients completed the functional outcome assessment with the Disabilities of the Arm, Shoulder and Hand (DASH) and the American Shoulder and Elbow Surgeons (ASES) questionnaires. Outcomes were compared between patients treated within 6 weeks of injury and those treated beyond 6 weeks.
Results:
Of the 68 identified PM tears, 25 were the result of parachute-induced mechanisms. A total of 13 patients consented and completed the functional outcome assessment. The mean patient age was 30.6 ± 6.4 years, and the mean follow-up period was 5.46 ± 1.26 years. Ten patients underwent repair within 6 weeks of injury, and the remaining 3 patients underwent repair at a mean of 338 days after injury (95% CI, -42.8 to 718.8 days), a significant difference between groups (P = .006). All 13 patients were able to return to military duties at a mean of 6 months from injury. Patients treated within 6 weeks of injury had significantly higher functional outcomes (DASH score, 6.17 vs 26.67; P = .018; ASES score, 85.97 vs 49.5; P = .008), with greater strength performance compared with preinjury (bench press, 90.58% vs 38.95%; P = .0057; push-ups, 81.9% vs 23.8%; P = .023) compared with patients treated beyond 6 weeks of injury.
Conclusion:
Operative repair of parachute-induced PM tears within 6 weeks of injury provided a superior functional and strength recovery when compared with delayed surgical repair. Acute repair should be recommended for military servicemembers who experience this unique injury mechanism.
Pectoralis major (PM) tendon tears are well-recognized injuries in military populations. Balazs et al 3 reported an injury incidence of 60 per 100,000 person-years in a review of all active-duty military servicemembers. Although the vast majority of these injuries occur as a result of weight lifting injuries, additional mechanisms have been recognized in military servicemembers. 6,22,23,25,28 One such rare but unique injury mechanism is a traumatic tear associated with airborne operations, and it is specific to static line parachuting. 24 Incorrect positioning of the static line during airborne operations results in violent abduction and external rotation of the arm after exit from the aircraft and has been associated with PM tears and biceps brachii injuries (Figure 1).

Illustration of incorrect static line placement (in yellow). It is positioned under the armpit, which produces violent abduction and external rotation of the arm after exit from the aircraft. Proper placement is with the arm close to the body and the static line outside of the arm. The image reproduced with permission of SLACK (Wilson DJ, Parada SA, Slevin JM, Arrington ED. Intrasubstance ruptures of the biceps brachii: diagnosis and management. Orthopedics. 2011; 34(11):890-896 30 ).
A recent magnetic resonance imaging study of PM tears in an active-duty Army population identified that static line-induced tears represented 36% of PM tears. 24 Additionally, these injuries were identified as having distinct differences in the tear characteristics. Compared with eccentrically loading PM tears caused by weight lifting, static line PM tears had a significantly higher rate of avulsion tears, representing 81% of the tears in the static line cohort. Tears involved both the sternal and clavicular heads of the PM in 68% of this cohort, although this was not statistically different from the weight lifting cohort. 24
In this specific population, operative treatment is most commonly recommended, as these injuries typically occur in fit, active, younger patients with high-demand activity and job requirements. Previous studies have reported the functional outcome of PM repair in military populations secondary to weight lifting mechanisms. 2,3,20,21,29 However, to date, no study has reported the functional outcome of PM tears secondary to static line parachuting injury mechanisms. This study sought to evaluate the midterm functional outcomes of operative repair in military members who sustained parachute-induced PM tears. We hypothesized that the functional recovery of parachute-induced PM tears would be comparable with previous data reported on weight lifting–induced PM tears and that delayed treatment would result in worse functional outcomes.
Methods
After obtaining institutional review board approval, we conducted a retrospective review of all patients who underwent PM tendon repairs at a single military medical center with a colocated airborne operations center. Patients were treated by 1 of 13 military orthopaedic surgeons between January 1, 2012, and December 31, 2016. Patients were considered for study inclusion if they were active-duty military servicemembers, sustained PM tear secondary to parachute-induced injury, were older than 18 years of age, and had >4 years follow-up since injury. Patients were excluded if they did not undergo a PM repair, were nonactive duty, sustained a PM tear by a mechanism other than static line injury, were younger than 18 years of age at the time of surgery, or had <4 years of follow-up.
