
Abstract
Background:
Pectoralis major repair (PMR) is an infrequent injury that occurs during resistance training, most commonly during the eccentric phase of muscle contraction. As the incidence of weight training continues to increase, it is important to understand the outcomes after PMR.
Purpose:
To evaluate the rate and duration of return to work in patients undergoing PMR.
Study Design:
Case series; Level of evidence, 4.
Methods:
Consecutive patients undergoing PMR from 2010 to 2016 at a single institution were retrospectively reviewed at a minimum of 1 year postoperatively. Patients completed a standardized and validated work questionnaire, as well as a visual analog scale for pain, American Shoulder and Elbow Surgeons survey, Single Assessment Numerical Evaluation, and a satisfaction survey.
Results:
Of the 60 eligible patients who had a PMR, 49 (81.7%) were contacted at the final follow-up. Of the 49 patients, 46 (93.9%) had been employed within 3 years before surgery (mean ± SD age, 40.4 ± 8.2 years; follow-up, 3.9 ± 2.8 years). Of these, 45 (97.8%) returned to work by 1.6 ± 2.1 months postoperatively, and 41 (89.1%) returned to the same level of occupational intensity. Patients who held sedentary, light-, medium-, or high-intensity occupations returned to work at a rate of 100.0%, 100.0%, 83.3%, and 66.7% by 0.8 ± 1.0, 0.8 ± 1.0, 1.3 ± 2.7, and 3.3 ± 2.7 months, respectively. Five of 6 patients (83.3%) with workers’ compensation returned to their previous occupations by 5.0 ± 1.6 months, while 100% of those without workers’ compensation returned to work by 1.1 ± 1.7 months (P < .001). Overall, 44 patients (95.7%) were satisfied with the procedure, and 40 (87.0%) would have the operation again if presented the opportunity. A single patient (2.2%) required revision PMR.
Conclusion:
Approximately 98% of patients who underwent PMR returned to work by 1.6 ± 2.1 months postoperatively. Patients with higher-intensity occupations took longer to return to their preoperative levels of occupational intensity. Information regarding return to work is imperative in preoperative patient consultation to manage expectations.
Keywords
Pectoralis major tendon ruptures are an infrequent injury; however, the incidence thereof has become increasingly prevalent over the past 30 years. 1,15,16,21,27,40,43,48 Among military personnel, pectoralis major tendon tears occur at an incidence of 6 cases per 100,000 person-years. 23 Injury to the pectoralis major tendon typically occurs during resistance training, most commonly during the eccentric phase of muscle contraction during weight lifting. 1,15,22,25,27,33,39,48 Recreational resistance training is practiced by approximately 45 million adults in the United States, with approximately 20% of adults aged 18 to 65 years participating in weight lifting at least twice a week. 13 Given the increasing prevalence of weight training and pectoralis major tendon ruptures, it is imperative to understand outcomes after management of these injuries.
Despite a complication rate of 14%, including a rerupture rate of 3%, pectoralis major tendon repair provides superior improvement in functional outcomes and isometric and isokinetic strength as well as satisfaction with cosmesis in comparison with nonoperative management. 11 In a systematic review, Bodendorfer et al 11 identified the most common complications after pectoralis major repair (PMR) to be rerupture, persistent pain, and the need for additional surgery. Although not identified, the most common cause of reinjury is likely due to eccentric contraction of the pectoralis major. The Bak criteria have traditionally been used to assess outcomes after PMR. 8 This metric assesses patients with respect to percentage loss of isokinetic strength in comparison with preoperative status or contralateral limb, pain, cosmesis, and return to sport. However, the Bak criteria are limited because of variability in sport involvement; further, strength assessment is biased by limb dominance, and it may not be feasible to perform in the clinical setting. 8
Operative management is efficacious, particularly in the acute setting, as tendon ruptures typically occur at the musculotendinous junction or tendinous insertion, which are amenable to anatomic repair. 12,26 Patients demonstrate improvements in patient-reported outcomes measures and strength after PMR. 11,12 However, patient-reported outcome measures may not indicate clinical significance in young active patients. Liu et al 31 reported that 97.7% of patients were able to return to sport by 7.7 months postoperatively. Furthermore, 94% of military members returned to duty by 7.1 months. 34 Despite favorable outcomes, return to work is an important outcome metric in young active patients, who comprise the majority of the workforce. However, information regarding return to work is limited in patients undergoing PMR.