Identified patients underwent a medical record review to confirm mechanism of injury, record demographic information, and record information pertaining to their injury. Operative reports were reviewed to identify the location of injury (defined as musculotendinous, intratendinous, or avulsion—with or without an osseous fragment), extent of injury (defined as either involving the sternal head, clavicular head, or both heads), and the technique utilized for operative repair.
Identified patients were then contacted by telephone to determine their willingness to participate in the current study and to complete a patient-reported functional outcome assessment. Functional outcome measures included the Disabilities of the Arm, Shoulder and Hand (DASH) and the American Shoulder and Elbow Surgeons (ASES) questionnaires. Supplemental questions were asked inquiring about their preinjury and current strength assessment, defined as maximal bench press and number of push-up repetitions within a 2-minute time period, military occupation, postoperative recovery period, current pain assessment via a visual analog scale (VAS), and long-term outcomes and satisfaction according to a previously published questionnaire. 2
Participating patients were divided into 2 groups based on acuity of repair, defined as immediate (<6 weeks after injury) or delayed (>6 weeks after injury) to determine the influence on the functional outcome as has been previously reported. 2 Minimal clinically important differences (MCIDs) were defined for the DASH score (10.83 points), the ASES (17 points), and the VAS pain score (1.3 points). 9,26,27 Statistical analysis was performed using SPSS Version 24 (SPSS). Significance was set at P < .05. Descriptive statistics were calculated, and Student t tests were used to determine the effect of acuity of PM repair on the functional outcome. For assessed variables, 95% CIs were calculated for comparison.
Results
Over the 4-year study period, a total of 68 patients underwent a PM repair with 25 (36.8%) of these patients meeting inclusion criteria as having undergone a PM repair caused by a static line injury during airborne operations (mean age, 31.69 ± 6.49 years; 100% men; mean follow-up, 5.3 ± 1.12 years). Of the identified 25 patients, 13 consented to participate in this study, completed the functional outcome assessments, and were included in the study (mean age, 30.6 ± 6.4 years; mean follow-up, 5.46 ± 1.26 years). The remaining 12 patients refused to participate in the current study and were therefore excluded from the analysis. A list of patient demographic information and summary of outcome variables is provided in Tables 1 and 2.
List of Characteristics of Patients who Agreed to Study Participation
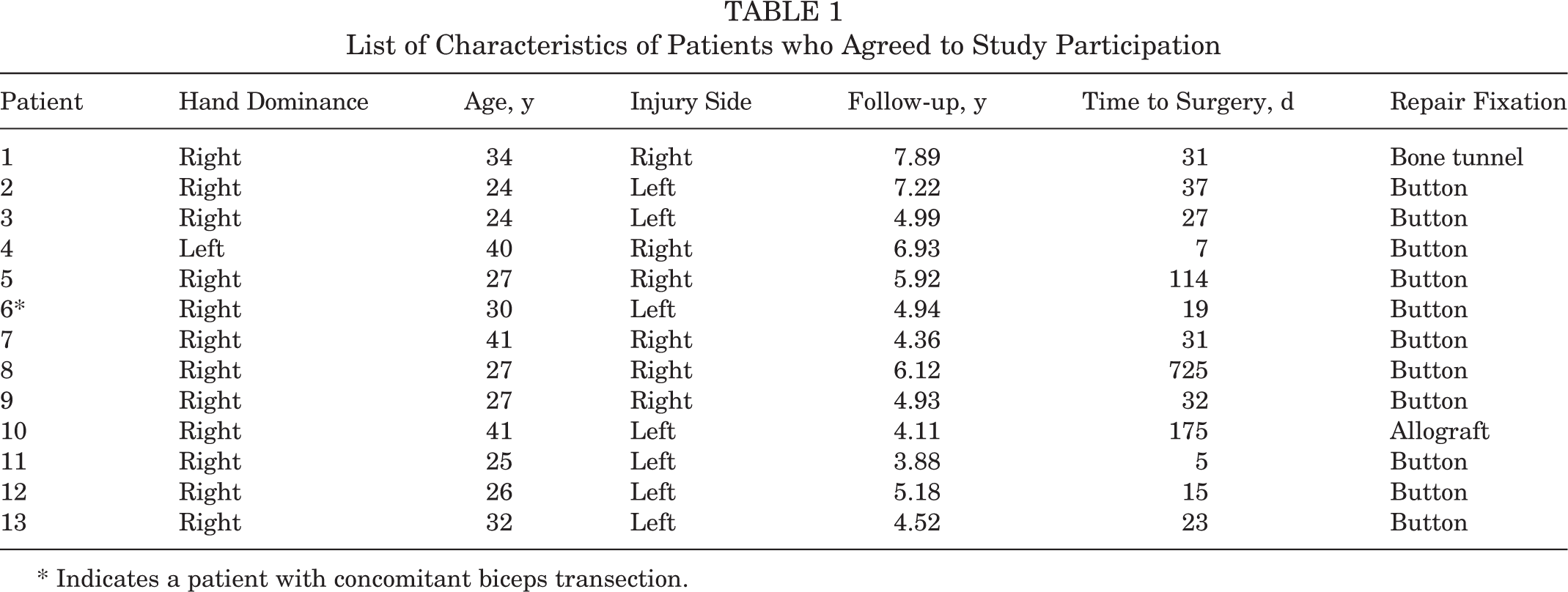
* Indicates a patient with concomitant biceps transection.