The purpose of this investigation was to assess the rate and duration of return to work after PMR. We hypothesized that patients with higher-intensity occupations would demonstrate a lower rate of return to their previous levels of work intensity, with a longer duration of absence, in comparison with patients with lower-intensity occupations.
Methods
This was a retrospective analysis of prospectively collected data on consecutive patients who underwent PMR from 2010 to 2016 at our institution. Before the initiation of this investigation, institutional review board approval was obtained. Indications for operative management included pectoralis major tendon tears in young active patients as well as high-level athletes. Inclusion criteria for this study were a PMR, age of at least 18 years at the time of surgery, and availability for minimum 1-year follow-up. Patients were excluded if they had complex concomitant injuries or procedures. Patients who underwent previous shoulder surgery or PMR were included in the analysis.
Patients were contacted via telephone or email to complete a survey regarding satisfaction and work outcomes. As part of the survey, patients completed the American Shoulder and Elbow Surgeons (ASES) survey, Single Assessment Numerical Evaluation (SANE), and visual analog scale for pain. ASES and SANE scores were collected preoperatively as well as at the final follow-up. This work questionnaire has been administered to describe outcomes after orthopaedic procedures. 2 –6,17 –20,24,28 –30,38 Occupational intensity was divided into high, medium, low, or sedentary occupations based on the US Department of Labor classification (Table 1). 2 –6,16 –19,23,27 –29,37 Patient records were reviewed to identify preoperative diagnosis, injury characteristics, operative details, characteristic information, preoperative radiographs, complications, and surgical history. Pectoralis major tendon tears were classified using the Tietjen classification. 46
Categorization of Work by Demand

a All physical demand requirements are in excess of the previous level.
bOccasionally, activity or condition exists up to one-third of the time; frequently, activity or condition exists one-third to two-thirds of the time; constantly, activity or condition exists two-thirds to most of the time.
Surgical Techniques
With the patient in a modified beach-chair position, an extended subpectoral incision was made. The clavicular and sternal heads of the pectoralis major tendon were identified and traced to their tendinous insertion within the bicipital groove. The insertion site was debrided to facilitate implant insertion. Double-loaded EndoButton (Pec Button; Arthrex) or double-loaded suture anchor (SutureFix; Smith & Nephew) was primarily used for fixation. Between 1 and 4 implants were used in each case. Each implant was placed approximately 2 cm apart and were loaded with No. 2 or No. 5 suture or suture tape (FiberWire, FiberTape [Arthrex]; Cobraid [Smith & Nephew]). The interval between the short head of the biceps tendon and clavicular head of the pectoralis major tendon on the coracoid process was identified and exposed to visualize the rupture site. The pectoralis major tendon stump was stitched with a running mattress or Krackow stitch and subsequently tied to create an anatomic reduction.
Rehabilitation Protocol
After PMR, patients were placed in a sling and instructed to limit shoulder range of motion for the first 2 weeks. Between 2 and 6 weeks, patients were allowed to begin passive range of motion. At 6 weeks, patients could discontinue the sling, begin active and active-assist range of motion, and restore full passive range of motion without restriction. At 12 weeks postoperatively, patients were allowed to progress with strengthening of the shoulder. Patients were permitted to resume full strengthening activities at 6 months postoperatively.