Summary of Overall Cohort Variables

Operative data indicated that the tear was isolated to the sternal head of the PM in 5 patients, with the remaining 8 patients having complete tears involving both the sternal and clavicular heads. Tears consisted of avulsions off the humerus (n = 8), intratendinous tears (n = 4), and musculotendinous tears (n = 1). Patients were treated almost exclusively with primary repair using intraosseous button fixation, with the exception of 2 patients: 1 primary repair through bone tunnels and 1 allograft augmentation fixated with intraosseous button fixation in a patient treated more than 6 weeks from injury (Table 1). One patient had a concomitant biceps transection involving both heads that was primarily repaired (patient 6 in Table 1).
Return to duty was reported in 100% of patients at a mean of 6 ± 3.24 months (range, 3-12 months) after injury. Regarding return to preinjury activity function, 5 patients (38.5%) indicated that they were unable to return to functional status, with the remaining patients returning at a mean of 6 ± 2.27 months. Specific functional performance in bench press and push-up is summarized in Table 2. Overall, patients rated their overall function as excellent (n = 6), good (n = 1), average (n = 5), and poor (n = 1), with 6 patients indicating they were very satisfied with their outcome, 6 satisfied, and 1 unsatisfied. Six patients (46.2%) indicated that they had no functional limitations, and 4 indicated some difficulty with weight lifting (bench press, n = 1; shoulder press, n = 2; limited poundage, n = 1). Pain evaluation indicated that 61.5% (n = 8) of patients reported no pain during routine activity, 30.8% reported mild, and 7.7% reported moderate pain. During strenuous activity, 46.2% of patients indicated no pain, while 46.2% indicated mild to moderate pain, and 7.7% indicated severe pain. One patient experienced reoperation (patient 6) for a painful scar and was treated with a scar revision and removal of suture used for the initial biceps primary repair. Three patients with pectoralis asymmetry (all chronic injuries) had additional complications that did not warrant additional treatment, and 5 patients reported cosmetic complaints regarding the surgical incision.
Overall, there were 10 patients in the immediate repair group, with repair performed at a mean of 22.7 days after injury (95% CI, 15.54 to 29.85 days), and 3 patients in the delayed repair group, with repair performed at a mean of 338.0 days after injury (95% CI, -42.8 to 718.8 days). The difference between groups in time to repair was significant (P = .006). We reported mean values and 95% CIs rather than median time to surgery, so as not to underreport the substantial variation in time to surgery among study participants. A summary of functional outcome data points according to acuity of repair is provided in Table 3.