Statistical Analysis
Descriptive analysis of continuous variables included means and standard deviations, while frequencies and percentages were used to report discrete variables. Chi-square analysis and analysis of variance were used to compare rate and duration of return to work across occupational intensities. A stepwise, binomial logistic regression was performed to assess the effect of characteristic and surgical variables on the likelihood of return to work to the preoperative level of occupational activity, while a multivariate linear regression was used to assess predictive factors of the duration until patients were able to return to work. Statistical comparisons were considered significant at P ≤ .05. Statistical analyses were performed using RStudio software (Version 1.0.143; R Foundation for Statistical Computing).
Results
Patient Characteristics
Sixty patients underwent PMR without other major concomitant procedures from 2010 to 2016. Eleven patients were lost to follow-up, leaving 49 (81.7%) eligible for inclusion in this investigation. Of these 49 patients, 46 (93.9%) were employed within 3 years of surgery and included in this analysis. Patient characteristics are provided in Table 2.
Patient Characteristics (N = 46)

This was the initial surgery in 37 patients (80.4%); for the remaining patients, previous surgery included PMR (n = 4; 8.7%), rotator cuff repair (n = 2; 4.3%), or arthroscopic debridement (n = 1; 2.2%). Six patients (13.0%) had previous surgery on the contralateral shoulder: 3 (8.1%) PMRs, 2 (4.3%) rotator cuff repairs, and 1 (2.2%) biceps tenodesis. Patients with previous pectoralis major tendon repair had undergone the initial procedure by an outside physician >1 year before the current revision surgery. Injuries occurred during weight lifting (n = 29; 63.0%), sporting activity (n = 9; 19.6%), work-related incident (n = 5; 10.9%), or an accident (n = 3; 6.5%). Three patients (6.5%) required allograft supplementation of the repair, and 1 (2.2%) had plasma-rich protein supplementation. These patients with allograft or platelet-rich plasma supplementation had a chronic tendon tear, except 1 patient who underwent revision surgery and necessitated allograft supplementation of the repair. Injury and operative details are provided in Table 3. There was no correlation between duration of injury and length of retraction (r = 0.59).
Injury and Operative Details
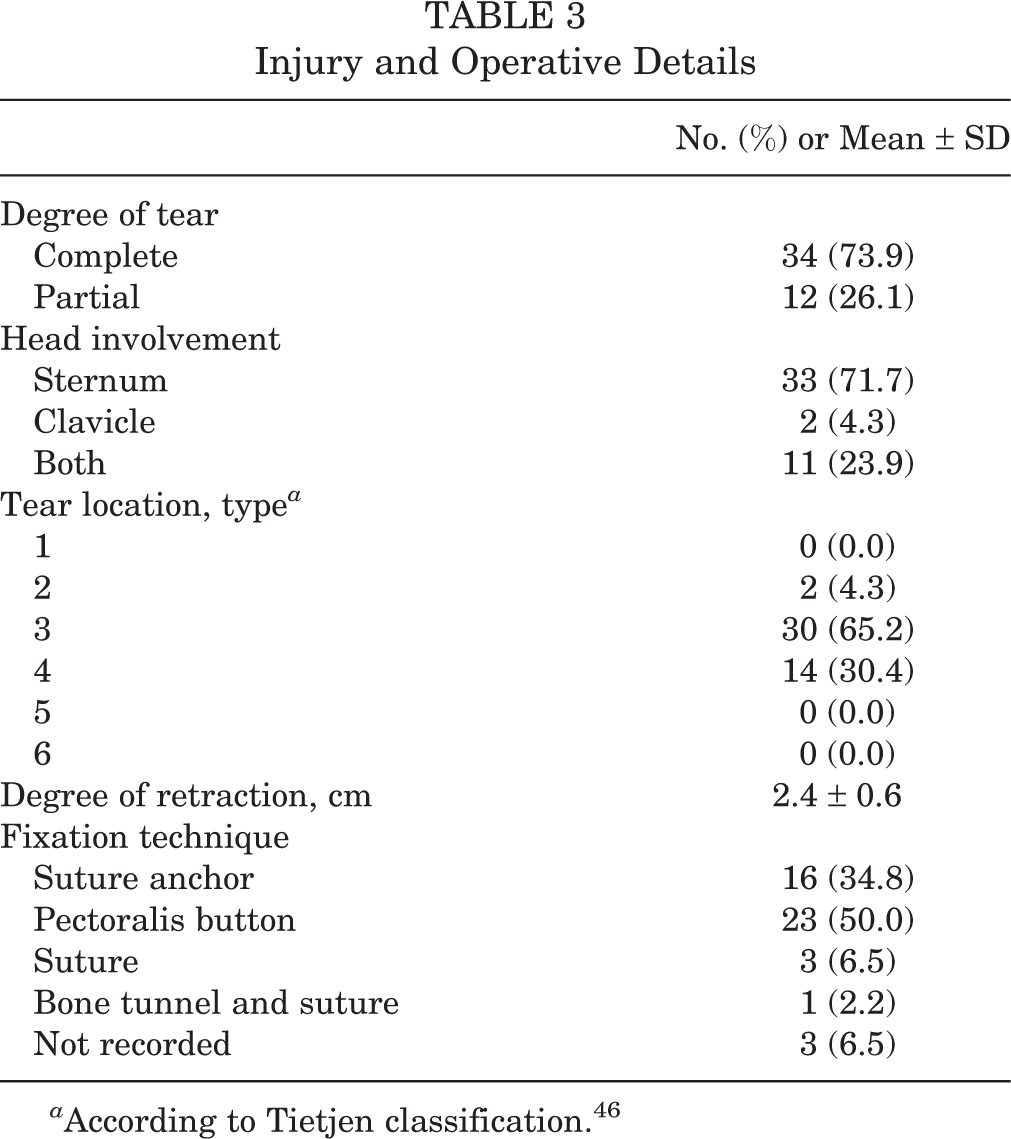
a According to Tietjen classification. 46
Return to Work
Overall, 45 patients (97.8%) returned to work at a mean 1.6 ± 2.1 months after PMR, and 41 (89.1%) returned to their previous levels of occupational intensity. A single patient (2.2%) who was unable to return to the previous level of occupation received disability payments. Six patients (13.0%) were covered by workers’ compensation; of these, 5 (83.3%) were able to return to their previous occupations by 5.0 ± 1.6 months postoperatively. Comparatively, 100% of patients (40/40) with non–workers’ compensation designation returned to work by 1.1 ± 1.7 months (P < .001). Every patient (4/4) who had previous PMR on the ipsilateral shoulder returned to work by 3.1 ± 2.5 months after surgery. A patient who had previous PMR held a heavy-intensity occupation and returned to work 6 months postoperatively.
Patients who held sedentary, light-, moderate-, or heavy-intensity occupations were able to return to their previous levels of occupational intensity at rates of 100.0%, 100.0%, 83.3%, and 66.7% at a duration of 0.8 ± 1.0, 0.8 ± 1.0, 1.3 ± 2.7, and 3.3 ± 2.7 months, respectively (Table 4). There was no difference in the rate of return to work among occupational intensities (P = .1); however, patients with higher-intensity occupations took longer to return to work than those with lower-intensity occupations (P = .01).
Return to Work to the Same Level of Occupational Intensity

a Mean ± SD.