Summary of Functional Outcome Measures for Included Patients, Subdivided According to Timing of Surgical Repair a
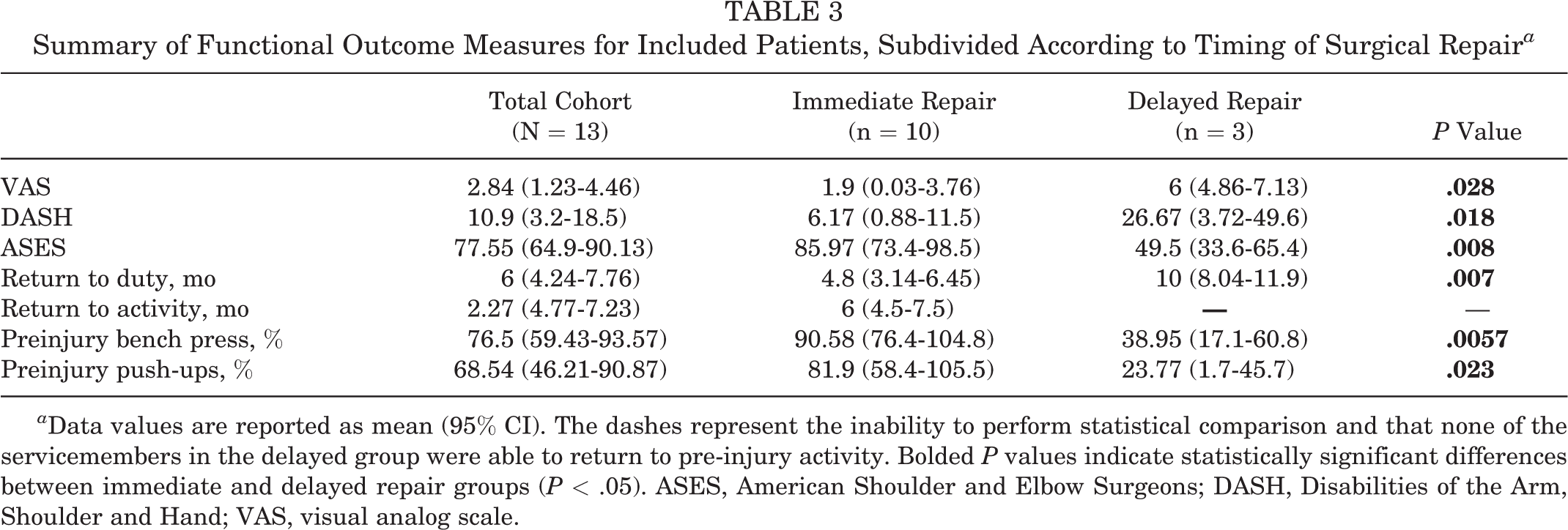
a Data values are reported as mean (95% CI). The dashes represent the inability to perform statistical comparison and that none of the servicemembers in the delayed group were able to return to pre-injury activity. Bolded P values indicate statistically significant differences between immediate and delayed repair groups (P < .05). ASES, American Shoulder and Elbow Surgeons; DASH, Disabilities of the Arm, Shoulder and Hand; VAS, visual analog scale.
Compared with the delayed repair group, patients in the immediate repair group had statistically superior strength performance as defined by percentage of preinjury bench press and push-up performance. Additionally, the patients in the immediate repair cohort had significantly lower VAS pain scores (mean difference, 4.1; MCID, 1.3 points) and greater function as rated with the DASH (mean difference, 20.49 points; MCID, 10.8 points) and ASES scores (mean difference, 36.4 points; MCID, 17 points). Differences in the functional outcome between the groups all surpassed the defined MCID.
Discussion
In the current study, we evaluated a series of PM tears occurring from a unique injury mechanism in military patients participating in airborne operations. All patients treated with operative repair of PM tears returned to military duty at a mean of 6 months from injury. Patient-reported satisfaction levels were high, with 12 of 13 patients rating their function as excellent, good, or average. Patients undergoing surgery within 6 weeks of injury demonstrated superior functional outcomes and recovery of strength in comparison with delayed repairs beyond 5 weeks from injury. Overall, 5 patients did not return to the same functional status after surgery, mixed between the 3 chronic repairs and 2 immediate repairs.
To our knowledge, this study represents the first series in the literature of PM tendon tears occurring secondary to parachute-induced mechanisms. Several previous case reports have identified this injury mechanism in individuals participating in military airborne operations. 15,17,24 McIntire et al 17 reported on a soldier who sustained a traumatic PM tear while exiting an aircraft during basic airborne training. Similarly, Kömürcü et al 15 described the injury in a paratrooper who became entangled in his parachute risers. A variety of other parachute-related shoulder injuries have also been described, including intrasubstance biceps brachii rupture, 30 conjoined tendon transection, 11 open humeral shaft fracture, 19 and glenohumeral fracture-dislocation. 8
Despite significant improvements in parachute technology, aircraft exiting, and landing techniques, injuries remain very common at a rate of 6 to 8 per 1,000 jumps. 8,12 Injury rates may be even higher in the presence of risk factors such as higher wind speed, night jumps, female sex, heavier equipment, decreased airborne experience, and increased numbers of jumpers. 13 Static line airborne operations were initially developed during World War II as a means of deploying large numbers of soldiers from an aircraft as safely and efficiently as possible. 14 With a static line jump, a cord is attached from the aircraft to the parachutist’s bag. As the individual exits the aircraft, the static line becomes taut and then quickly deploys the canopy. The rapid tensioning of the static line and the risers (suspension lines) as the canopy inflates may violently abduct and externally rotate the arm if not secured against the body (see Figure 1). This leads to an array of potential upper extremity injuries, including PM tears. Craig and Lee 7 reported that 33% of parachute injuries at altitude resulted from static line entanglement and 46% resulted from riser entanglement.