On stepwise multivariate binomial logistic analysis, complete tendon tear (odds ratio [OR], 0.57 [95% CI, 0.47-0.69]; P = .002), length of retraction (OR, 0.95 [95% CI, 0.93-0.97]; P = .008), and higher occupational intensity (OR, 0.81 [95% CI, 0.76-0.86]; P = .001) were associated with a significantly decreased likelihood of returning to work at the same intensity. Younger age (OR, 1.02 [95% CI, 1.01-1.02]; P = .006) and surgery on the dominant extremity (OR, 1.31 [95% CI, 1.15-1.51]; P = .01) were associated with a greater likelihood of returning to work at the preoperative level of intensity. A multiple linear regression was calculated to predict duration of return to work based on characteristic and operative variables. Patients with partial tendon tears returned to work 3.93 months sooner than those with complete tears (95% CI, –6.75 to –1.1; P = .027). Patients with previous surgery (pectoralis or shoulder surgery) took 6.15 months longer to return to work (95% CI, 1.59-10.71; P = .028).
Postoperative Outcomes
Patients had statistically significant improvements in ASES (91.8 ± 14.2 vs 62.5 ± 23.0; P < .001) and SANE (89.3 ± 20.7 vs 38.9 ± 24.6; P < .001). At the final follow-up, 9 (19.6%) continued to report shoulder pain at night, and among the entire cohort, the mean score on the visual analog scale for pain was 1.3 ± 2.1. Six patients (13.0%) indicated taking acetaminophen or nonsteroidal anti-inflammatory medications to relieve their pain, while a single patient (2.2%) reported taking opioids for pain control. Forty-one patients (89.1%) noted at least “a little improvement” in their quality of life after PMR, while 44 (95.7%) were at least “satisfied” with the procedure, with 27 (61.4%) being “very satisfied.” Thirty-five patients (76.1%) were at least “satisfied” with the cosmetic appearance of the surgery, and 40 (87%) would still have the operation if presented the opportunity to alter their decision. Five patients (10.9%) returned to the operating room after surgery: 1 (2.2%), revision PMR; 2 (4.3%), an irrigation and debridement with removal of hardware; 1 (2.2%), rotator cuff repair; and 1 (2.2%), an unspecified shoulder procedure.
Discussion
In this study, we demonstrated that 97.8% of patients returned to work by 1.6 ± 2.1 months after PMR, with 89.1% returning to the same level of occupational intensity. Patients with higher-intensity occupations took significantly longer to return to work than those with lower-intensity occupations. Since PMR is commonly performed in younger active patients, who make up the majority of the workforce, it is important that patients be appropriately counseled regarding work outcomes.
Return to work is an important outcome metric after elective orthopaedic procedures because employment results in higher self-esteem and sense of purpose as well as overall improved mental health. 42,45 However, outcomes regarding return to work are limited in patients undergoing PMR. Among military personnel, 78% to 100% of patients were able to return to active duty, with the majority returning to active duty within 6 months of surgery. 7,34,35,37,41,44 In the present work, approximately 98% of patients returned to work; however, only 66.7% of those who had high-intensity occupations were able to return to that level. The military population differs significantly from the civilian population, as the result of its work culture of camaraderie and resilience. Furthermore, its continued employment is contingent upon physical well-being. 9 Additional factors, such as rank, station, branch, and military occupational specialty, may affect return to duty among military personnel. 31 Therefore, extrapolating findings among military service members to the general population may not be possible. In a systematic review, Yu et al 49 demonstrated that 95% of patients returned to work after PMR; however, 95% of the patients in this study were military members. 7,34 Nonetheless, in this investigation, 98% of patients were able to return to work by 1.6 months after PMR.
The relationship between occupational intensity and duration until return to work is likely multifactorial. The senior authors (G.P.N., B.F., N.N.V., and A.A.R.) implement a protocol of nonweightbearing and no range of motion for the first 2 weeks after surgery, after which patients are slowly allowed to perform active and active-assist range of motion at 6 weeks. This protocol may be favorable to patients with sedentary or light-intensity occupations, allowing return to work sooner than those with higher-intensity occupations. It is possible that the lack of statistical significance between the rate of return to work and occupational intensity may be due to low statistical power. Furthermore, patients with a workers’ compensation designation had a lower rate of return to work (83.3% vs 100%) and a longer duration until return (5.0 vs 1.1 months). It is important to note that these comparisons are limited because of the number of patients with a workers’ compensation designation in this study. However, patients with workers’ compensation have been shown to achieve lower clinically significant outcomes after biceps tenodesis, 32 rotator cuff repair, 10 and shoulder arthroplasty. 47 These patients may not experience greater subjective improvement and may have undocumented reasons for being unable to return to work after PMR. Preoperative patient expectations affect clinical outcomes 14,36 ; therefore, physicians should counsel patients regarding outcomes of return to work after PMR.
It is imperative that the present analysis be interpreted within the context of its limitations. The external validity of these results may be limited as the result of differences in patient characteristics or occupational demands. The inclusion of patients who had undergone previous shoulder surgery or PMR creates heterogeneity and may affect the results. More than half of the patients held sedentary or light-intensity occupations, which may alter the rate and duration of return to work. However, the rate and duration of return to work were calculated for each occupational intensity and demonstrated that those with higher-intensity occupations take longer to return to work than those with lighter occupational demands. This was a retrospective study, which contains inherent limitations, such as the inability to control for baseline characteristics, as well as the variability in surgical indications, technique, and rehabilitation protocols. The retrospective nature of this investigation subjects its results to selection bias. The follow-up is relatively short-term, and the impact of continued participation in work on patient outcomes is not well-understood. In addition, this study is subject to recall bias; however, its design is similar to previous investigations that assessed return to work and satisfaction after upper and lower extremity orthopaedic procedures. 2 –6,17 –20,24,28 –30,38 This study is also subject to nonresponse bias, as 18.3% of patients were lost to follow-up. Patients lost to follow-up may compose a different population than those retained in the study. The rationale for return to work was not investigated, which may be influenced by social situation, economic need, comorbidities, disability coverage, and health insurance coverage. Confounding variables, such as anabolic steroid use, were neither assessed nor controlled for. Furthermore, the results would be strengthened by inclusion of the Bak criteria; however, some of these data (ie, isokinetic strength) were not collected, and appropriate calculations could not be made.
Conclusion
Approximately 98% of patients who undergo PMR returned to work by 1.6 ± 2.1 months postoperatively. Patients took longer than that to return to their preoperative levels of occupational intensity. Information regarding return to work is imperative in preoperative patient consultation so as to manage expectations.
Footnotes
Final revision submitted June 7, 2021; accepted June 23, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.N.L. has received education payments from Arthrex and Smith & Nephew; nonconsulting payments from Smith & Nephew; and hospitality payments from Exactech, Stryker, and Wright Medical. G.H.G. has received education payments from Arthrex and Smith & Nephew and honoraria from Wright Medical. G.P.N. has received consulting fees from Tornier and Wright Medical; nonconsulting fees from Arthrosurface and Wright Medical; honoraria from Arthrosurface; and royalties from Arthrosurface, Innomed, and Wright Medical. B.F. has received research support from Arthrex and Stryker, fellowship support from Smith & Nephew and Ossur, education payments from Medwest, consulting fees from Stryker, and royalties from Elsevier and has stock/stock options in Jace Medical. A.A.R. has received research support from Aesculap/B. Braun, Arthrex, Histogenics, Medipost, NuTech, OrthoSpace, Smith & Nephew, and Zimmer and consulting and nonconsulting fees and royalties from Arthrex. N.N.V. has received research support from Arthrex, Arthrosurface, DJO, Ossur, Athletico, ConMed Linvatec, Miomed, and Mitek; consulting fees from Arthrex, Medacta, Minivasive, Orthospace, Smith & Nephew, and Stryker; nonconsulting fees from Arthrex; royalties from Arthroscopy, Smith & Nephew, and Vindico Medical-Orthopaedics Hyperguide; and hospitality payments from Relievant Medsystems. N.N.V. also has stock/stock options from Cymedica, Minivasive, and Omeros. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (ORA No. 18080809-IRB01).