In previous studies, military members have been well-described as an at-risk population for PM tears. 2,3,20,21,29 While the overwhelming majority of PM tears occur due to weight lifting, a variety of other less common injury mechanisms have been described to include contact sports, 6 rappelling, 28 combat training, 25 rugby, 22 and high-intensity interval training. 23 Operative treatment is most commonly recommended, as these injuries usually occur in fit, active, younger patients with high-demand activity and job requirements.
Functional outcomes and return to military duty rates after this surgery are excellent and in line with findings of large nonmilitary outcomes studies. 4,31 Nute et al 20 reported a 94% return to full duty rate and 5.4% reoperation rate in a large study of 257 military patients, while Balazs et al 3 reported a 95.3% return to full duty rate in a study of 214 military patients. We observed a similar trend in this study, with all 13 patients returning to full duty at a mean of 6 months after injury and only 1 patient indicating he was not satisfied. While return to duty rates are high, consistent return to preinjury functional levels is not guaranteed. Yu et al 31 reported that 74% of patients returned to preinjury levels of sport. Liu et al 16 identified a lower rate with 50% returning to preinjury sport intensity and significant decreases in pectoralis strength. In the current study, both acute and chronic repairs still resulted in some postoperative residual pain, functional deficit, and loss of strength, as measured by bench press and push-ups. However, this effect was magnified in the chronic versus acute repairs. This finding was statistically significant and met the MCID for VAS, DASH, and ASES scores.
Multiple previous studies have concluded that acute repairs are associated with better functional outcomes; however, these studies are also generally small and retrospective and lack standardization. 1,2,18 As such, the ideal timing for PM repair has not been clearly elucidated. In a large recent meta-analysis of 20 articles with 384 patients, Bodendorfer et al 5 reported that functional outcomes and cosmetic satisfaction were significantly superior in acute versus chronic repairs. However, Gupton and Johnson 10 reported no differences between acute and chronic repairs in another similar study of 259 patients. Our findings would support previous studies in that acute repair resulted in better functional outcomes and return of strength than chronic repair in an active, young, high-demand population.
This study has multiple limitations. This is a small, retrospective case series with a limited sample size because of the uncommon nature of this specific injury mechanism. The study may be limited by response bias, as only 13 of 25 patients were willing to participate in the study and complete final questionnaires. The majority of patients were treated by direct repair with unicortical button fixation. However, the population included 1 patient treated with bone tunnel fixation and another chronic injury that at 175 days from injury required allograft augmentation. There is a risk of recall bias for reported proxy’s strength measures (bench press and push-up). Additionally, this study did not include objective strength measures and also involved a high-demand military population; as such, findings may not necessarily be applicable to nonmilitary and athletic populations. The study's strengths include the improved identification of a unique injury mechanism for PM tears in individuals participating in static line parachuting, and all patients were treated at a single military medical institution with colocated airborne operations.
Conclusion
Operative repair of parachute-induced PM tears within 5 weeks of injury provided superior functional and strength recovery when compared with delayed surgical repair. Strength performance was within a mean of 10% of preinjury performance for patients undergoing repair within 5 weeks of injury, indicating that these injuries may have a less deleterious impact on strength performance compared with PM tears caused by eccentric loading mechanisms. Acute repair should be considered for military servicemembers who experience this unique injury mechanism.
Footnotes
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of Defense or the U.S. Government. The authors are employees of the U.S. government. This work was prepared as part of their official duties, and as such there is no copyright to be transferred.
Submitted December 4, 2020; accepted February 9, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: I.J.A. has received nonconsulting fees from Arthrex, Exactech, and Smith & Nephew. S.A.P. has received consulting fees from Arthrex and Exactech and research support from Exactech. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Regional Health Command Atlantic Institutional Review Board (RHCA18022_916745).